(UroToday.com) The European Association of Urology (EAU) 2026 Annual Congress was host to a non-muscle invasive bladder cancer (NMIBC) poster session. Dr. Kevin Keane presented G-DISCO, a first-in-human study of synchronous intravesical gemcitabine + docetaxel administration.
Sequential intravesical gemcitabine + docetaxel is a commonly used salvage treatment for patients with Bacillus Calmette–Guérin (BCG)-unresponsive NMIBC who are either unfit for or decline radical cystectomy. The conventional gemcitabine-first sequence has largely been based on theoretical cell-cycle considerations rather than bladder-specific pharmacologic data. Experimental work using ex vivo porcine bladder models has demonstrated that gemcitabine may enhance the uptake of docetaxel when administered concurrently, supporting the concept of synchronous drug delivery. No pharmacologic incompatibilities between gemcitabine and docetaxel have been identified using Reaxys®, and pre-clinical work conducted at the investigators’ institution confirmed that the two agents remain stable and compatible when combined in a single solution under physiologic and storage conditions. Delivering the drugs synchronously rather than sequentially may reduce treatment time, decrease resource utilization, and limit staff exposure during administration. The G-DISCO study, therefore, represents the first clinical evaluation of synchronous intravesical gemcitabine + docetaxel.
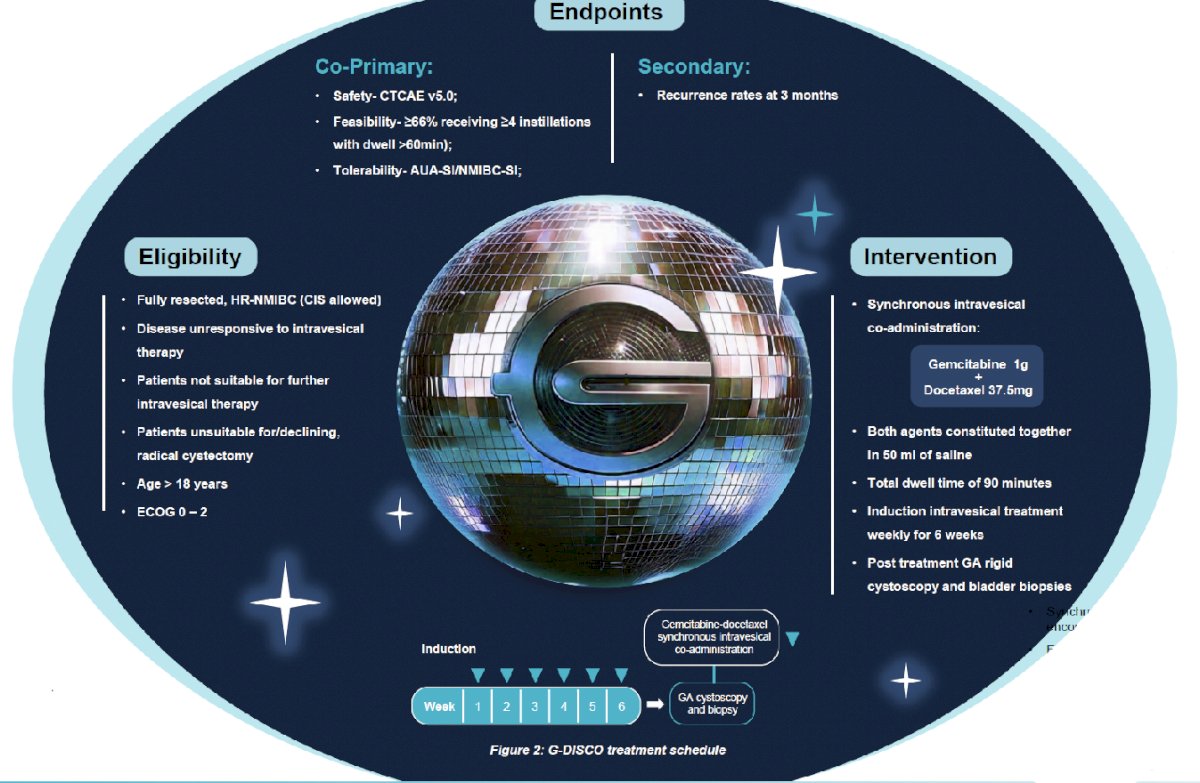
G-DISCO (ANZUP 2403 / ACTRN12624001188527p) is an investigator-initiated, single-arm, open-label phase I study designed to evaluate the feasibility, safety, and tolerability of synchronous intravesical gemcitabine + docetaxel. The study received ethics approval from the SMHS Human Research Ethics Committee (RGS7135). Eligible participants included patients with completely resected, high-risk NMIBC that was BCG-unresponsive, as well as patients who were BCG-ineligible, medically unfit for cystectomy, or who declined surgery. Treatment consisted of gemcitabine 1 g combined with docetaxel 37.5 mg in 50 mL of saline, administered intravesically once weekly for six weeks. The target dwell time was at least 60 minutes, with an optimal dwell time of 90 minutes.
The co-primary study endpoints were feasibility, safety, and tolerability. Feasibility was defined as ≥66% of participants receiving four or more instillations with a dwell time exceeding 60 minutes. Adverse events were graded according to CTCAE version 5.0. Tolerability was assessed using validated symptom instruments, including the American Urological Association Symptom Index (AUA-SI) and the NMIBC Symptom Index (NMIBC-SI). The key secondary endpoint was the presence of recurrence at 3 months, evaluated using cystoscopy and biopsy performed under general anesthesia.
Between January and October 2025, a total of 15 participants were enrolled. The predefined feasibility threshold was met, with 14 of 15 patients (93%) successfully receiving at least four instillations with dwell times exceeding 60 minutes. Thirteen patients (87%) completed the full six planned treatments, while two patients discontinued therapy after four instillations due to storage-related lower urinary tract symptoms.
Synchronous administration was generally well tolerated. There were no statistically significant changes in patient-reported urinary symptoms across the treatment course, with AUA-SI scores remaining stable between screening, Week 3, and Week 6 (p=0.935). Similarly, NMIBC-SI scores did not demonstrate significant change across the treatment period (p=0.38).
Adverse events were observed across all severity grades. Grade 1 events occurred in 7 of 15 patients (47%), grade 2 events in 8 patients (53%), grade 3 events in 4 patients (27%), and grade 4 events in 2 patients (13%). Eight serious adverse events were reported among five participants; however, none were considered related to the gemcitabine + docetaxel combination itself. Two treatment-related infections occurred that required hospital admission.
Among the 13 patients who underwent 3-month cystoscopy and biopsy, 8 patients (62%) achieved a complete response. Recurrence was identified in five patients, including three high-grade recurrences and two low-grade recurrences. Following initial evaluation, nine patients continued on maintenance synchronous gemcitabine + docetaxel therapy. One patient proceeded to radical cystectomy, two patients transitioned to sequential gemcitabine + docetaxel therapy, two opted for cystoscopic surveillance, and one patient was awaiting confirmatory biopsy at the time of reporting.
Based on these results, Dr. Keane concluded that synchronous intravesical gemcitabine + docetaxel administration was feasible, safe, and well-tolerated in this phase I study, with a 3-month high-grade recurrence-free survival rate of 77%. These first-in-human findings support further evaluation of this approach in the planned multinational phase II G-DISCOTEQ trial. If confirmed, synchronous intravesical gemcitabine + docetaxel may offer a more efficient treatment paradigm with shorter administration times, improved clinical workflow, and reduced occupational exposure during drug administration.
Presented by: Kevin Keane, MB, BCh, BAO, MCh, MRCSi, Research Fellow, University of Western Australia, UWA Medical School, Perth, Australia
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.