(UroToday.com) The European Association of Urology (EAU) 2026 Annual Congress was host to a non-muscle invasive bladder cancer (NMIBC) poster session. Dr. Daniele Robesti presented an analysis examining how differences in trial design influence reported efficacy across single-arm studies evaluating therapies for bacillus Calmette-Guérin–unresponsive (BCG-U) carcinoma in situ (CIS).
Comparing outcomes across single-arm trials in patients with BCG-unresponsive CIS is inherently difficult because of heterogeneity in study protocols. Important differences exist across studies in areas such as biopsy timing, definitions, and timing of complete response (CR) assessment, and policies regarding treatment retreatment or rechallenge. These methodological differences can meaningfully influence reported efficacy outcomes.
The aim of this study was to quantify the extent to which trial design characteristics influence reported efficacy estimates in BCG-U CIS trials.
The investigators reconstructed individual-patient survival data from five phase III trials evaluating therapies in BCG-unresponsive CIS. The trials analyzed included studies evaluating:
- Atezolizumab
- Pembrolizumab
- Nadofaragene firadenovec
- Nogapendekin alfa inbakicept plus BCG
- TAR-200
Simulation analyses were then performed to evaluate how key design differences across trials could influence the estimated 12-month CR rates.
Two main adjustments were tested:
- Patients undergoing reinduction or treatment rechallenge were reclassified as non-responders to evaluate the impact of retreatment policies.
- CR estimates were adjusted to account for potential false-negative findings from cystoscopy and urine cytology when biopsy confirmation was not mandated. The nadofaragene firadenovec trial was used as the reference comparator because it uniquely required protocol-mandated biopsies, allowing estimation of the false-negative rate associated with cystoscopy/cytology alone.
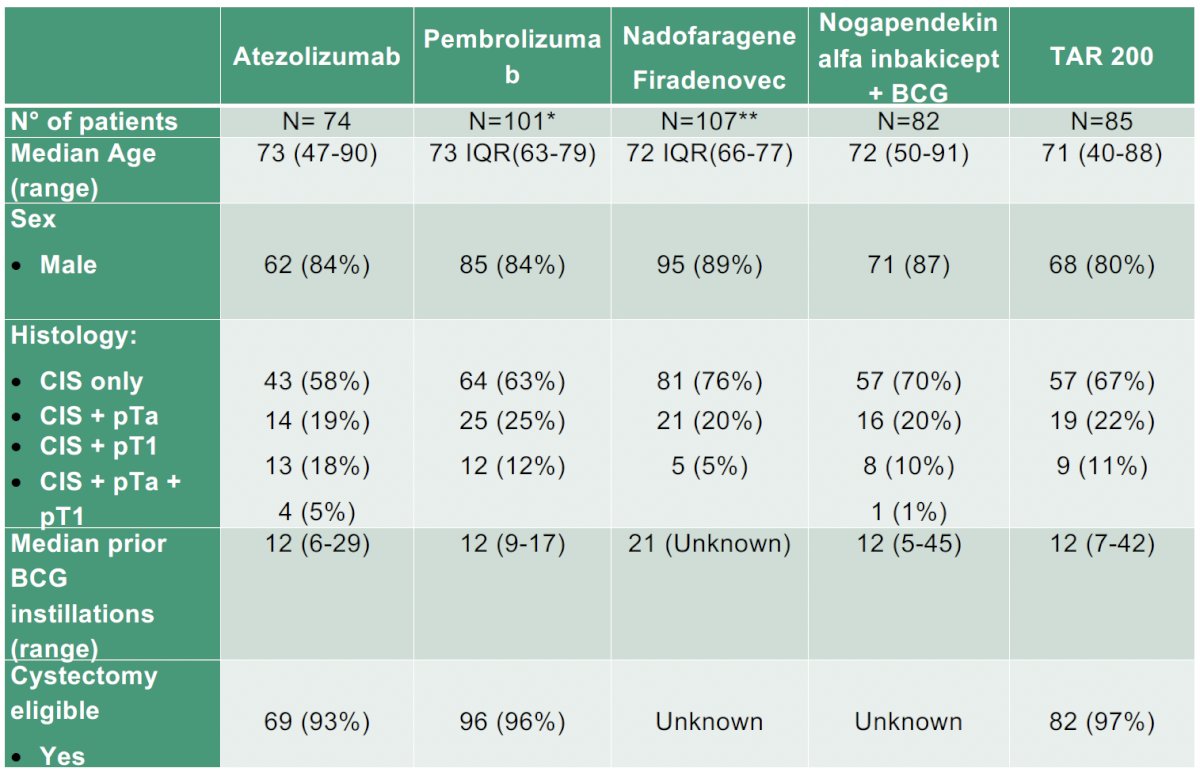
The baseline patient characteristics from each of the five trials are summarized in the table below:
- Sample sizes ranged from 74 patients (atezolizumab) to 107 patients (nadofaragene firadenovec).
- The median patient age was consistently in the early 70s across trials (71–73 years).
- Most patients were male (80–89%).
- The distribution of CIS presentations also varied between studies. For example:
- In the atezolizumab trial, 58% of patients had CIS only, while 19% had CIS with concomitant Ta disease and 18% had CIS with T1 disease.
- In the pembrolizumab study, 63% had CIS only and 25% had CIS with Ta disease.
- In the nadofaragene firadenovec study, 76% had CIS only.
- The number of prior BCG instillations also differed between trials, with medians ranging from approximately 12 to 21 instillations.
- Eligibility for radical cystectomy was high in studies reporting this parameter, with approximately 93–97% of patients considered cystectomy eligible.
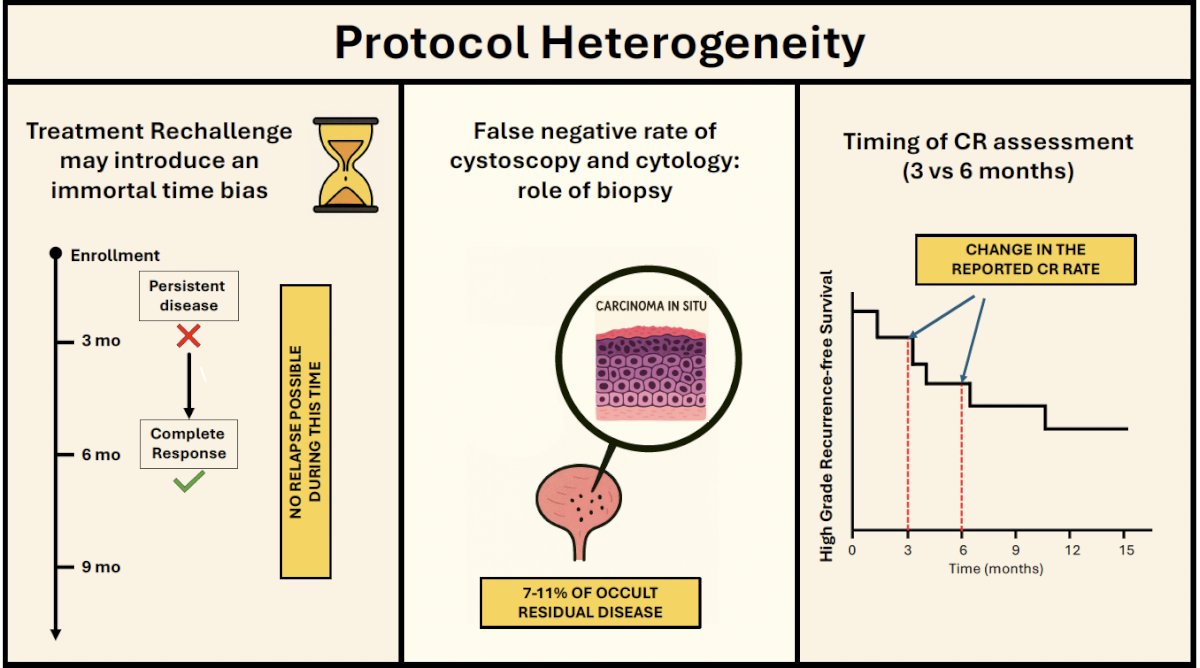
The study investigators highlighted several sources of protocol heterogeneity that may introduce bias when comparing outcomes across trials:
- First, treatment rechallenge or reinduction may introduce an immortal time bias. During the interval between initial response assessment and retreatment, patients cannot be classified as having relapsed, which may artificially inflate response estimates.
- Second, trials differ in the timing of CR assessment, with some studies evaluating responses at 3 months and others at 6 months.
- Third, cystoscopy and urine cytology have a known false-negative rate relative to biopsy.
- 7–11% of patients may harbor occult residual disease when biopsy is not mandated.
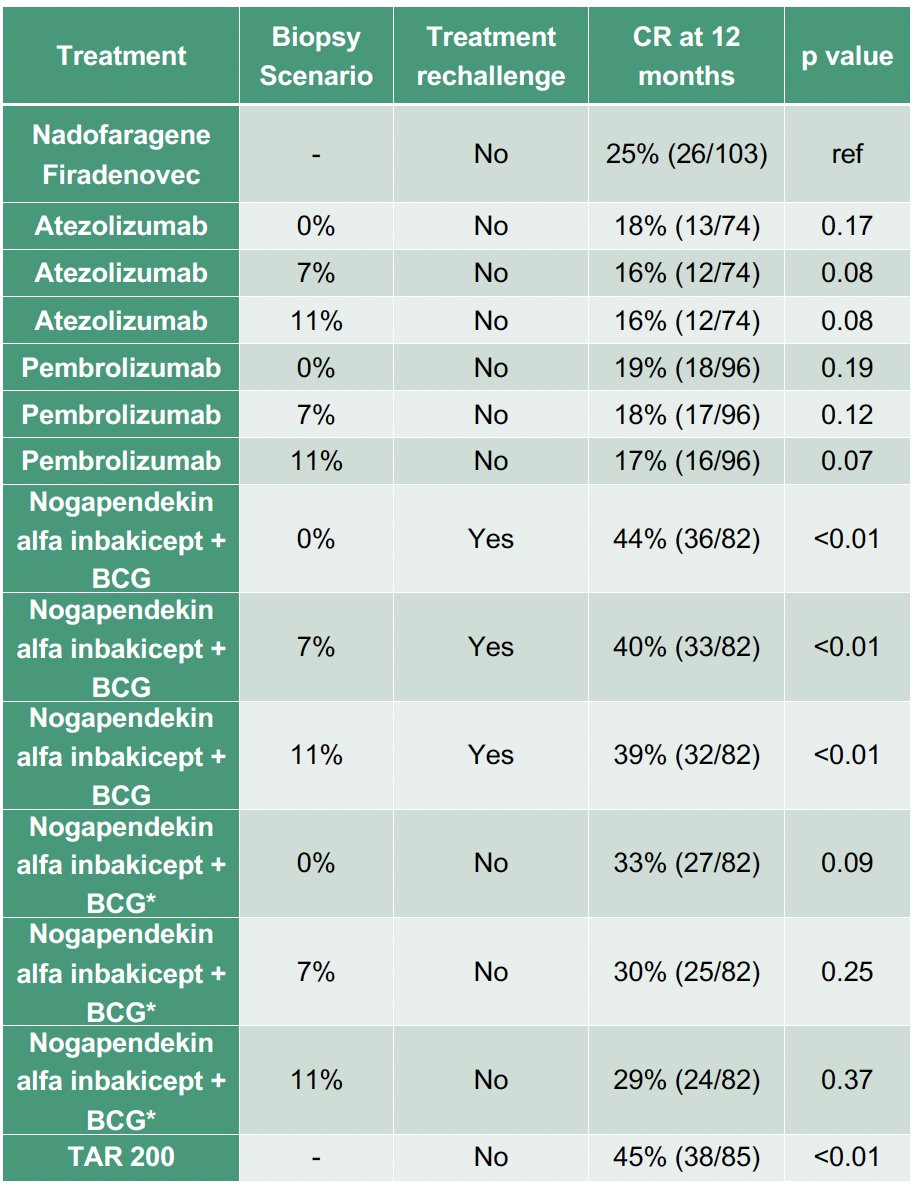
The investigators simulated how trial design features influenced reported 12-month CR rates across therapies. Using the nadofaragene firadenovec trial as the reference scenario (protocol biopsies mandated, no treatment rechallenge), the observed CR rate at 12 months was 25% (26/103).
Reinduction reclassification reduced the 12-month CR rate for nogapendekin alfa inbakicept + BCG from 44% to 33%. After adjusting for an 11% false-negative rate in trials lacking mandatory biopsies, pembrolizumab’s 12-month CR rate declined to 17% (p=0.07), while NAI adjusted for reinduction yielded 29% (p=0.4). TAR-200 remained superior under mandatory biopsy conditions, with a 12-month CR rate of 45% (p<0.01)
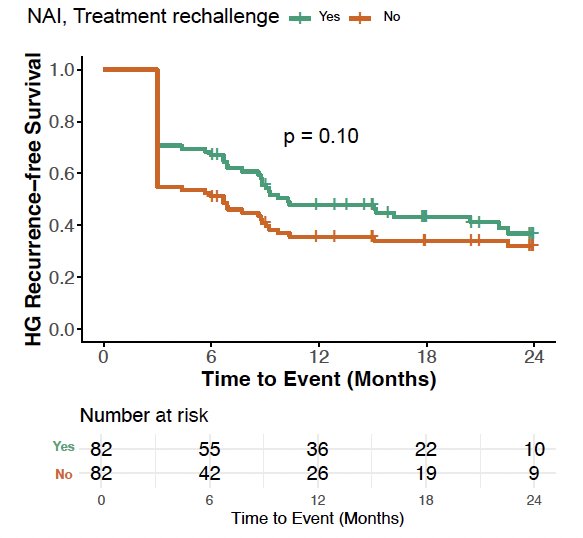
Dr. Robesti and colleagues further evaluated high-grade recurrence-free survival under scenarios with and without treatment rechallenge.
This analysis demonstrates that trial design artifacts can substantially influence reported efficacy outcomes in BCG-unresponsive CIS trials.
Reported complete response rates across studies are therefore not directly comparable across agents because of differences in biopsy requirements, CR assessment timing, and retreatment strategies.
The authors emphasize that future trials in BCG-unresponsive NMIBC should harmonize key protocol elements—particularly biopsy timing and retreatment policies—to allow meaningful comparisons of therapeutic efficacy across studies.
Presented by: Daniele Robesti, MD, Urology Resident Physician, Vita-Salute San Raffaele University, Milan, Italy
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Black PC, Tangen CM, Singh P, et al. Phase 2 trial of atezolizumab in bacillus Calmette-Guérin–unresponsive high-risk non–muscle-invasive bladder cancer: SWOG S1605. Eur Urol. 2023;84(6):536-44.
- Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): an open-label, single-arm, multicentre, phase 2 study. Lancet Oncol. 2021;22(7):919-930.
- Boorjian SA, Alemozaffar M, Konety BR, et al. Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: a phase III clinical trial. Lancet Oncol. 2021;22(1):107-117.
- Chamie K, Chang SS, Kramolowsky EV, et al. IL-15 superagonist nogapendekin alfa inbakicept plus BCG for BCG-unresponsive non-muscle-invasive bladder cancer (QUILT-3.032): results from a multicentre phase II/III study. NEJM Evid. 2023;2(1): EVIDoa2200167.
- Daneshmand S, van der Heijden MS, Jacob JM, et al. TAR-200 for Bacillus Calmette-Guérin–Unresponsive High-Risk Non–Muscle-Invasive Bladder Cancer: Results From the Phase IIb SunRISe-1 Study. J Clin Oncol. 2025;43(33):3578-88.