(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., between March 13th and 16th 2026, was host to the Urothelial Cancer: Towards Integrated Therapeutic Strategies: Plenary Session. Dr. Matthew Galsky participated in the Case-based panel discussion Beyond platinum: Evolving frontlines in mUC and discussed where ADCs fit in the sequencing.
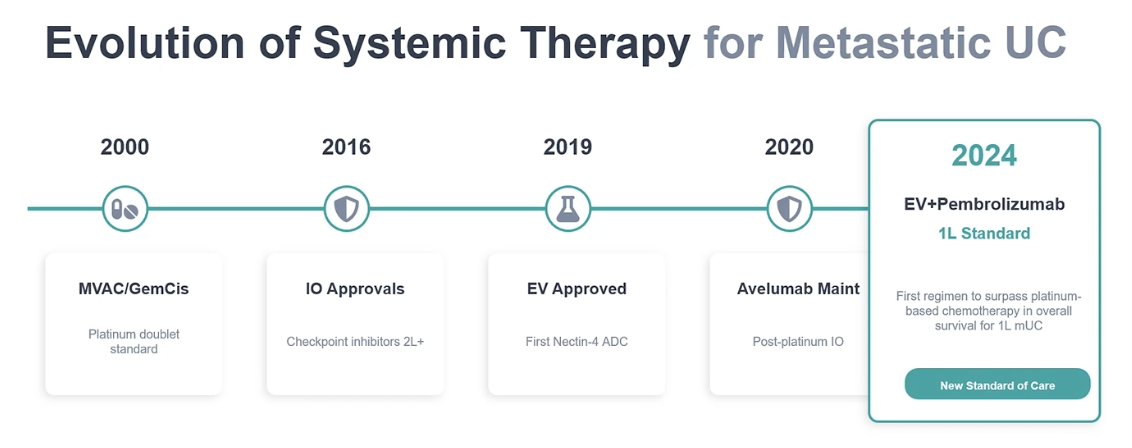
Dr. Galsky began by emphasizing the rapid evolution of systemic therapy for metastatic urothelial carcinoma, noting that for the first time in more than a decade, the field has seen major progress. He reviewed this therapeutic progression from platinum doublets to immune checkpoint inhibitor approvals, to enfortumab vedotin, and then maintenance avelumab, culminating in EV + pembrolizumab becoming the new first-line standard of care for metastatic urothelial carcinoma. He then framed the discussion around the next key question: where do we go from here?
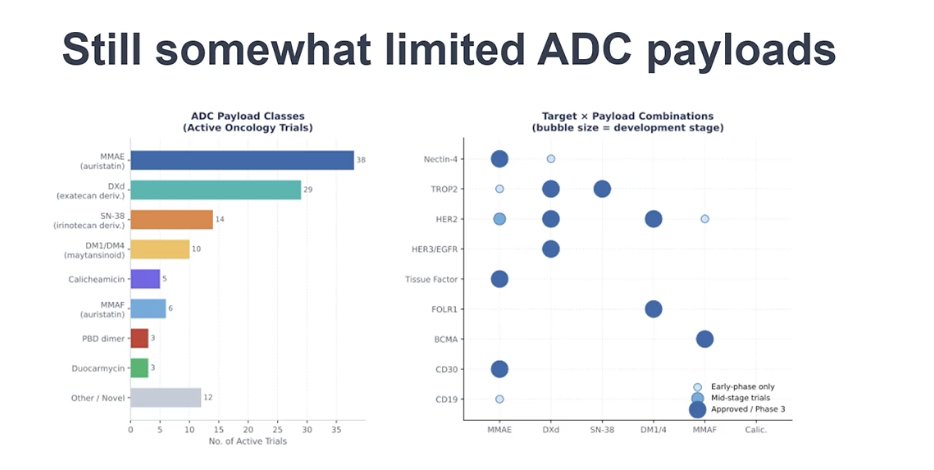
He noted that there is enormous enthusiasm around ADC development, with a rapidly expanding number of active clinical trials exploring a broad range of targets. As shown in the figure, several of these targets are directly relevant to urothelial carcinoma, including HER2, TROP2, nectin-4, and HER3, among others. The challenge now is no longer whether there are enough drugs in development, but rather how to develop them efficiently and how to prioritize which targets and combinations should move forward in bladder cancer.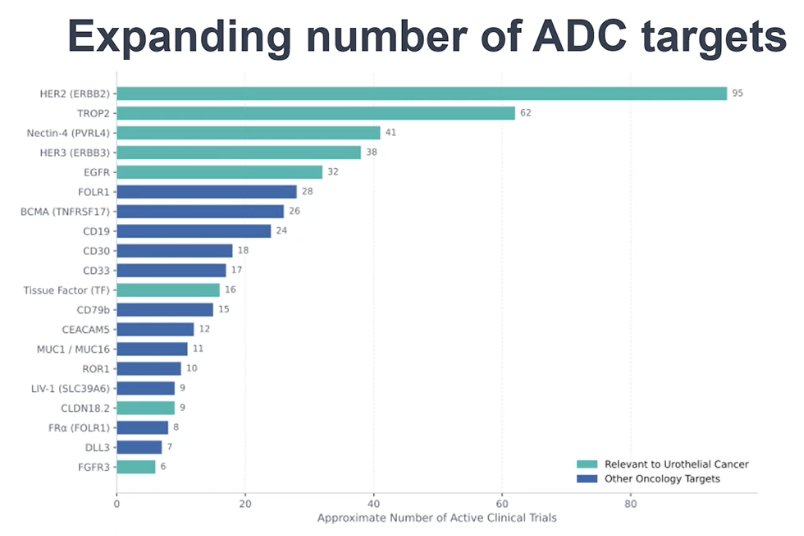
He emphasized that several key considerations will need to be addressed as these agents move forward. How ADCs are used in an EV + pembrolizumab world, whether in combination or sequentially, will ultimately depend on why combinations appear to work, whether through higher single-agent activity, simple additivity, or true synergy. Pragmatic issues such as cost and toxicity will also be critical when developing ADC-based combination regimens. In addition, the clinical disease state in which these drugs are studied will matter, as will prior ADC exposure, including which agent a patient previously received and why it was discontinued. A better understanding of mechanisms of resistance will also be essential to guide rational sequencing and combination strategies.
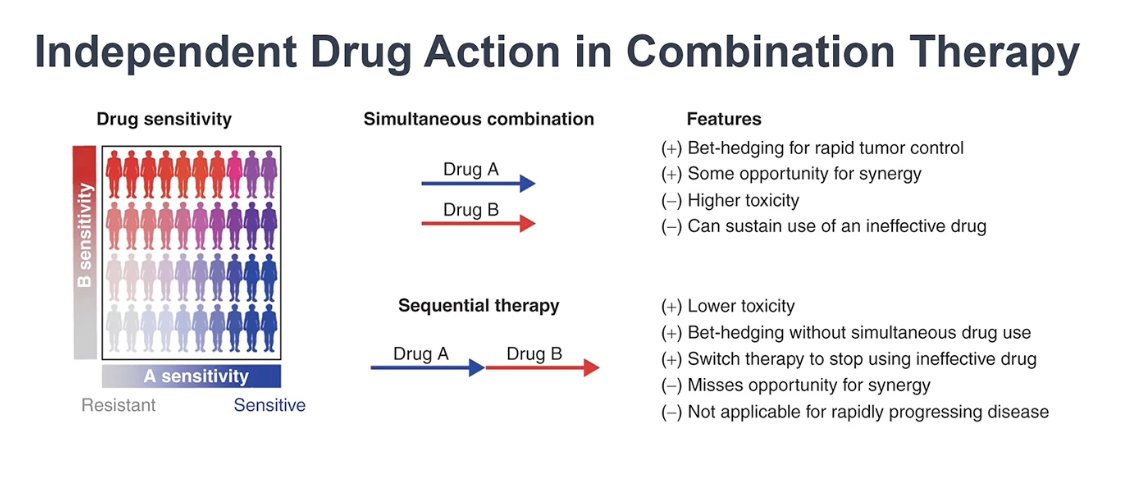
He then discussed why combination therapy is used in oncology. While synergy is often cited as the rationale, true biological synergy is actually difficult to demonstrate and, when modeled rigorously, appears to be relatively uncommon. Analyses of hundreds of randomized trials suggest that most combination regimens work primarily through additivity or through the highest single-agent activity. In other words, giving two active drugs together increases the likelihood that a tumor will be exposed to an effective agent, thereby improving the probability of response rather than producing a true synergistic interaction.1
He explained that the concept of independent drug action helps illustrate why combination therapy can be beneficial. Using two drugs simultaneously allows for “bet-hedging,” increasing the likelihood that at least one active agent will control the tumor, which can be particularly important when rapid tumor control is needed. In contrast, for patients with more indolent or slowly growing disease, a similar strategy can often be achieved through sequential therapy, allowing clinicians to switch treatments if one proves ineffective while potentially minimizing toxicity.
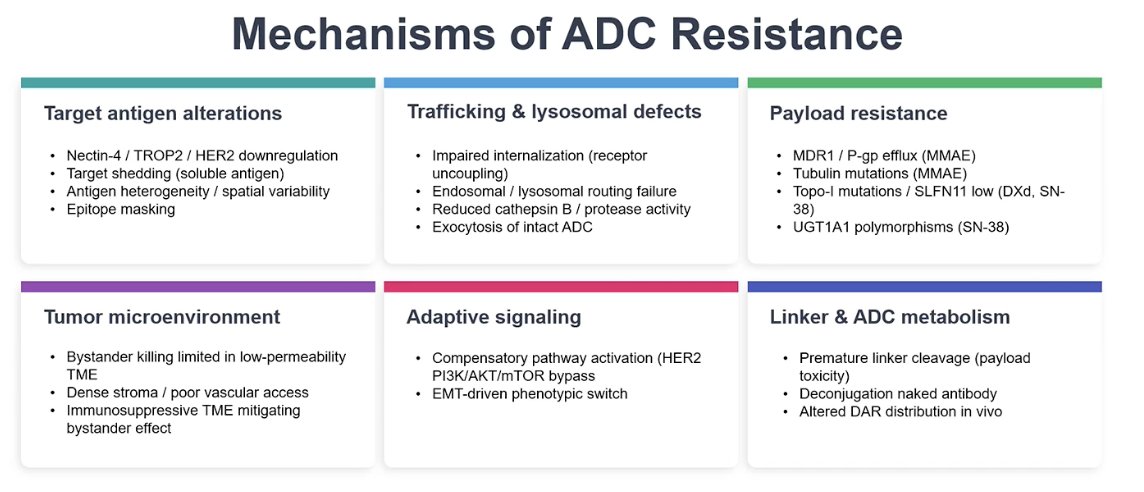
He emphasized that mechanisms of ADC resistance must be considered both in preclinical models and in patients. Multiple resistance pathways have been described, including alterations in the target antigen, defects in intracellular trafficking or lysosomal processing, payload resistance, and influences from the tumor microenvironment or adaptive signaling pathways. A major challenge in developing predictive biomarkers for ADCs is that resistance mechanisms are heterogeneous and may differ across patients, making it difficult to establish a single biomarker that reliably predicts response for all individuals. A summary of mechanisms of ADC resistance is shown below.
Dr. Galsky noted that, despite the growing number of ADC targets, the range of payloads currently used in the clinic remains relatively limited. Most ADCs rely on a small number of payload classes, primarily auristatins such as MMAE or topoisomerase inhibitors. He suggested that it may be more useful to think about these therapies based on payload class rather than simply by target. From a clinical standpoint, an important strategy moving forward may involve switching both targets and payloads when sequencing ADCs, taking advantage of the opportunity to overcome resistance by exposing tumors to different mechanisms of action.
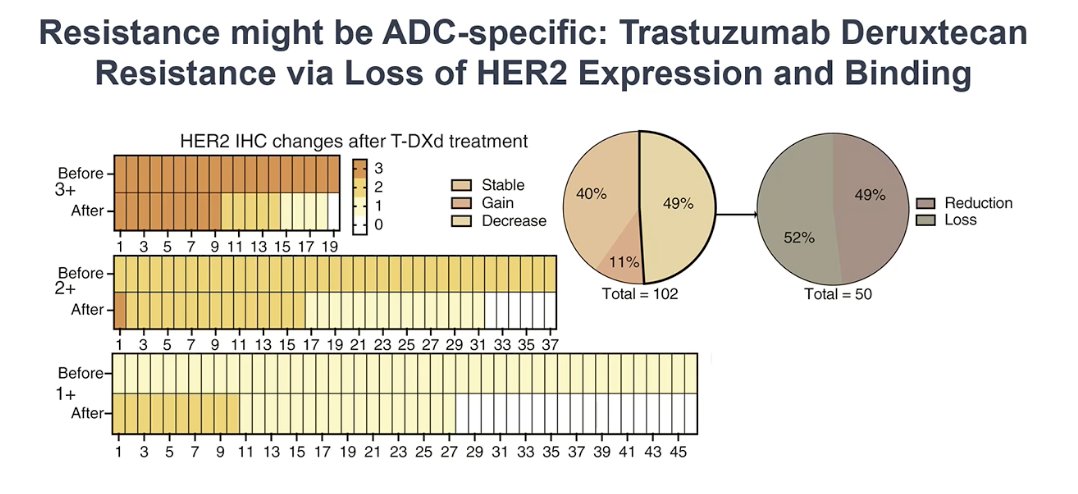
He also discussed mechanisms of resistance, noting that loss of target expression may be ADC-dependent. Using data from breast cancer treated with trastuzumab deruxtecan, an anti-HER2 ADC with a topoisomerase payload, he showed that HER2 expression can decrease over time with treatment. The plots illustrate changes in HER2 IHC before and after therapy, demonstrating that approximately half of the patients lose HER2 expression at the time of progression. These findings suggest that resistance may occur through loss of the target itself, raising the possibility that switching to an ADC with a different payload, rather than simply changing the target, could be a rational strategy in some patients.
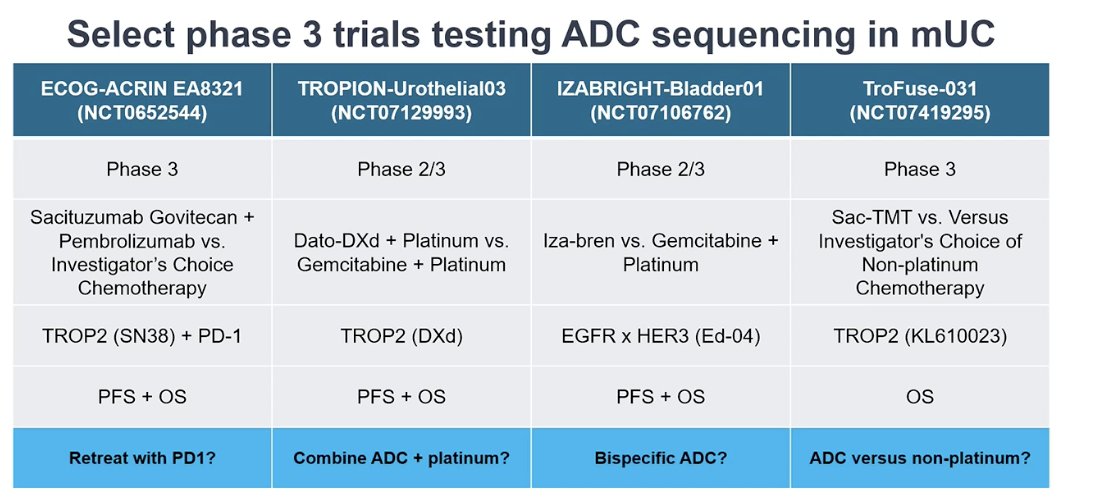
Dr. Galsky also discussed the important issue of ADC sequencing, highlighting several ongoing phase II/III and phase III trials currently in the public domain. These studies are particularly interesting because each addresses a different critical question in the clinical management of metastatic urothelial carcinoma, including PD-1 retreatment with an ADC, combining ADCs with platinum chemotherapy, the development of bispecific ADCs, and whether ADCs can replace non-platinum chemotherapy. These trials are summarized in the table below, with TroFuse-031 being the only study directly testing an ADC against a non-platinum chemotherapy regimen.2
As EV + pembrolizumab moves earlier into the perioperative setting, several new clinical considerations emerge. These include how to treat patients who progress while receiving perioperative EV + pembrolizumab, as well as those who relapse after completing therapy. Important questions also remain regarding which drug should be used after progression and for how long, and whether switching to a different ADC or rechallenging with EV may be appropriate, particularly in patients whose tumors demonstrate increased HER2 expression.
Dr. Galsky concluded his presentation with the following take-home messages:
- ADCs have transformed the treatment landscape of metastatic urothelial carcinoma
- Both combination and sequential strategies are being explored, and optimal approaches will require careful consideration of several factors:
- A realistic understanding of the highest single-agent activity versus additivity versus true synergy
- Pragmatic considerations such as toxicity and cost
- The clinical disease state in which these drugs are used
- Mechanisms of resistance
- Multiple promising ADC targets are emerging in mUC, but maximizing their impact may require the development of additional non–cross-resistant payloads
Presented by: Matthew D. Galsky, MD, FASCO, Professor of Medicine, Icahn School of Medicine at Mount Sinai, Director, Genitourinary Medical Oncology, Associate Director, Translational Research, Tisch Cancer Institute, New York, NY
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Plana D, Palmer AC, Sorger PK. Independent Drug Action in Combination Therapy: Implications for Precision Oncology. Cancer Discov. 2022 Mar 1;12(3):606-624. doi: 10.1158/2159-8290.CD-21-0212. PMID: 34983746; PMCID: PMC8904281.
- Zhu Y, Jiang S, Shi Y, Wang S, Yuan F, Zhou F, Jiang K, Zhang X, Seneviratne L, Yu G, Zhang M, Liu T, Li X, Chen X, Wang X, Zhang S, Liu Y, Ge Y, Chen M, Blumenthal G, Akala O, Li Y, Li X, Ge J, Ye D. Sacituzumab tirumotecan in participants with advanced or metastatic urothelial carcinoma and disease progression after chemotherapy and immune checkpoint inhibitors. Ann Oncol. 2026 Mar;37(3):378-387. doi: 10.1016/j.annonc.2025.11.013. Epub 2025 Nov 21. PMID: 41276258.