(UroToday.com) The European Association of Urology (EAU) 2026 Annual Congress was host to a non-muscle invasive bladder cancer (NMIBC) poster session. Dr. Pietro Scilipoti presented results from a large multicenter study evaluating the real-world oncologic outcomes of bladder-sparing treatment approaches, compared with radical cystectomy (RC), in patients with BCG-unresponsive NMIBC.
Dr. Scilipoti noted that radical cystectomy currently remains the recommended standard of care for patients with BCG-unresponsive NMIBC. However, many patients are either medically unfit for or unwilling to undergo radical surgery. As a result, bladder-sparing approaches have increasingly been adopted in real-world clinical practice. The aim of this study was to describe the oncologic outcomes of patients with BCG-unresponsive NMIBC treated with bladder-preserving therapies, including gemcitabine/docetaxel (Gem/Doce), electromotive drug administration of mitomycin C (EMDA/MMC), additional BCG therapy, or upfront radical cystectomy.
This multicenter retrospective analysis included 361 patients diagnosed with BCG-unresponsive NMIBC who were treated between 2009 and 2024 across 21 centers. Patients received one of four treatment strategies:
- Additional BCG therapy
- Gem/Doce
- EMDA/MMC
- Upfront RC
The primary oncologic endpoints were disease recurrence and progression. Cumulative incidence curves were used to estimate the rates of these outcomes, and multivariable Cox regression models were applied to evaluate the association between treatment type and oncologic outcomes.
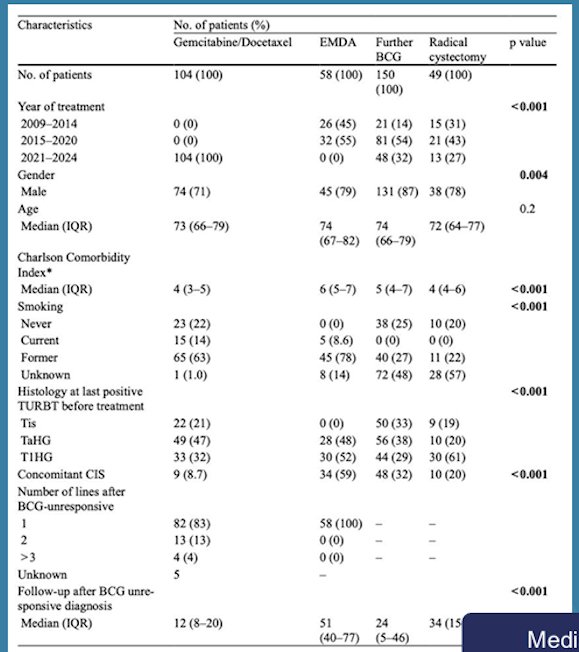
The median follow-up for the study cohort was 73 months. Among the 361 patients with BCG-unresponsive NMIBC, treatment allocation was as follows:
- Additional BCG: 150 patients (42%)
- Gem/Doce: 104 patients (29%)
- EMDA/MMC: 58 patients (16%)
- Upfront RC: 49 patients (14%)
The baseline characteristics varied modestly across treatment groups. The median age ranged from 73–74 years across cohorts, and most patients were male (approximately 77–82%). Differences in comorbidity burden, smoking status, and tumor characteristics were observed across treatment cohorts, reflecting treatment selection patterns in real-world clinical practice.
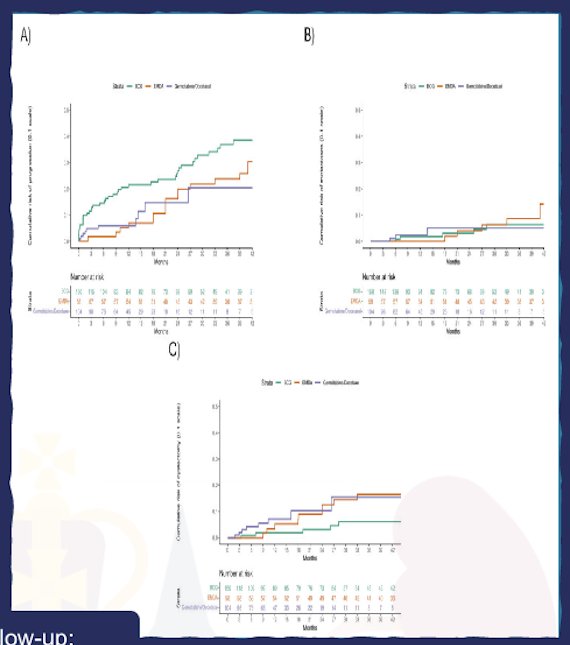
Time-to-event analyses demonstrated differences in the rates of any-grade recurrence, high-grade recurrence, and progression across treatment strategies. In cumulative incidence analyses (Figure panels A–C), bladder-sparing approaches demonstrated distinct patterns of recurrence and progression over time. Multivariable Cox regression analyses showed that Gem/Doce and EMDA/MMC were associated with lower risks of recurrence compared with additional BCG therapy.
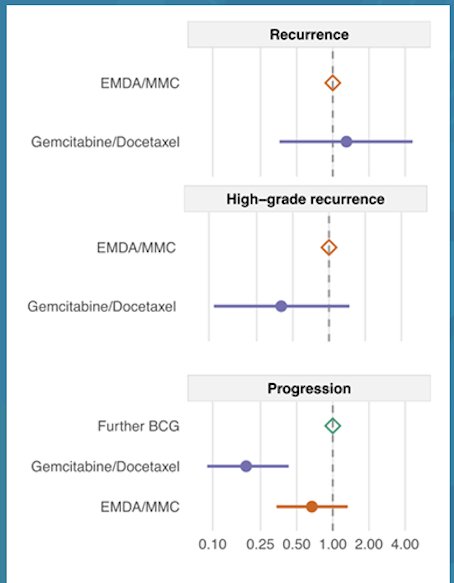
In the forest plot analyses, Gem/Doce demonstrated the lowest relative risk of recurrence, whereas EMDA/MMC showed intermediate outcomes and repeat BCG was associated with higher recurrence risk. For high-grade recurrence, both Gem/Doce and EMDA/MMC demonstrated more favorable point estimates relative to repeat BCG. Similarly, for disease progression, bladder-sparing strategies demonstrated variable risk profiles, with EMDA/MMC showing a numerically higher progression risk compared with Gem/Doce in the multivariable analysis.
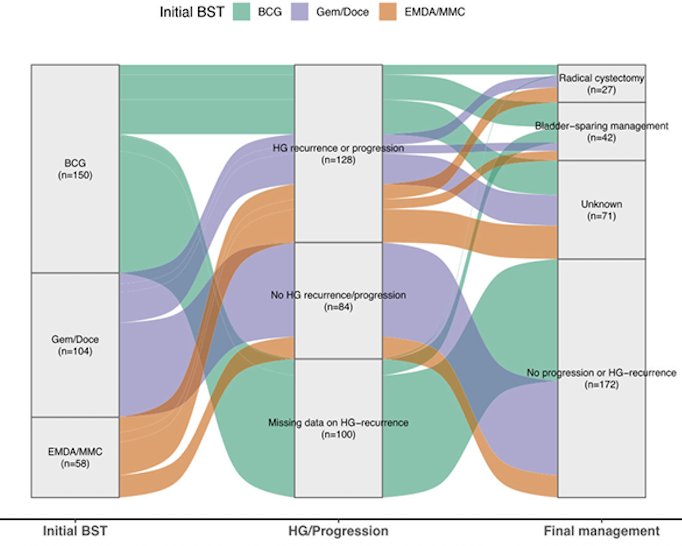
The treatment course Sankey diagram further illustrated the clinical trajectories of patients after initial bladder-sparing therapy. Among the 361 patients, 140 patients (39%) experienced recurrence or progression, whereas 220 patients (61%) did not experience recurrence or progression during follow-up. Among those who developed recurrence or progression, 78 ultimately underwent radical cystectomy, 12 were managed with additional bladder-sparing treatment, and 71 had unknown subsequent management. Among patients without recurrence or progression, 9 later underwent radical cystectomy, 78 continued bladder-sparing management, and 133 had unknown subsequent management. Among the 102 patients who developed high-grade progression, 78 proceeded to radical cystectomy, 12 received bladder-sparing treatment, and 12 had unknown management, highlighting that definitive surgical management remained the most common pathway following high-grade progression.
Overall, these real-world data suggest that both Gem/Doce and EMDA/MMC represent viable bladder-sparing treatment options for selected patients with BCG-unresponsive NMIBC who decline or are not candidates for radical cystectomy. However, for patients who are eligible and willing to undergo surgery, radical cystectomy continues to represent the guideline-endorsed standard of care. The investigators concluded that prospective clinical trials are needed to better define the optimal therapeutic sequencing and management strategies for this challenging patient population.
Presented by: Pietro Scilipoti, MD, Resident Physician, Department of Urology, IRCCS Ospedale San Raffaele, Milan, Italy
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.