(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a plenary prostate cancer session and a presentation by Dr. Markus Graefen discussing the optimal management of de-novo oligometastatic disease and that surgery is still an option in 2026. Dr. Graefen’s discussion was based on a prior case presentation of a 52 year old fit man with ISUP 5 oligometastatic prostate cancer (cT1cN0M1) on conventional imaging. Dr. Graefen notes that in this specific case, radical prostatectomy is not a reasonable option for several reasons:
- This is high volume metastatic hormone sensitive prostate cancer (mHSPC), and there is no data to support radical prostatectomy in this disease space
- Conventional imaging was used
- If such a patient suffers from lower urinary tract symptoms, a transurethral resection of the prostate would be indicated
However, in low volume mHSPC, the body of evidence is sufficient to offer selected patients radical prostatectomy for local treatment of the primary cancer. Dr. Graefen notes that many series have shown that radical prostatectomy is a safe option in oligometastatic HSPC patients, with the safety profile comparable to high-risk patients. Thus, this is “straight-forward” surgery with no additional surgical side effects based on the oligometastatic status itself. The published comparisons of radical prostatectomy and radiation therapy suffer from the bias that patients who underwent radical prostatectomy in oligometastatic HSPC are less locally advanced compared to patients in radiotherapy series.
In 2022, Dai and colleagues1 published the results of a phase 2 trial comparing ADT + local radiotherapy versus ADT alone for newly diagnosed oligometastatic prostate cancer (defined as five or fewer bone or extrapelvic lymph node metastases and no visceral metastases), and found that after a median follow-up of 48 months, the median radiographic progression free survival was not reached in the study group versus 40 months in the control group (HR 0.43, 95% CI 0.27-0.70; p = 0.001). Moreover, the 3-year overall survival rate was 88% for the study group and 70% for the control group (HR 0.44, 95% CI 0.24-0.81; p = 0.008):
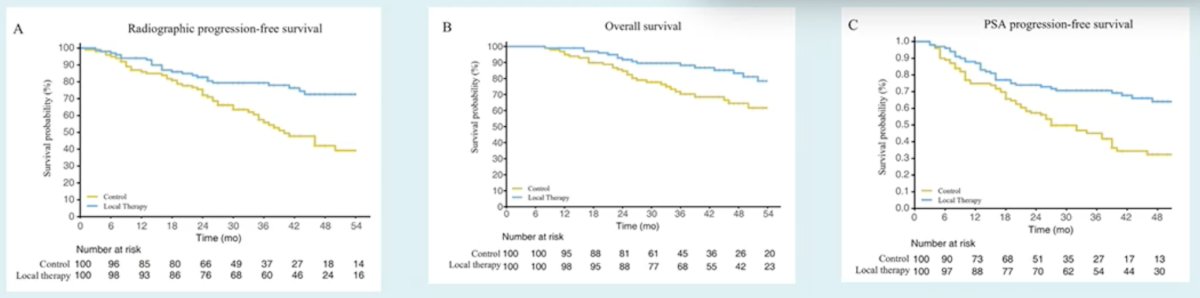
Radiotherapy clearly works in this patient population.
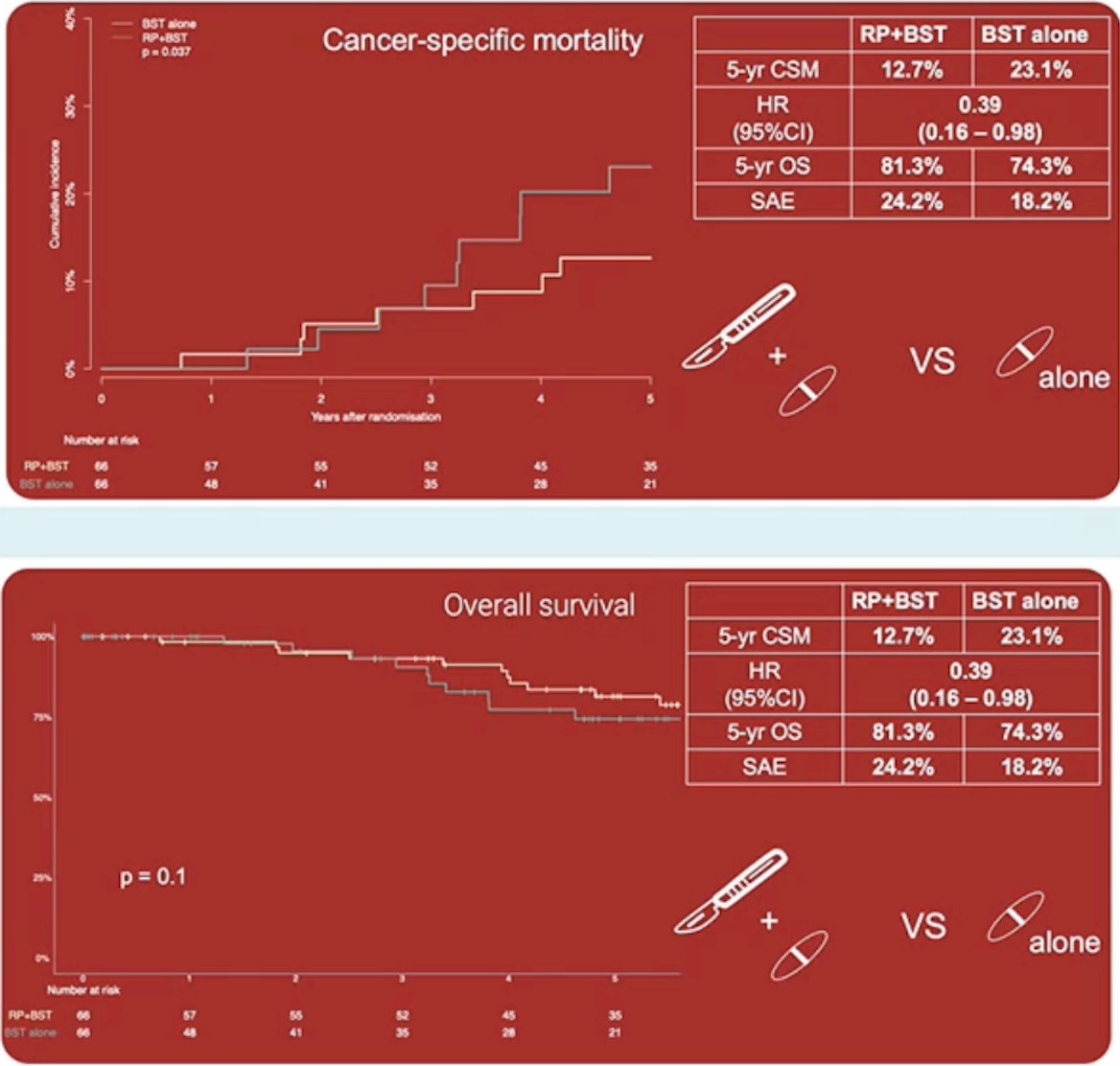
In 2025, Dr. Graefen and colleagues published the results of the RAMPP randomized clinical trial that compared best systemic therapy with or without radical prostatectomy in men with oligometastatic prostate cancer (defined as 1-5 bone metastases with or without nodal involvement).2 Among 132 randomized men, the 5-year cancer specific mortality cumulative incidence was 13% for radical prostatectomy + best systemic therapy versus 23% for best systemic therapy alone (p = 0.037), with a hazard ratio of 0.39 (95% CI 0.16-0.98; p = 0.045). The 5-year cumulative incidence of clinical progression, including cancer specific mortality, was 59% for radical prostatectomy + best systemic therapy versus 60% for best systemic therapy alone. Finally, the 5-year overall survival rate was 81% for radical prostatectomy + best systemic therapy versus 74% for best systemic therapy alone:
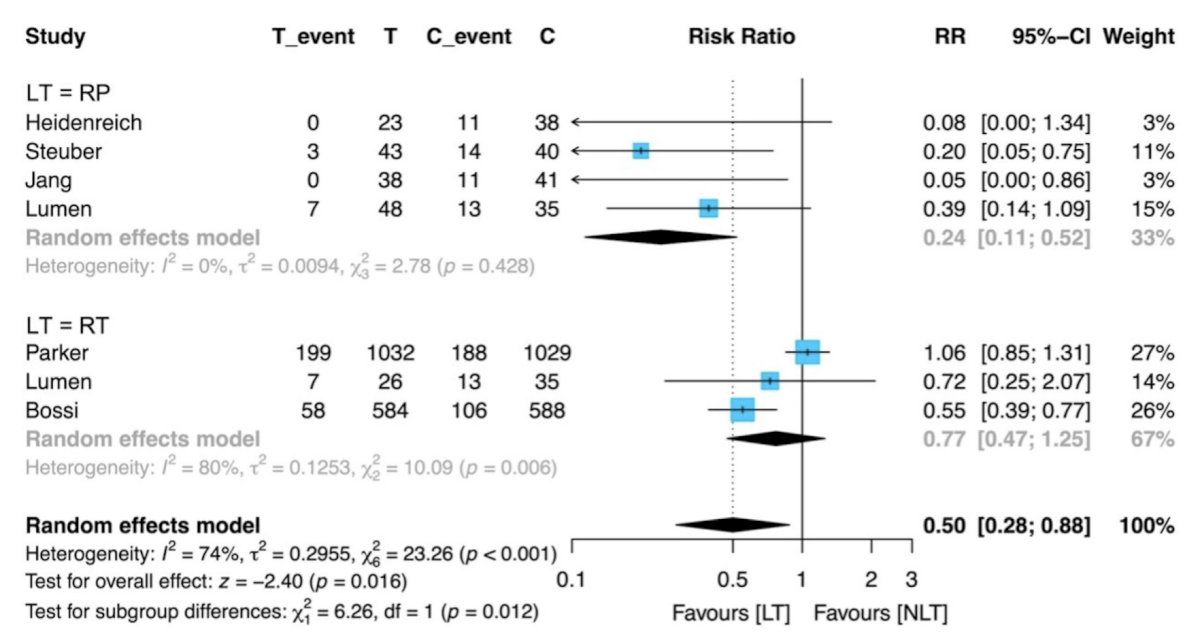
With regards to addressing local events due to primary cancer progression, Tsuboi et al.3 performed a systematic review and meta analysis assessing the impact of local therapies on local event suppression in mHSPC. Among 6 studies included in the analysis, the overall incidence of local events was significantly lower in the local treatment + systemic therapy group than in the systemic therapy only groups (RR 0.50, 95% CI 0.28-0.88, p = 0.016). Radical prostatectomy significantly reduced the incidence of overall local events (RR 0.24, 95% CI 0.11-0.52) and that of local events requiring surgical intervention (RR 0.08, 95% CI 0.03-0.25). Although there was no statistically significant difference between the radiotherapy + systemic therapy and systemic therapy only groups in terms of overall local events, the incidence of local events requiring surgical intervention was significantly lower in the radiotherapy + systemic therapy group (RR 0.70, 95% CI 0.49-0.99):
Dr. Graefen concluded his presentation discussing the optimal management of de-novo oligometastatic disease and that surgery is still an option in 2026 with the following take-home points:
- Radical prostatectomy is a safe option in oligometastatic HSPC
- The evidence for radiotherapy is clearly more solid, yet radical prostatectomy can be an option in selected patients after respective counseling
- A “good” patient is young with low metastatic burden, locally resectable disease, and with lower urinary tract symptoms
- It remains unclear if and to what degree local treatment improves outcomes in the era of modern systemic treatment
- Our typical concept is “all in” – combining systemic treatment, local treatment to the primary, and metastasis directed therapy
- Radical prostatectomy may improve the option for later treatment de-escalation
Presented by: Markus Graefen, MD, Martini-Klinik Prostate Cancer Center, Hamburg, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Dai B, Zhang S, Wan FN, et al. Combination of Androgen Deprivation Therapy with Radical Local Therapy versus Androgen Deprivation Therapy Alone for Newly Diagnosed Oligometastatic Prostate Cancer: A phase II Randomized Controlled Trial. Eur Urol Oncol. 2022 Oct;5(5):519-525.
- Graefen M, Falkenbach F, Maurer T, et al. Best Systemic Therapy with or without Radical Prostatectomy in Management of men with Oligometastatic Prostate Cancer: The RAMPP Randomized Controlled Trial. Eur Urol. 2025 Oct 3:S0302-2838(25)04687-1.
- Tsuboi I, Matsukawa A, Parizi MK, et al. A systematic review and meta-analysis of the impact of local therapies on local event suppression in metastatic hormone-sensitive prostate cancer. Eur Urol Oncol. 2024 Dec;7(6):1185-1194.