(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a plenary prostate cancer session and a presentation by Dr. Jozefina Casuscelli discussing the optimal management of de-novo oligometastatic disease and asserting that intensified systemic therapy is still mandatory. Dr. Casuscelli’s discussion was based on a prior case presentation of a 52 year old fit man with ISUP 5 oligometastatic prostate cancer (cT1cN0M1) on conventional imaging. Currently, there is no standardized definition for oligometastatic prostate cancer, and it has historically been based on the CHAARTED low volume status. Moreover, oligometastatic prostate cancer has been based on conventional CT + bone scan imaging: there have been no phase 3 trials incorporating molecular imaging, and no biomarkers distinguishing true oligometastatic from early polymetastatic disease. What we see as oligometastatic disease may represent systemic disease biologically.
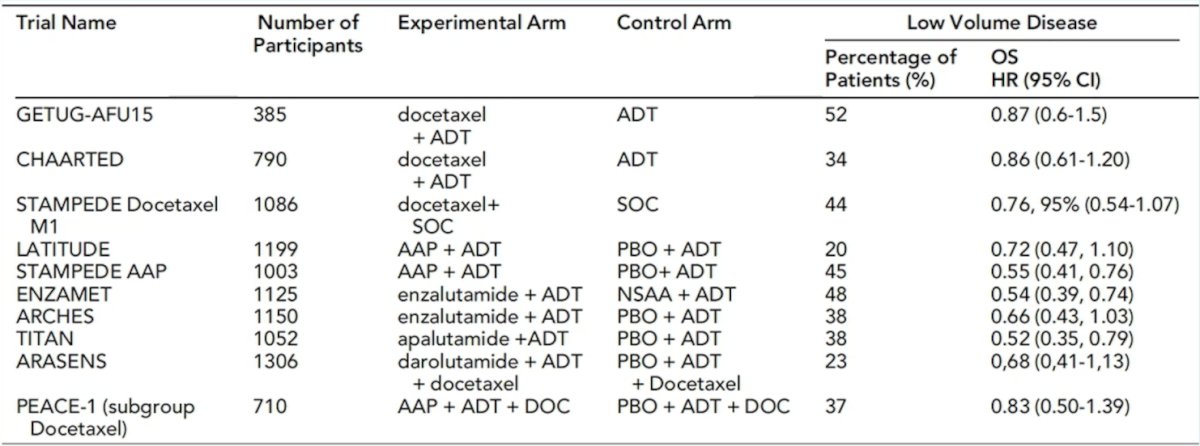
Dr. Casuscelli notes that data for metastasis directed therapy alone is promising, but to date, there is no overall survival benefit. Importantly, metastasis directed therapy treats all of the visible lesions, but not occult systemic clones; thus, metastasis directed therapy may complement, but cannot replace systemic therapy. Systemic intensification improves overall survival, with evidence coming from many large randomized phase III trials:
Dr. Casuscelli emphasized that systemic therapy is mandatory, but we must refine it. Standard of care is ADT + an androgen receptor pathway inhibitor, however:
- The definitions are outdated (CT/bone scan based)
- PSMA PET changes staging dramatically
- There are no trials stratified by molecular imaging
- There is an unknown optimal duration of intensified ADT
What we need are oligometastatic prostate cancer specific prospective trials and integration of PSMA PET/CT, in addition to biomarker guided risk stratification. These studies should address who truly needs long-term ADT and who we can safely de-escalate.
Dr. Casuscelli concluded her presentation discussing the optimal management of de-novo oligometastatic disease and that intensified systemic therapy is still mandatory, with the following take-home points for this patient case:
- This patient should have immediate systemic intensification with ADT + androgen receptor pathway inhibitor based on a proven overall survival benefit in low volume mHSPC
- This patient may benefit from prostate radiotherapy based on an overall survival benefit in low-volume M1 disease from the STAMPEDE trial [1]
- This patient should be considered for metastasis directed therapy to the bone lesions, but not as a replacement for systemic therapy
- This patient should receive a PSMA PET/CT scan and a discussion regarding the potential benefit of germline + somatic testing, as well as clinical trial participation
Presented by: Jozefina Casuscelli, MD, LMU University Hospital, Munich, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References: