(UroToday.com) The European Association of Urology (EAU) 2026 Annual Congress was host to a session on risk stratification for non-muscle invasive bladder cancer (NMIBC). Dr. Jethro Kwong presented RECURxNCE-BCa, an artificial intelligence-based tool to predict NMIBC recurrences using the WHO 2004/2022 grading system.
Current tools used to estimate recurrence risk in NMIBC, such as the European Organization for Research and Treatment of Cancer (EORTC) and the Club Urologico Español de Tratamiento Oncológico (CUETO) risk calculators, were developed using historical cohorts that may not adequately represent contemporary practice. Notably, these models do not incorporate the updated World Health Organization (WHO) 2004/2022 grading system. Dr. Kwong and colleagues therefore sought to develop a modern recurrence risk prediction model incorporating contemporary grading systems and artificial intelligence approaches.
RECURxNCE-BCa was trained using 14 clinicopathological features from 3,797 patients treated between 2005 and 2023 across 34 North American and European institutions. A held-out testing cohort included 8,862 patients from the same centers and time period. The primary endpoint was time to first recurrence.
Model performance was assessed in the testing cohort and compared with the EORTC and CUETO risk calculators using concordance indeces (c-index), calibration plots, and decision curve analysis. In addition, RECURxNCE-BCa was evaluated for its ability to further stratify intermediate-risk NMIBC (IR NMIBC) as defined by European Association of Urology (EAU) criteria. For this analysis, thresholds were derived from the top and bottom thirds of RECURxNCE-BCa scores within the training cohort. The performance of this approach was compared with two established clinical risk stratification methods: the International Bladder Cancer Group (IBCG) model, which categorizes patients into 0, 1–2, or ≥3 risk factors, and the IR Low versus IR High classification system, which defines IR High disease as either multiple tumors or tumor size >3 cm.
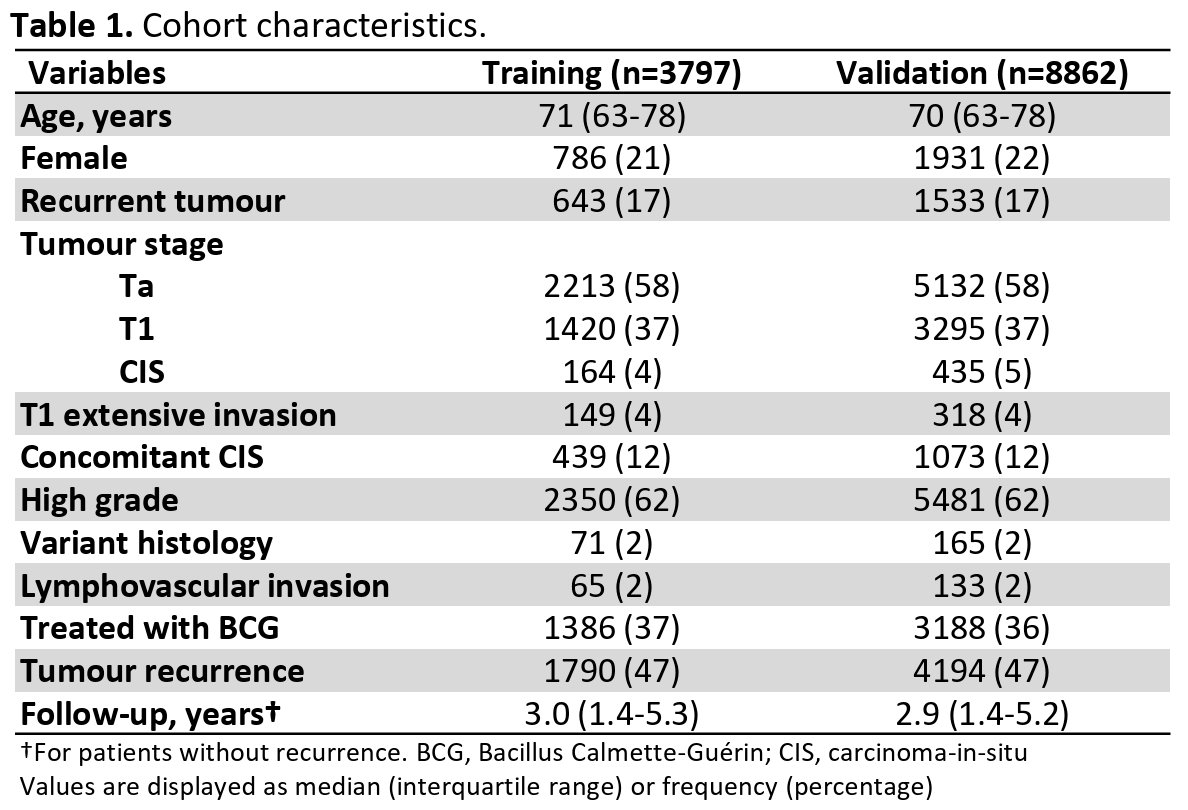
A total of 12,659 NMIBC patients were included across the training and validation cohorts. The training cohort consisted of 3,797 patients, while the validation cohort included 8,862 patients. Median age was similar between cohorts (70-71 years), and approximately 20% of patients were female. Tumor stage distribution was comparable between cohorts, with Ta disease present in 58%, T1 disease in 37%, and carcinoma in situ (CIS) in approximately 4–5% of patients. High-grade disease was observed in 62% of patients in both cohorts. Concomitant CIS was present in approximately 12% of patients, while variant histology and lymphovascular invasion were relatively uncommon (2% and 1–2%, respectively). Approximately one-third of patients received intravesical Bacillus Calmette–Guérin (BCG) therapy. Median follow-up was 3.0 years (IQR 1.4–5.3) in the training cohort and 2.9 years (IQR 1.4–5.2) in the validation cohort
During follow-up, recurrence occurred in 5,984 of the 12,659 patients across the full dataset. In the validation cohort, the artificial intelligence–based RECURxNCE-BCa model achieved a concordance index (c-index) of 0.67 (95% CI 0.66–0.67), demonstrating improved discrimination compared with established clinical risk calculators.
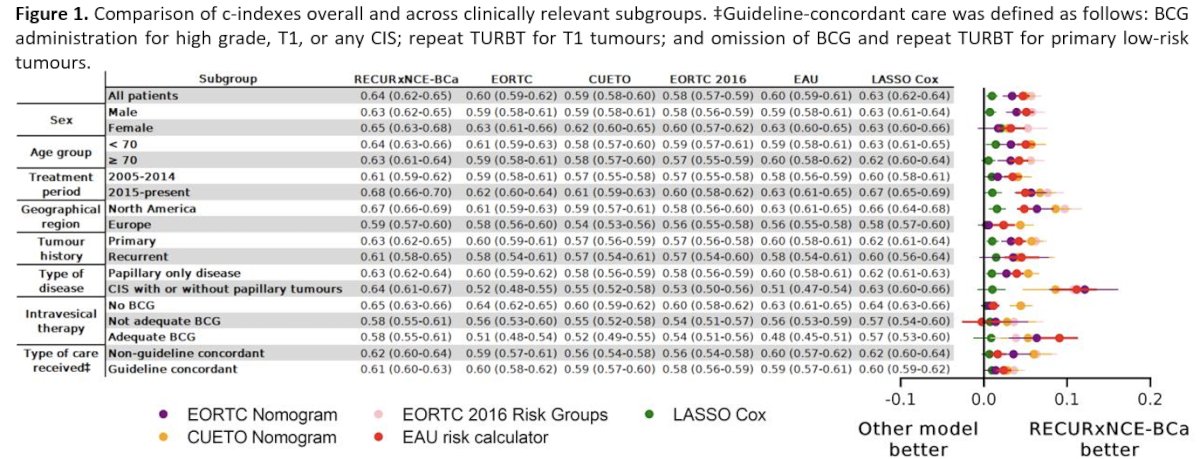
Across clinically relevant subgroups, RECURxNCE-BCa consistently demonstrated higher c-indices compared with existing models, including the EORTC nomogram, the CUETO model, the 2016 EORTC risk groups, and the EAU risk calculator. In the overall cohort, RECURxNCE-BCa achieved a c-index of 0.64 (95% CI 0.62–0.65), compared with 0.60 (95% CI 0.59–0.62) for the EORTC nomogram and 0.59 (95% CI 0.58–0.60) for the CUETO model. Performance remained stable across important clinical subgroups, including sex, age category, treatment era, geographic region, tumor history, intravesical therapy exposure, and guideline-concordant care. Notably, discrimination improved modestly in more contemporary cohorts (2015–present), with a c-index approaching 0.68.
Substratification analyses further evaluated the model’s performance within intermediate-risk NMIBC. When patients were divided into tertiles based on RECURxNCE-BCa scores, the model demonstrated clear separation of recurrence risk. Among patients with low-grade tumors only, estimated 5-year recurrence risks were 51% for the lowest tertile, 60% for the middle tertile, and 70% for the highest tertile. A similar gradient was observed among patients with high-grade tumors, with 5-year recurrence risks of 35%, 47%, and 63% across the low-, middle-, and high-risk tertiles, respectively
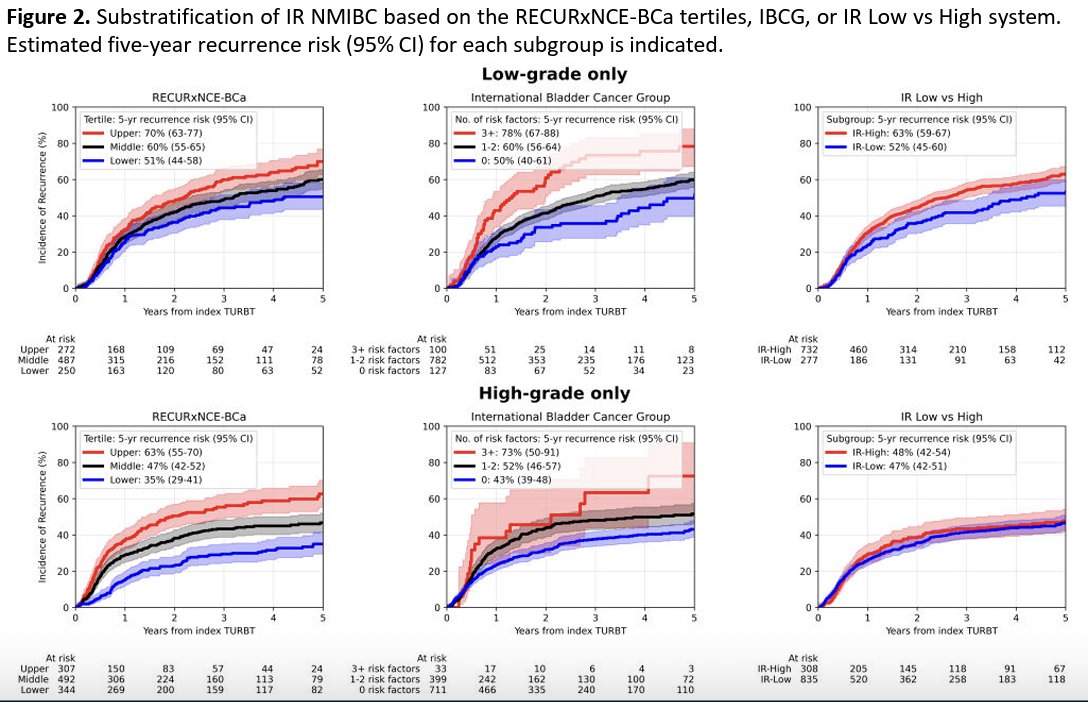
When compared with established clinical risk stratification approaches, RECURxNCE-BCa demonstrated comparable discriminatory ability relative to the IBCG model, while providing a more balanced distribution of patients across risk categories. In contrast, the commonly used IR Low versus IR High system resulted in more limited separation between risk groups.
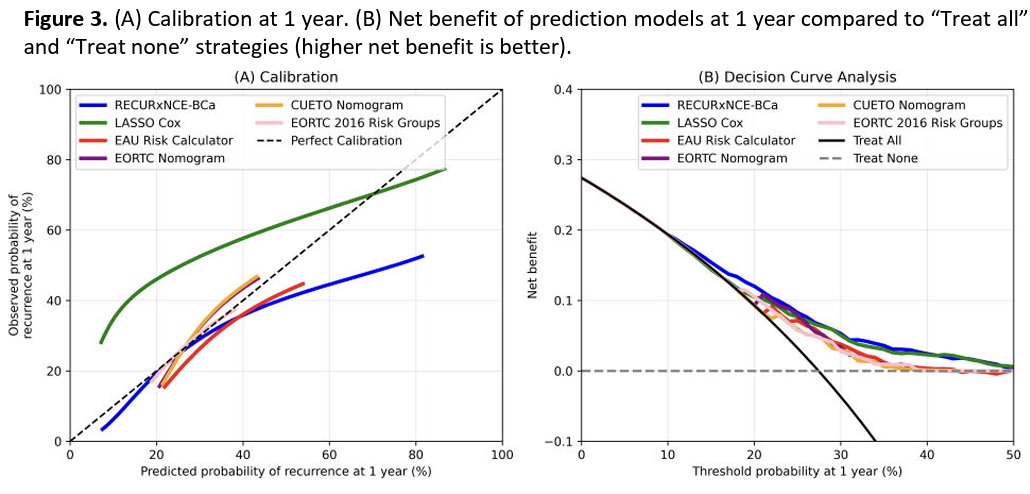
Calibration analyses demonstrated improved agreement between predicted and observed recurrence risk with RECURxNCE-BCa compared with existing risk calculators. At one year, the RECURxNCE-BCa model showed closer alignment with the ideal calibration line relative to the EORTC, CUETO, and EAU models. Decision curve analysis further demonstrated that RECURxNCE-BCa provided the greatest net clinical benefit across a range of clinically relevant recurrence probability thresholds when compared with competing models and the “treat all” or “treat none” strategies.
Dr. Kwong concluded that RECURxNCE-BCa outperformed current tools in predicting recurrence in the largest NMIBC cohort to date. However, its overall performance remains modest, likely limited by institutional variations in surgical and perioperative practices, or other factors not captured by conventional risk factors. For intermediate-risk NMIBC, RECURxNCE-BCa substratification performed similarly to the IBCG system and offered a more balanced distribution of patients across tertiles.
Presented by: Jethro Kwong, MD, MSc, Resident Physician, Division of Urology, University of Toronto, Toronto, ON, Canada
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.