(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., between March 13th and 16th 2026, was host to the BCG meets immunotherapy in high-risk NMIBC: Key lessons for urologists from POTOMAC, ALBAN, and CREST Thematic Session. Dr. Neal D. Shore presented Highlights from the CREST Trial — Sasanlimab + BCG (a positive trial).
Dr. Shore began by noting that these three trials were largely led by urologists, which is notable in a field where large randomized trials are often conducted by medical oncologists. He emphasized that prior to these studies, there had been very limited randomized data evaluating checkpoint inhibitors in BCG-naïve patients with HR-NMIBC. Importantly, all three trials were conducted during the COVID-19 pandemic, adding additional logistical challenges to patient enrollment and trial execution.
Dr. Shore then reviewed the CREST study design, noting that the overall design of these trials is largely similar, particularly when comparing CREST with POTOMAC. The CREST study (NCT04165317) enrolled patients with BCG-naïve HR-NMIBC, including T1 disease, high-grade Ta, or CIS. Patients with prior exposure to PD-1, PD-L1, CTLA-4 inhibitors, or other immunostimulatory agents were excluded. A total of 1,055 patients were randomized in a 1:1:1 ratio and stratified according to the presence of CIS and geographic region.
The CREST trial included three treatment arms. Arm A evaluated sasanlimab administered subcutaneously in combination with BCG induction and maintenance (I+M). Arm B included sasanlimab combined with BCG induction only, without maintenance. Arm C served as the control arm and consisted of standard BCG induction plus maintenance therapy. BCG induction consisted of six instillations, followed by maintenance therapy for up to two years, while sasanlimab was administered for up to 25 four-week cycles.
The primary endpoint compared Arm A versus Arm C and was event-free survival (EFS), defined as recurrence of high-grade disease, disease progression, persistence of CIS, or death from any cause.1 The study design is shown below:
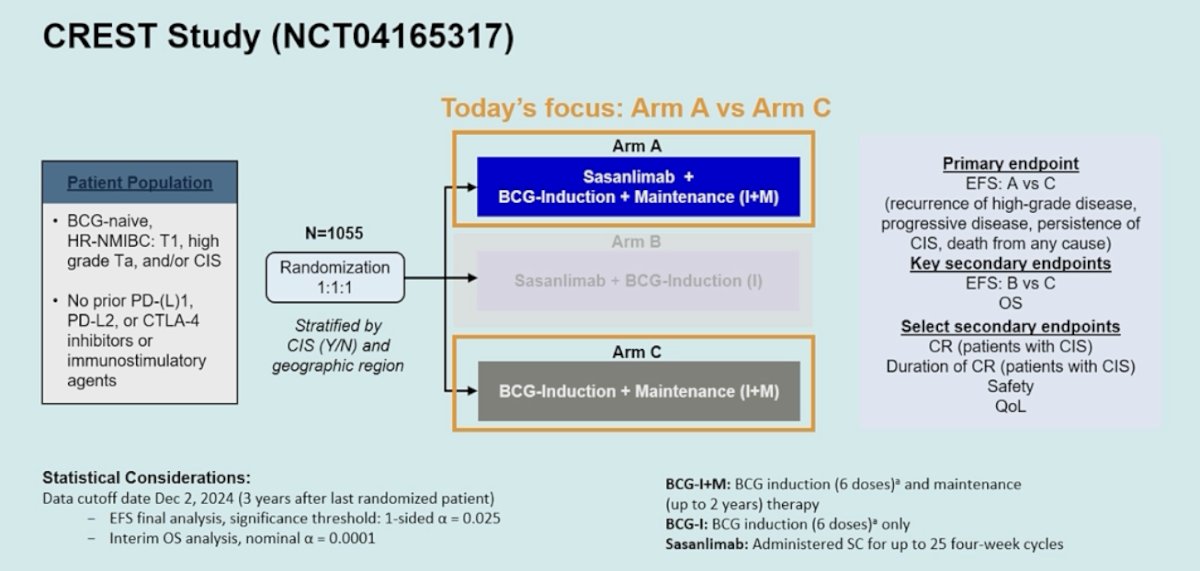
The study had broad international participation, with patients enrolled from the United States, Western Europe/Canada, and other regions, reflecting the global distribution of the trial. He also emphasized key practical aspects of the study design. Sasanlimab was administered subcutaneously, which differs from the intravenous administration used in other checkpoint inhibitor trials in this setting. In addition, patients in both arms received standard BCG induction followed by maintenance BCG, consistent with contemporary standard-of-care treatment.
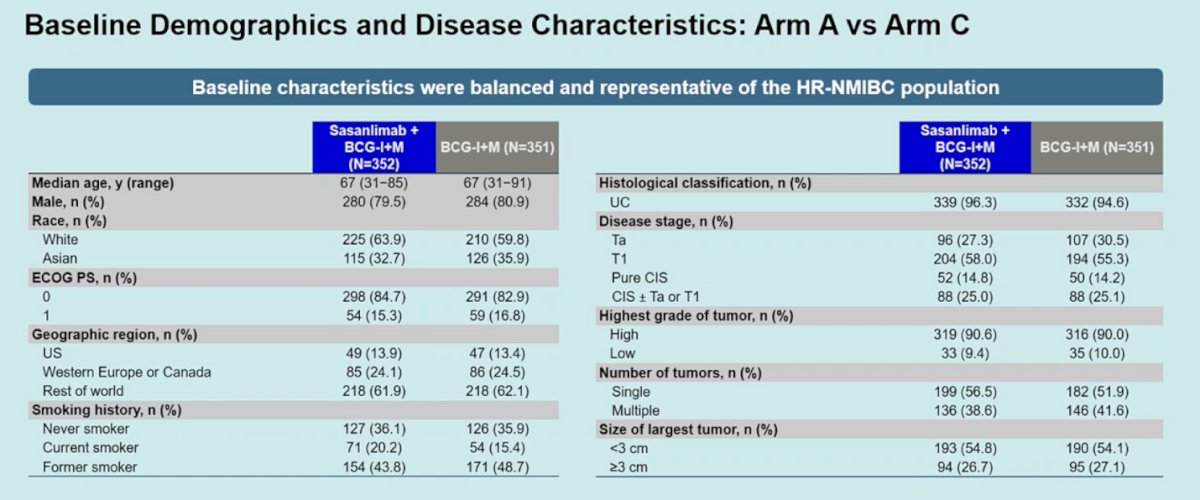
Baseline characteristics were balanced and representative of the HR-NMIBC population. Most tumors were urothelial carcinoma (>94%), and T1 disease represented the largest subgroup, present in about 55–58% of patients. Pure CIS was reported in roughly 14–15% of patients, slightly higher than in POTOMAC, while approximately one quarter had CIS with concomitant Ta or T1 disease. High-grade tumors were present in about 90% of cases, and nearly 40% of patients had multiple tumors.
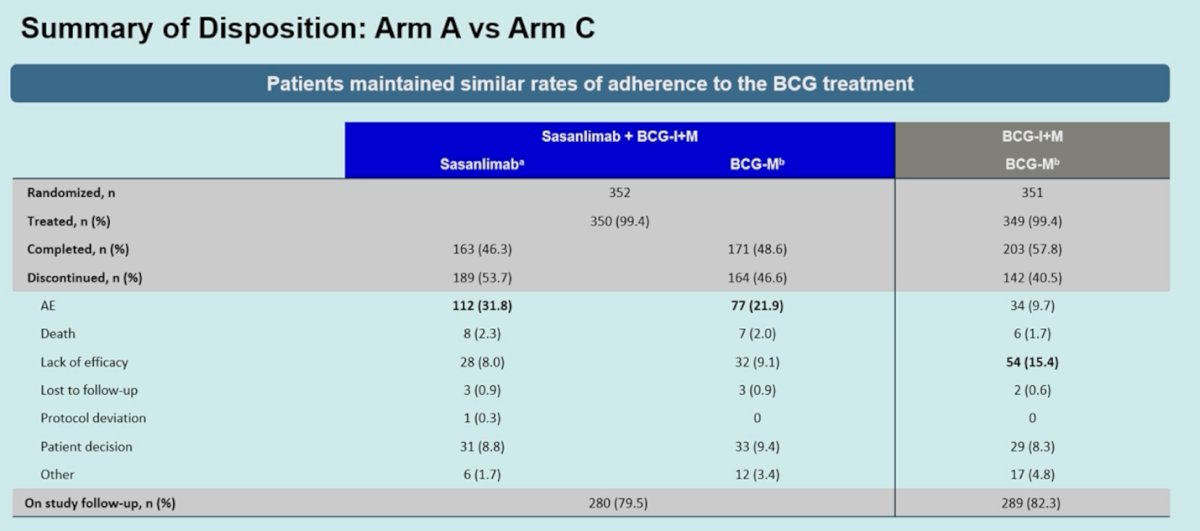
Dr. Shore highlighted that the addition of an immuno-oncology agent did not compromise adherence to BCG therapy. Rates of BCG administration were similar between the two arms, indicating that adding sasanlimab did not reduce the likelihood of patients receiving induction and maintenance BCG. He also placed these findings in the context of real-world practice, noting that most patients do not complete the full planned duration of BCG therapy. Even in the SWOG trial, only about 17% of patients were able to receive the full three years of maintenance BCG.
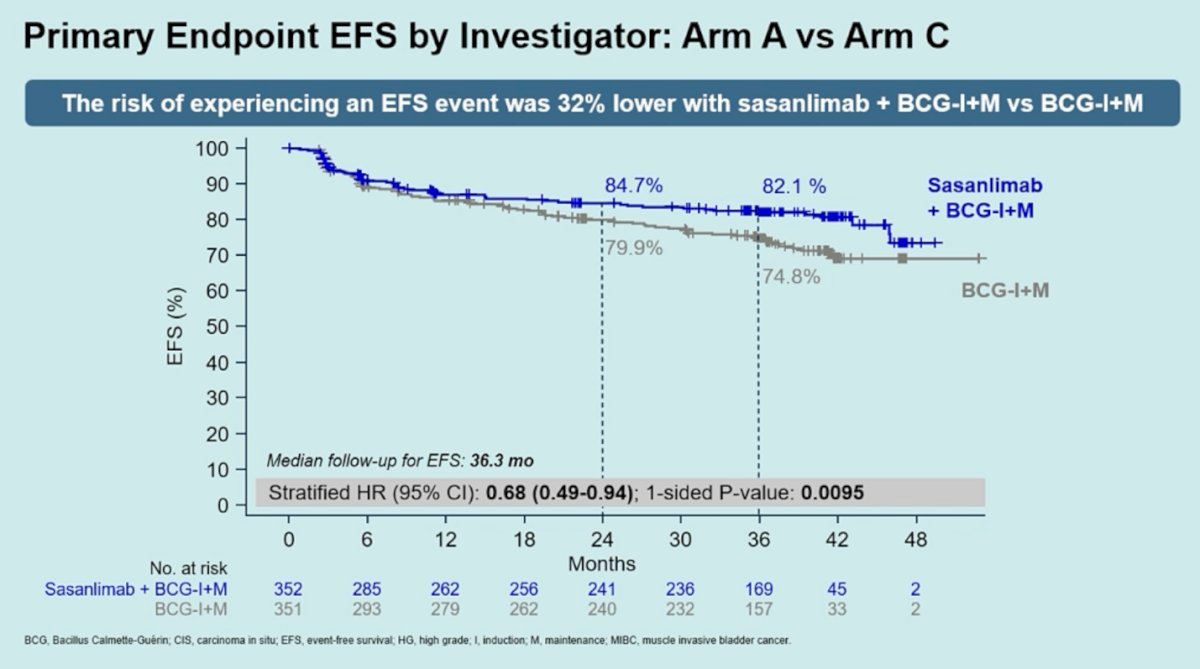
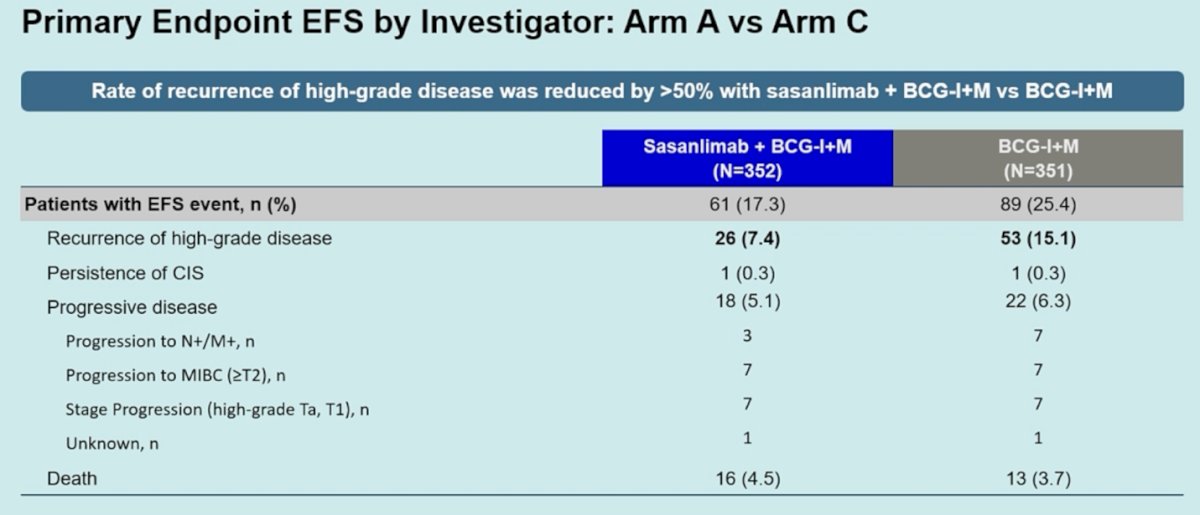
The primary endpoint was event-free survival, defined similarly to POTOMAC and including recurrence of high-grade disease, progression, persistence of CIS, or death. In this comparison of Arm A versus Arm C, the addition of sasanlimab to BCG induction and maintenance resulted in a 32% reduction in the risk of an EFS event compared with BCG alone (HR 0.68; 95% CI 0.49–0.94; one-sided p=0.0095). At a median follow-up of 36.3 months, EFS rates favored the combination, with separation of the curves observed early and maintained over time.
When examining the components of the primary endpoint, Dr. Shore noted that the benefit in EFS was largely driven by a reduction in high-grade recurrences. Recurrence of high-grade disease occurred in 7.4% of patients in the sasanlimab plus BCG arm compared with 15.1% in the BCG-alone arm, representing roughly a doubling of events in the control group. Rates of persistent CIS were low and similar between arms, and progression events were uncommon overall.
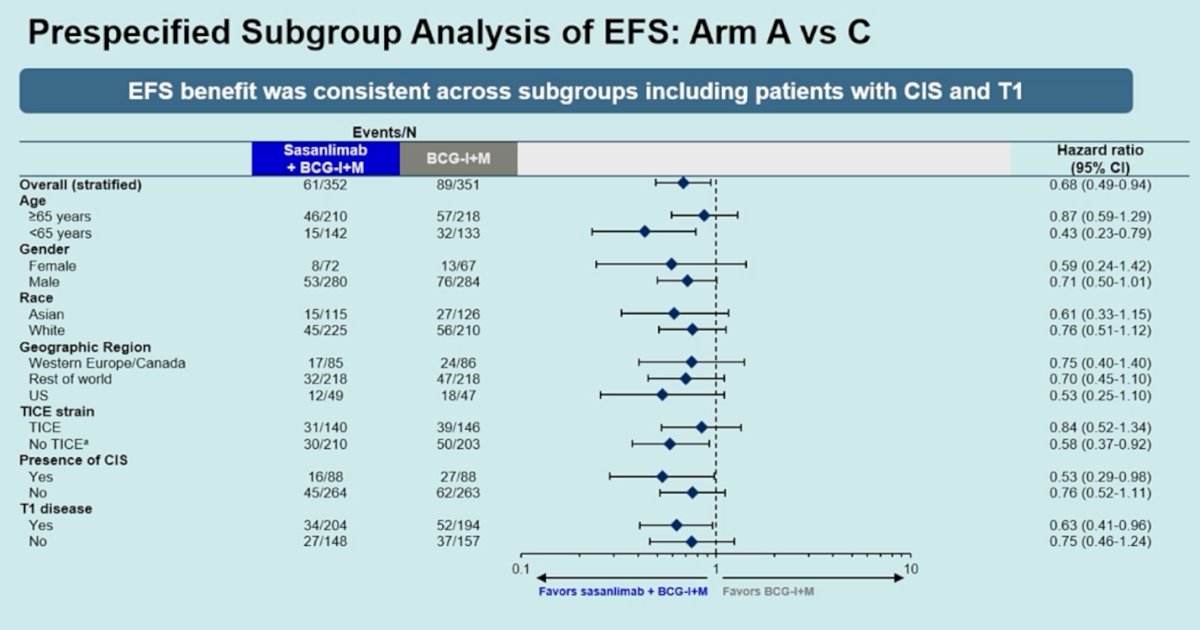
In the prespecified subgroup analysis, the EFS benefit with sasanlimab plus BCG was generally consistent across most subgroups. Dr. Shore highlighted that the effect appeared particularly relevant in patients with CIS, suggesting that this subgroup may derive greater benefit from the addition of checkpoint inhibition. A benefit was also observed among patients with T1 disease. Importantly, outcomes were similar regardless of the BCG strain used, with no meaningful differences observed between TICE and non-TICE strains.
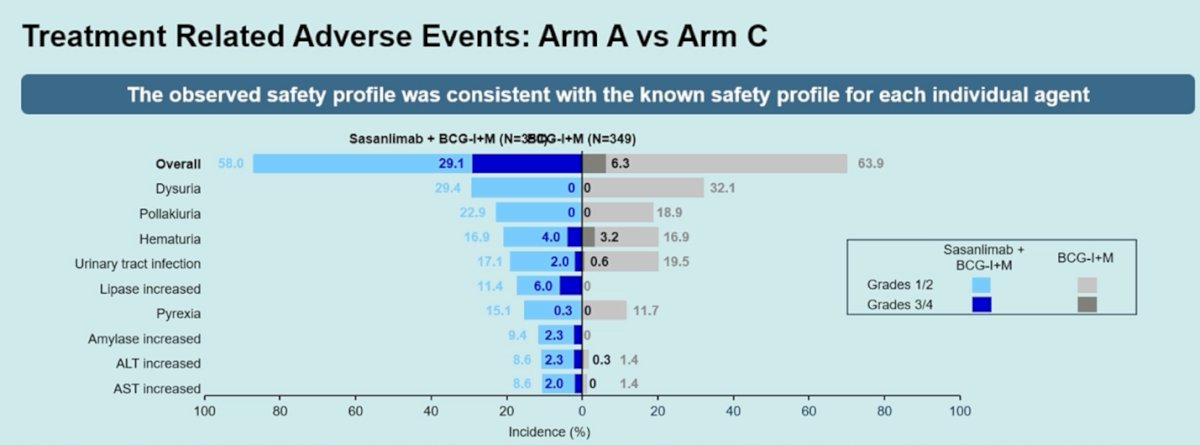
Regarding safety, the observed profile was consistent with the known safety of each individual agent. Dr. Shore noted that if one were to qualitatively compare these findings with those seen in POTOMAC, acknowledging the limitations of cross-trial comparisons, there appeared to be a higher incidence of immune-related adverse events and grade 3/4 events in the combination arm. These immune-related toxicities were largely consistent with what is typically seen with checkpoint inhibitors, including thyroiditis, low-grade rash, transaminitis, and elevations in lipase. Serious treatment-related adverse events occurred more frequently in the sasanlimab plus BCG arm, although no treatment-related deaths were reported.
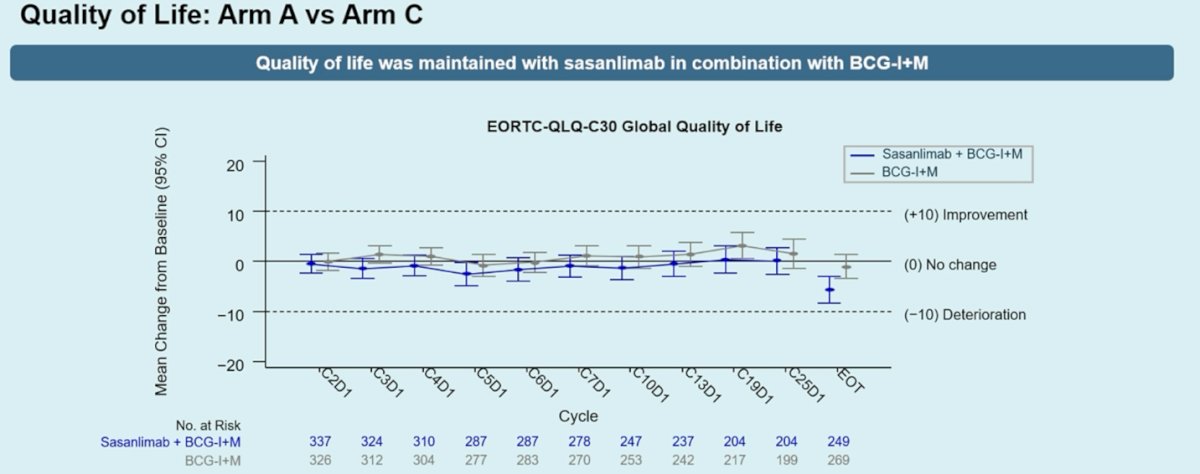
Dr. Shore also reviewed quality-of-life outcomes and noted that quality of life was maintained with the addition of sasanlimab to BCG induction and maintenance. Using the EORTC QLQ-C30 global quality-of-life scale, mean changes from baseline remained close to zero throughout treatment in both arms, indicating no meaningful deterioration associated with the combination therapy, as shown in the graphic below.
Dr. Shore concluded with the following key takeaways:
- CREST demonstrated a statistically significant improvement in EFS with sasanlimab in combination with BCG induction and maintenance compared with BCG induction and maintenance alone in patients with HR-NMIBC (HR 0.68; 95% CI 0.49–0.94).
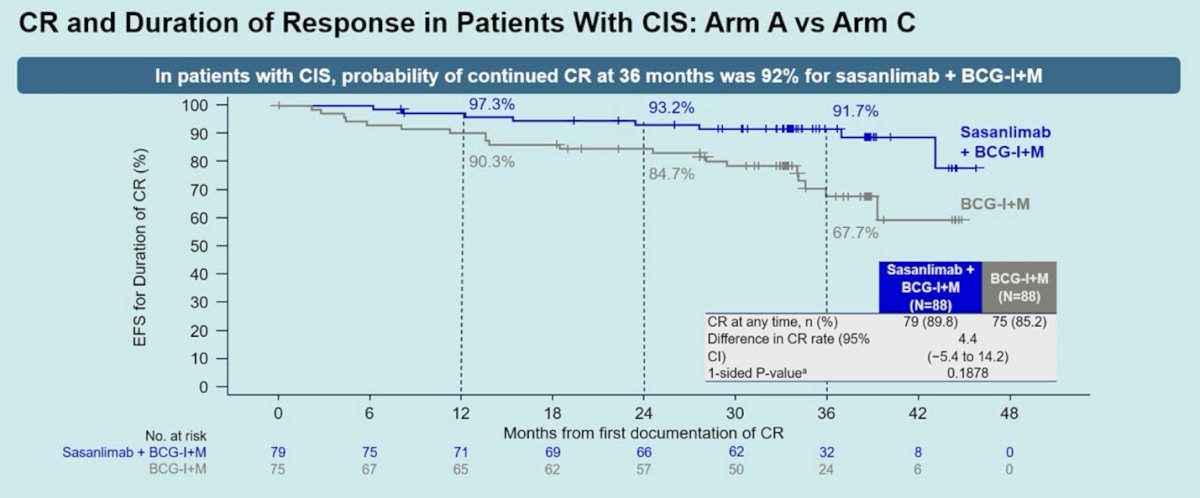
- Among patients with CIS, the probability of maintaining a complete response was higher with the addition of sasanlimab, with a 36-month continued CR rate of 92% compared with 68% with BCG alone.
- The safety profile of sasanlimab combined with BCG was consistent with the known safety profiles of the individual agents.
- Subcutaneous sasanlimab in combination with BCG induction and maintenance has the potential to redefine this treatment paradigm in patients with HR-NMIBC, particularly those with CIS or T1 disease.
- Multidisciplinary collaboration remains essential for monitoring and managing immune-related adverse events.
Presented by: Neal D. Shore, MD, FACS, Director, START Carolinas/Carolina Urologic Research Center, Head of GU Oncology and Radiopharm START Research, AUC Urology Specialists, Myrtle Beach, SC
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
Reference: