(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a metastatic urothelial carcinoma session and a presentation by Dr. Amanda Nizam discussing results from UNITE assessing factors associated with inferior outcomes in patients with advanced urothelial carcinoma treated with first-line enfortumab vedotin + pembrolizumab.
Enfortumab vedotin + pembrolizumab is the preferred first-line regimen for patients with advanced urothelial carcinoma. However, in EV-302, ~10% of patients experienced primary progression on first-line enfortumab vedotin + pembrolizumab.1 As such, Dr. Nizam and colleagues hypothesized that established poor prognostic factors in advanced urothelial carcinoma and variant histology would be associated with inferior outcomes, including early progressive disease.
UNITE is a multi-site retrospective study across 17 US sites of patients with advanced urothelial carcinoma treated with targeted agents. Patients receiving ≥1 dose of first-line enfortumab vedotin + pembrolizumab were included. Observed response rate was assessed in patients with post-baseline imaging. Progression-free survival and overall survival were calculated from enfortumab vedotin + pembrolizumab start to progressive disease or death. Early progressive disease was defined as radiographic or clinical progressive disease ≤12 weeks. Baseline clinicopathologic and somatic alterations by NGS were assessed, and in an exploratory analysis, compared between patients with and without early progressive disease:
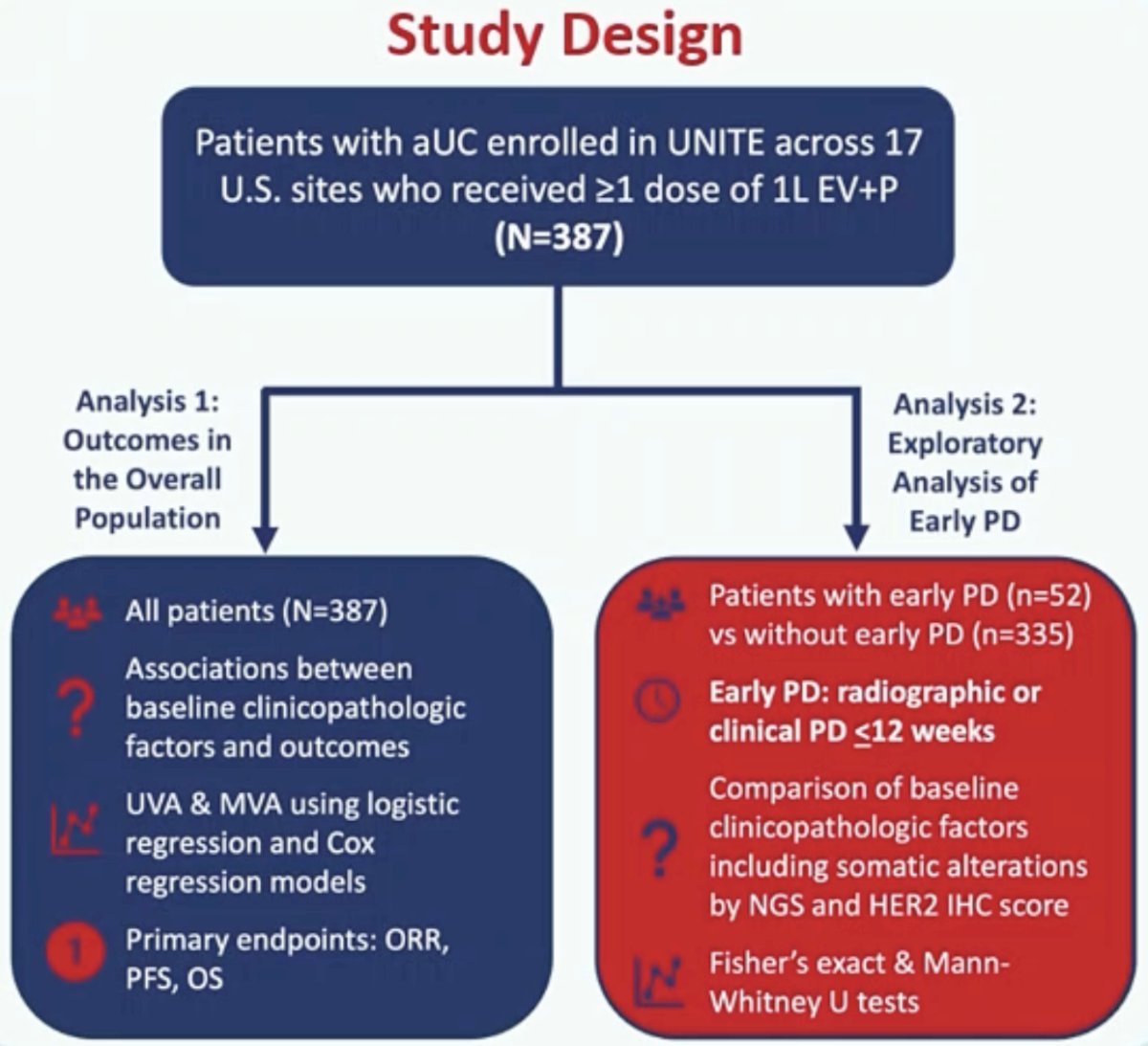
In the overall population, associations between pre-specified factors (derived from a directed acyclic graph) and outcomes were evaluated using univariable and multivariable logistic and Cox regression models.
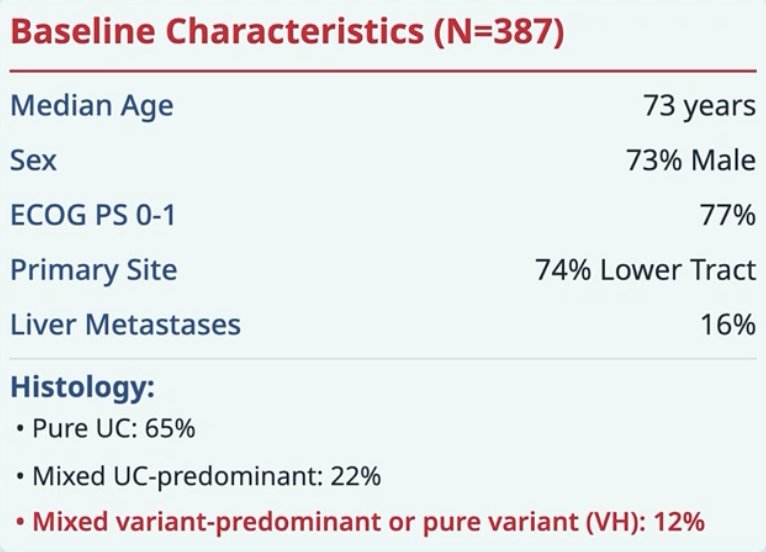
Among 387 patients treated with first-line enfortumab vedotin + pembrolizumab (52 early progressive disease), there were 238 patients who had NGS (34 early progressive disease). At enfortumab vedotin + pembrolizumab start, the median age was 73 years, 73% were male, 81% were White, 77% had an ECOG performance status of 0-1, 74% had a lower tract primary tumor, 65% had pure urothelial carcinoma, 22% mixed urothelial carcinoma, 12% variant histology, and 16% had liver metastases:
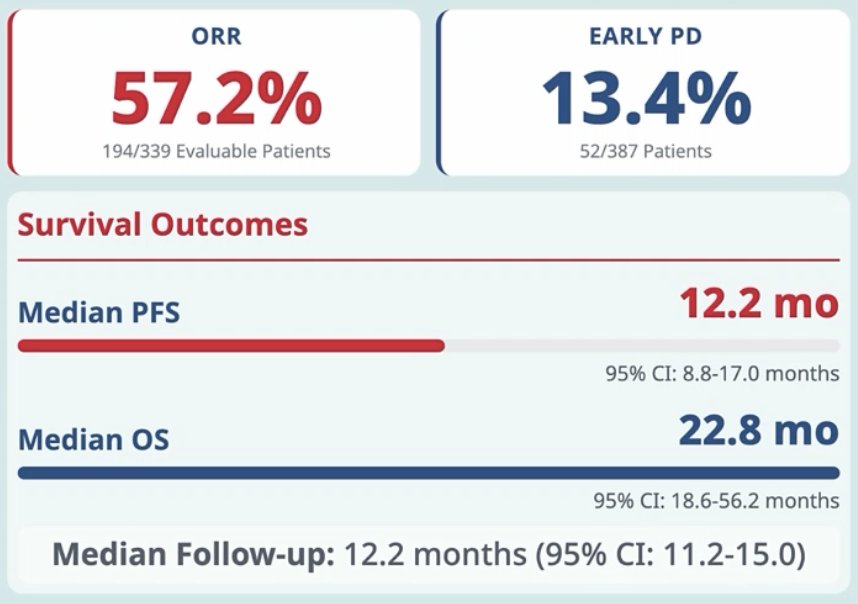
Over a median follow-up of 12.2 months (95% CI 11.2-15.0), the observed response rate was 57.2%, median progression-free survival was 12.2 months (95% CI 8.8-17.0), and median overall survival was 22.8 months (95% CI 18.6-56.2). There were 13.4% of patients who had early progressive disease:
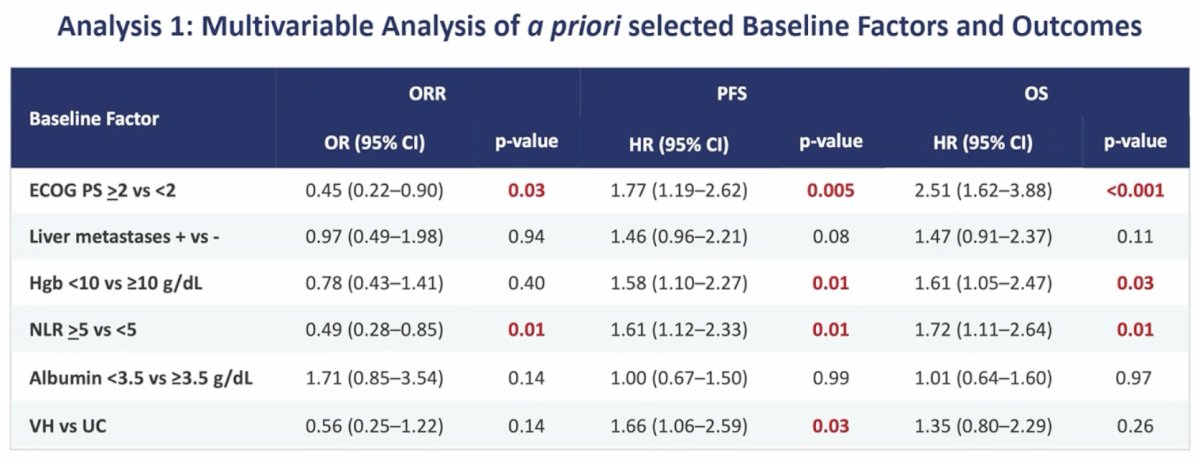
On multivariable analysis of a priori selected baseline factors and outcomes, ECOG performance status ≥2 and NLR ≥5 correlated with lower observed response rate and shorter progression-free survival and overall survival. Variant histology (progression-free survival) and Hgb <10 g/dL (progression-free and overall survival) were associated with worse outcomes:
Early progressive disease correlated with variant histology (p = 0.02), ECOG performance status ≥2 (p = 0.01), lower Hgb (p = 0.001), higher NLR (p = 0.008), and smoking history (p = 0.002). Somatic alterations by NGS and HER2 immunohistochemistry were not associated with outcomes.
Dr. Nizam concluded her presentation discussing results from UNITE assessing factors associated with inferior outcomes in patients with advanced urothelial carcinoma treated with first-line enfortumab vedotin + pembrolizumab, with the following take-home points:
- Real-world outcomes of enfortumab vedotin + pembrolizumab remain consistent with pivotal trial data, supporting the efficacy of enfortumab vedotin + pembrolizumab in practice
- ECOG performance status >2, low hemoglobin, elevated NLR, and mixed variant/predominant or pure variant histology are independently associated with inferior outcomes
- The persistence of these prognostic factors across therapeutic classes suggests that poor outcomes in advanced urothelial carcinoma are largely driven by treatment-agnostic, tumor-intrinsic biology
- Future directions include the following:
- ctDNA integration: incorporation of liquid biopsy markers to capture real-time tumor dynamics and treatment response
- Enhanced histologic analysis: deeper characterization of variant histologic subtypes and their specific biological drivers
- Molecular correlates: expansion beyond somatic alterations to include transcriptomic, epigenomic, and immune profiling
- Refined prognostic models: development of comprehensive risk stratification models that integrate clinical, histologic, and molecular features
Presented by: Amanda Nizam, MD, Cleveland Clinic Taussig Cancer Institute, Cleveland, OH
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
Reference: