(UroToday.com) The European Association of Urology (EAU) 2026 Annual Congress was host to the “Common Problems and Controversies in Bladder Cancer: Rapid-Fire Debates” session, developed and led by Dr. Ashish Kamat. Dr. Paolo Gontero presented a case study, following which Drs. Jeremy Teoh and Laura Mertens debated whether it was time to ‘ditch’ cystoscopy in favor of urinary biomarkers for the surveillance of patients with non-muscle invasive bladder cancer (NMIBC).
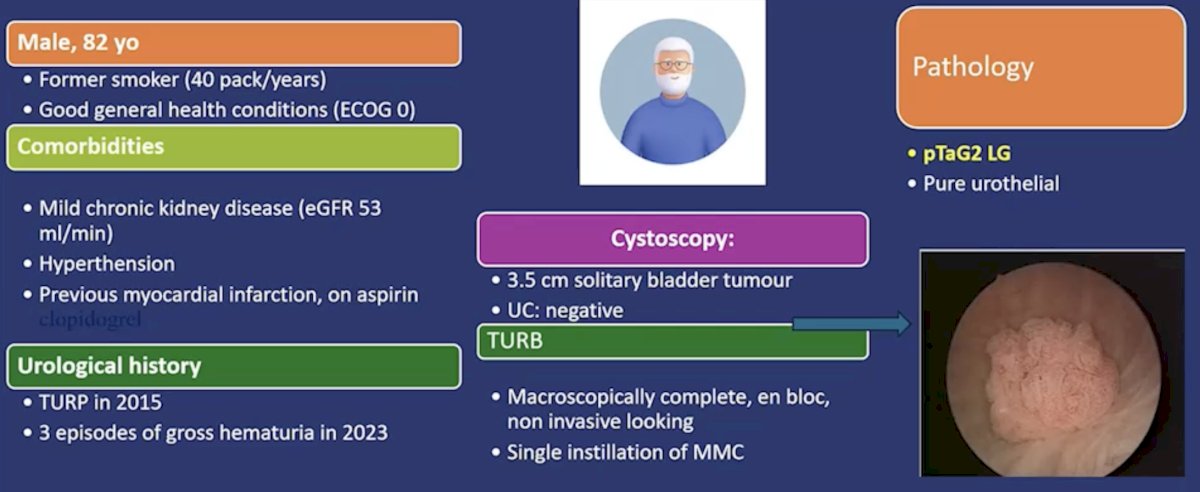
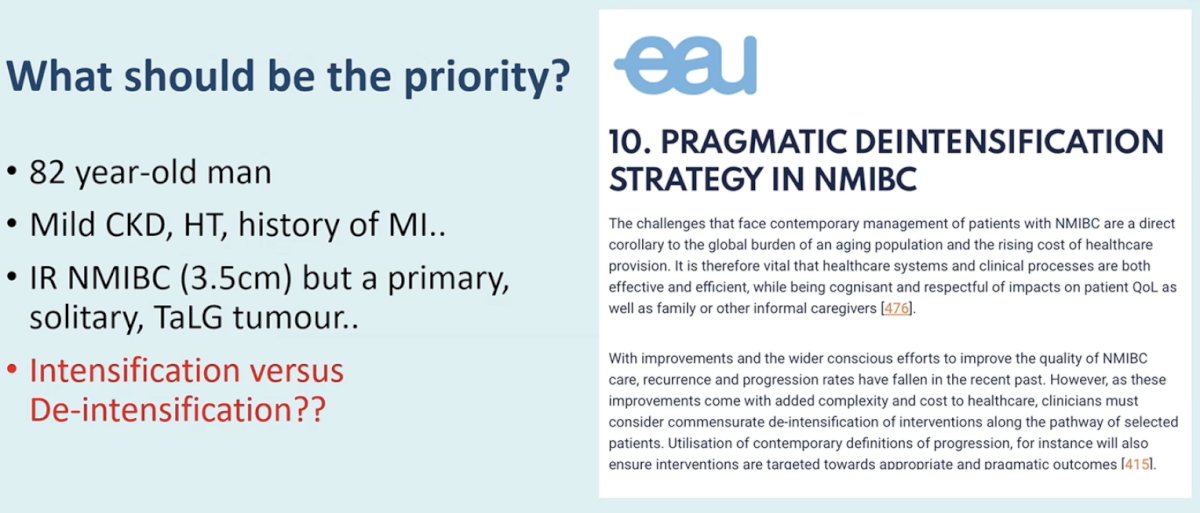
Dr. Gontero presented a case of an 82-year-old former-smoker (40 pack-year) with a significant cardiac history who was found to have a 3.5 cm solitary bladder tumor, in the setting of a negative urine cytology. He underwent an en block transurethral resection of bladder tumor (TURBT) with a single post-operative instillation of mitomycin, with final pathology demonstrating low-grade Ta disease.
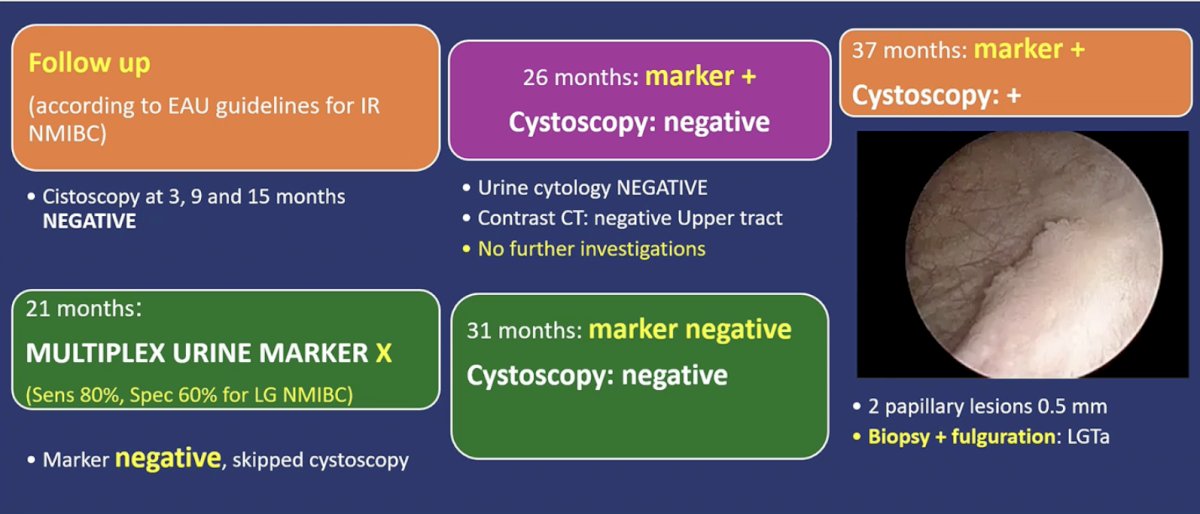
He underwent follow up in accordance with the EAU guidelines for intermediate-risk NMIBC with negative cystoscopies at 3, 9, and 15 months. At 21 months, he had a urinary biomarker test (Multiplex – sensitivity: 80%, specificity 60% for low-grade NMIBC) that was negative. As such, cystoscopy was omitted at 21 months. At 26 months, his marker converted to a positive, yet his urine cytology, CT of his upper tracts, and cystoscopy were all negative. At 31 months, both cystoscopy and the urine test were negative.
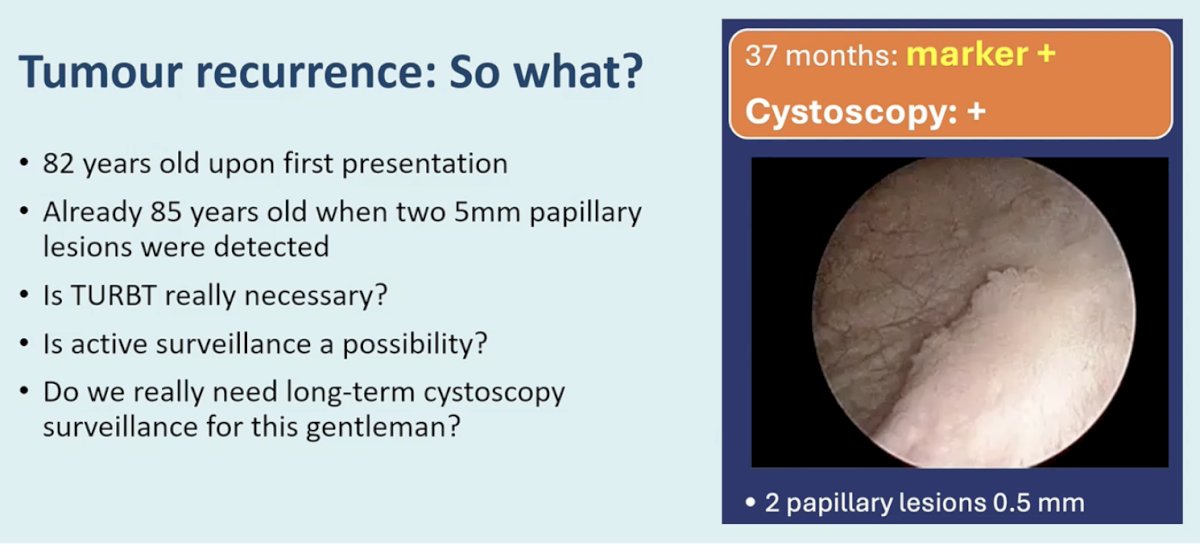
At 37 months, however, the urinary marker again became positive, and cystoscopy demonstrated two small papillary lesions measuring approximately 5 mm. Biopsy and fulguration confirmed low-grade Ta disease.
Dr. Gontero used this scenario to illustrate the clinical dilemma: in elderly patients with low-risk or intermediate-risk disease, intensive cystoscopic surveillance may represent overtreatment, yet replacing cystoscopy with urinary markers introduces the risk of delayed detection or unnecessary investigations.
Following this case presentation, Dr. Jeremy Teoh presented the affirmative position in the debate: that urinary markers are ready to replace cystoscopy in appropriate clinical settings.
Dr. Teoh first emphasized the biological and clinical risk profile of the presented case. The patient had a primary, solitary Ta low-grade urothelial carcinoma measuring 3.5 cm without concomitant CIS, representing classic intermediate-risk NMIBC. He highlighted that current risk stratification systems consistently show very low risks of progression for such patients.
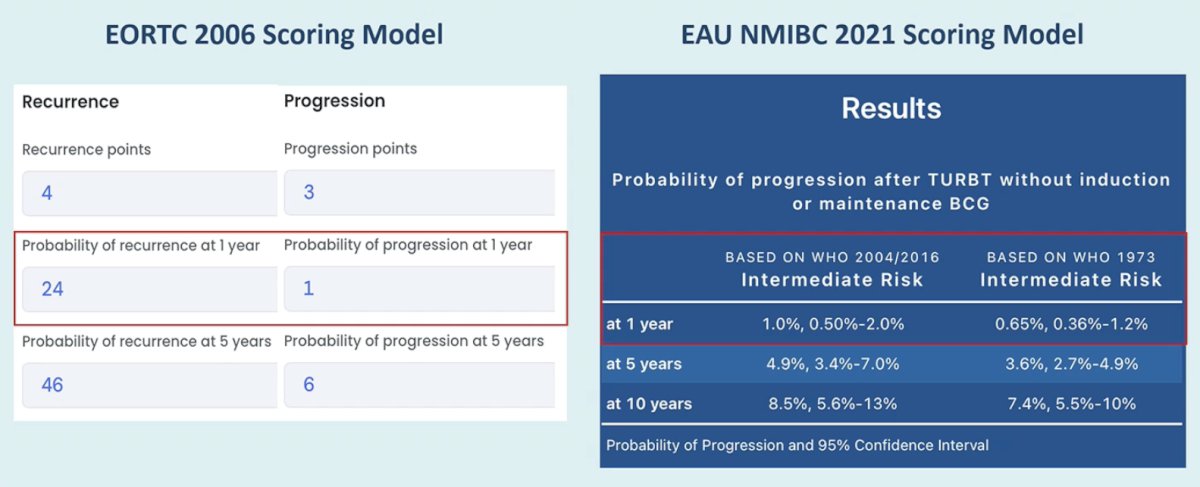
Using the EORTC 2006 risk calculator, this patient would have a recurrence score of 4 and progression score of 3, translating to an estimated recurrence risk of approximately 24% at 1 year and 46% at 5 years, but a progression risk of only about 1% at 1 year and 6% at 5 years.
Similarly, the updated EAU 2021 NMIBC model demonstrates that intermediate-risk patients have extremely low progression risks when managed after TURBT without BCG: approximately 1% at 1 year, 4.9% at 5 years, and 8.5% at 10 years.
Given this low progression risk, Dr. Teoh questioned whether intensive cystoscopic surveillance remains justified in all patients.
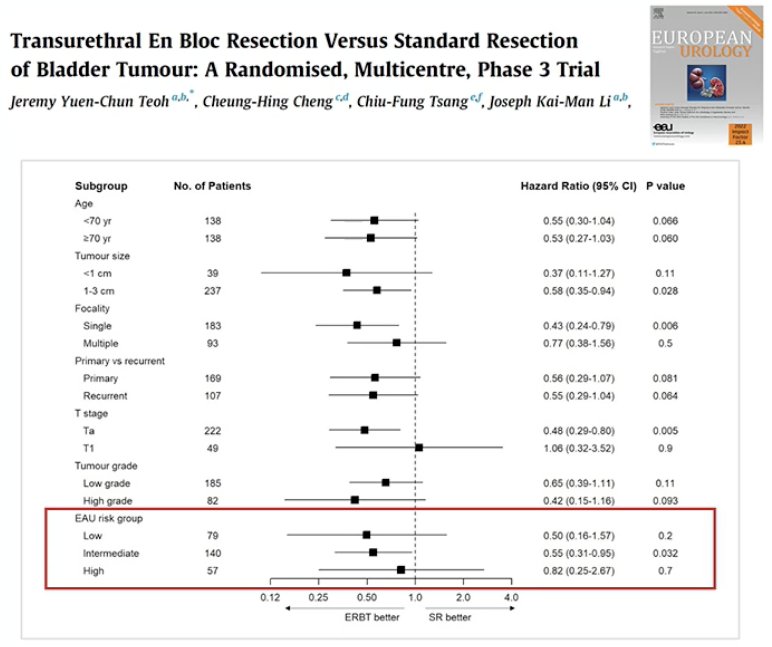
He then highlighted the importance of TURBT quality. In the presented case, an en bloc resection was performed with macroscopically complete removal of the tumor. He referenced EB-StaR, a multicenter randomized phase III trial comparing en bloc resection versus conventional TURBT, which demonstrated potential improvements in oncologic outcomes with en bloc techniques. In subgroup analyses, en bloc resection was associated with reduced recurrence rates (1-year: 29% versus 38%), particularly in low-grade and EAU low-risk disease categories.1
Dr. Teoh argued, as such, that high-quality resection may further reduce the need for intensive surveillance in selected patients, particularly in an elderly patient with significant comorbidities, such as the patient presented earlier by Dr. Gontero. The EAU guidelines have recently incorporated a section entitled ‘Pragmatic Deintensification Strategy in NMIBC’ to highlight the growing relevance of de-intensification approaches in select patients.
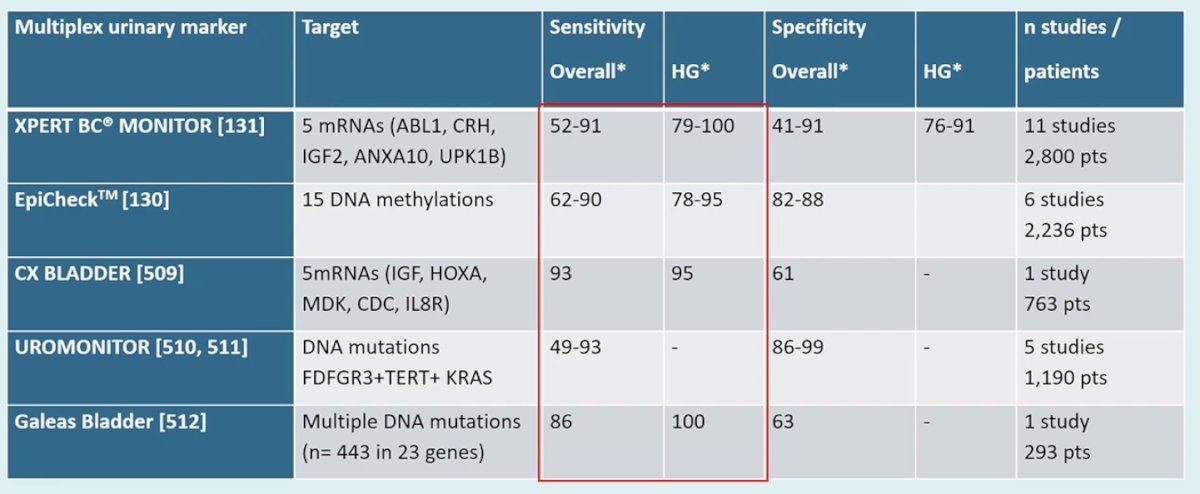
Discussing the diagnostic performance of contemporary urinary biomarkers, Dr. Teoh noted that several multiplex urinary assays have demonstrated improved diagnostic accuracy compared with earlier generations of biomarkers:
- XPERT BC Monitor: Targets five mRNAs (ABL1, CRH, IGF2, ANXA10, and UPK1B) and has reported overall sensitivities ranging from 52% to 91% and high-grade sensitivities of 79–100%, with specificities between 41% and 91% overall and 76–91% for high-grade disease across 11 studies involving approximately 2,800 patients.
- EpiCheck: Evaluates 15 DNA methylation markers and demonstrates sensitivities of 62–90% overall and 78–95% for high-grade tumors, with specificities of approximately 82–88% across six studies, including over 2,200 patients.
- CxBladder: Measures five mRNA targets (IGF, HOXA, MDK, CDC, and IL8R), reports sensitivities of approximately 93% and high-grade sensitivity around 95%, though specificity is more modest at approximately 61%.
- Uromonitor: Detects FGFR3 and TERT promoter mutations and has demonstrated sensitivities ranging from 49–93% with specificities of 86–99% across multiple studies.
- Galeas Bladder: Evaluating multiple DNA mutations across 23 genes demonstrated sensitivity around 86% and specificity around 63% in an early cohort of 293 patients.
Following this, Dr. Teoh highlighted emerging level 1 evidence supporting marker-guided surveillance.
The non-inferiority, randomized DaBlaCa-15 trial evaluated the Xpert Bladder Cancer Monitor (XBCM) in patients with high-grade NMIBC. In this non-inferiority study, 392 patients were randomized to XBCM-based surveillance versus standard cystoscopy-based surveillance. In the experimental arm, XBCM was used at 12- and 24-month visits to determine whether cystoscopy could be safely omitted. The primary endpoint was recurrence-free survival, defined as detection of high-grade NMIBC, MIBC, or metastatic urothelial carcinoma.
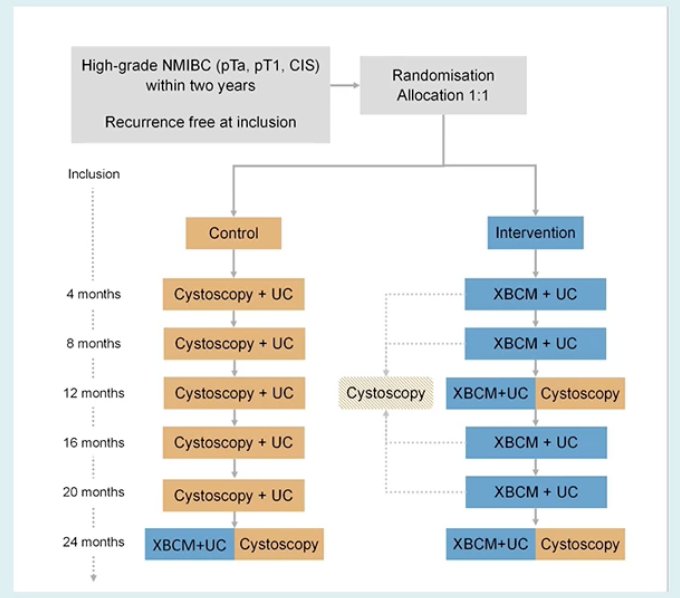
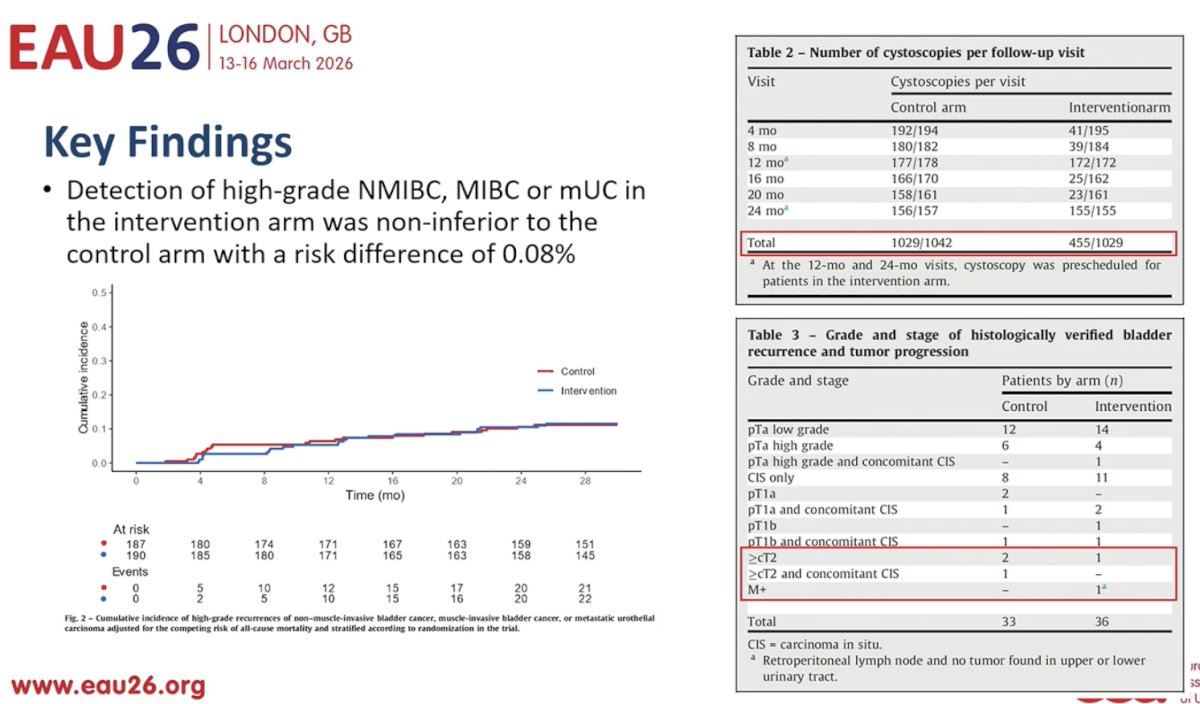
Results showed that detection of high-grade NMIBC, muscle-invasive disease, or metastatic disease in the intervention arm was non-inferior to the control arm, with a risk difference of only 0.08%. Importantly, the number of cystoscopies performed was almost halved: 455 cystoscopies in the marker-guided arm compared with 1,029 cystoscopies in the standard surveillance arm. There were no differences in the proportions of patients who progressed to ≥cT2 disease.2
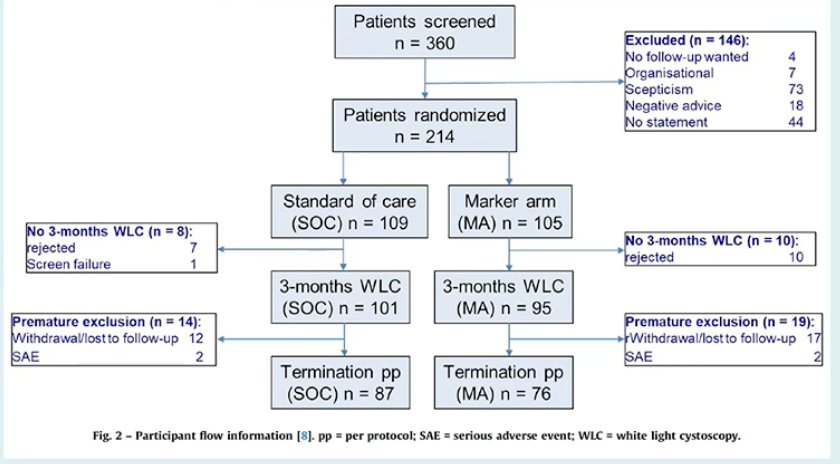
Another key randomized study in this space is the UroFollow trial, which compared marker-based surveillance with cystoscopy-based surveillance in patients with low- and intermediate-risk bladder cancer.3 In this non-inferiority study, 214 patients with Ta low-grade (G1–2) tumors were randomized. The marker-guided arm used urinary markers and ultrasound after the initial 3-month cystoscopy, whereas the control arm underwent standard cystoscopic surveillance. The primary endpoint was detection of greater than 80% of tumor recurrences.
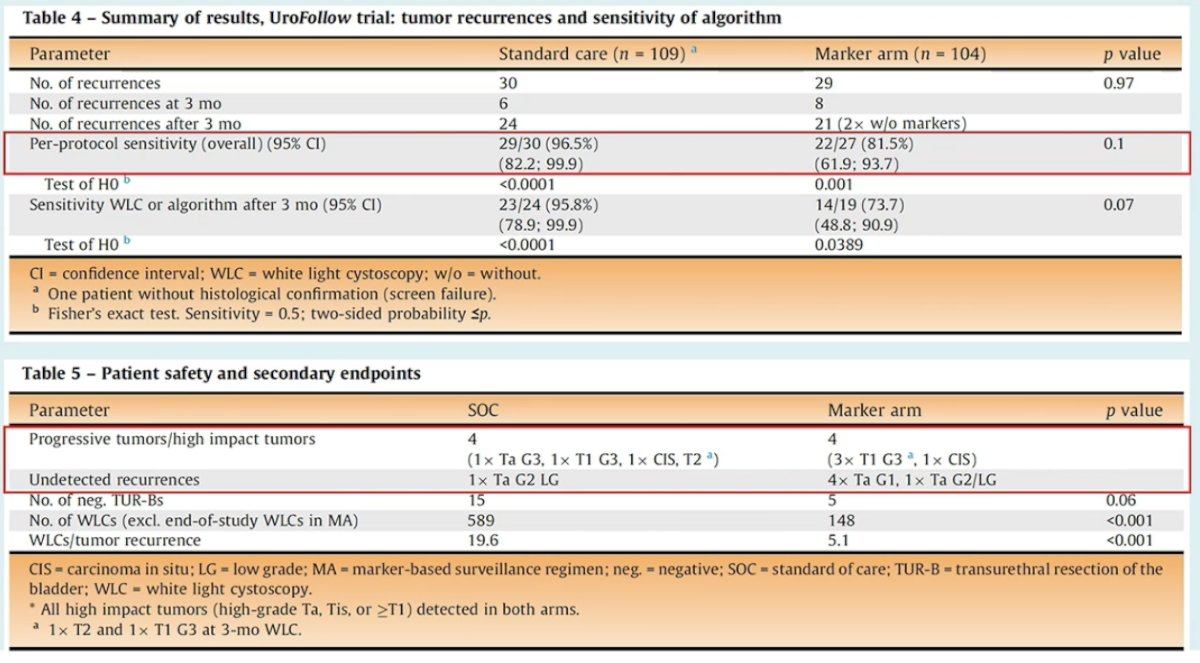
Per-protocol analysis demonstrated that recurrences were detected in 29 of 30 patients (96.5%) in the standard arm and in 22 of 27 patients (81.5%) in the marker arm. Among the few undetected recurrences in the marker-guided arm were four TaG1 tumors and one TaG2/LG tumor. Importantly, all high-impact tumors (high-grade Ta/T1 or ≥T1 disease) were detected in both arms.
Similarly, progression events were rare and comparable between arms, with four events in the standard arm and four events in the marker arm. Dr. Teoh argued that these results demonstrate that marker-guided surveillance can safely reduce the burden of cystoscopy without compromising detection of clinically meaningful disease.
Returning to the index case, he emphasized that when recurrence occurred at 37 months, the patient was already 85 years old and the detected lesions were small papillary tumors measuring approximately 5 mm. This raises an important clinical question: in elderly patients with indolent low-grade recurrences, is TURBT always necessary, or could active surveillance be considered?
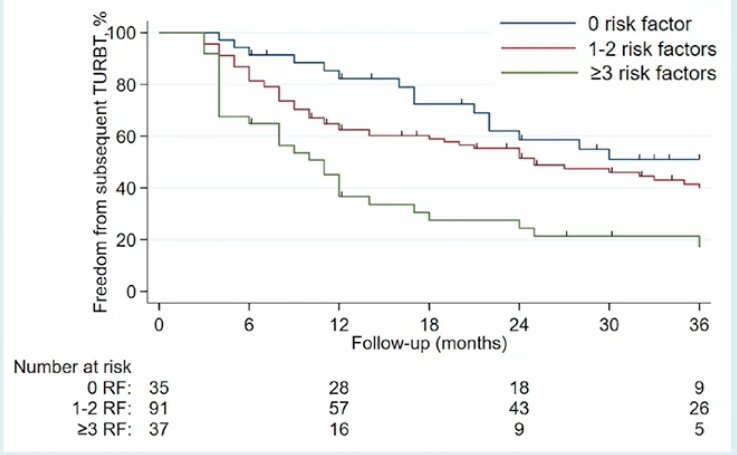
Evidence supporting this concept comes from a prospective cohort study of patients with recurrent low-grade Ta/T1 NMIBC managed with active surveillance. In this study, several risk factors predicted the need for intervention:
- Multifocal tumors
- Early recurrence within one-year
- Frequent recurrences (>1/year)
- Tumor size ≥3 cm
- Prior failure of intravesical therapy.
Patients with none of these risk factors had favorable outcomes, suggesting that conservative management may be appropriate in selected patients.4

Dr. Teoh concluded his argument in favor of urinary biomarkers in place of cystoscopy for surveillance of NMIBC as follows:
- There is an increasing level 1 evidence demonstrating that urinary marker–based surveillance is both safe and feasible.
- Biomarker-based strategies are particularly attractive for patients with low- and intermediate-risk NMIBC, where the risk of progression is low and where the burden of repeated cystoscopy can be substantial
- This approach may be especially relevant in elderly patients with recurrent low-grade disease, where de-intensification of surveillance is becoming increasingly important.
- Surveillance strategies, however, must remain individualized, and that multiple factors—including tumor biology, patient age, comorbidities, and prior treatment history—should be considered when designing the optimal follow-up protocol for patients with NMIBC.
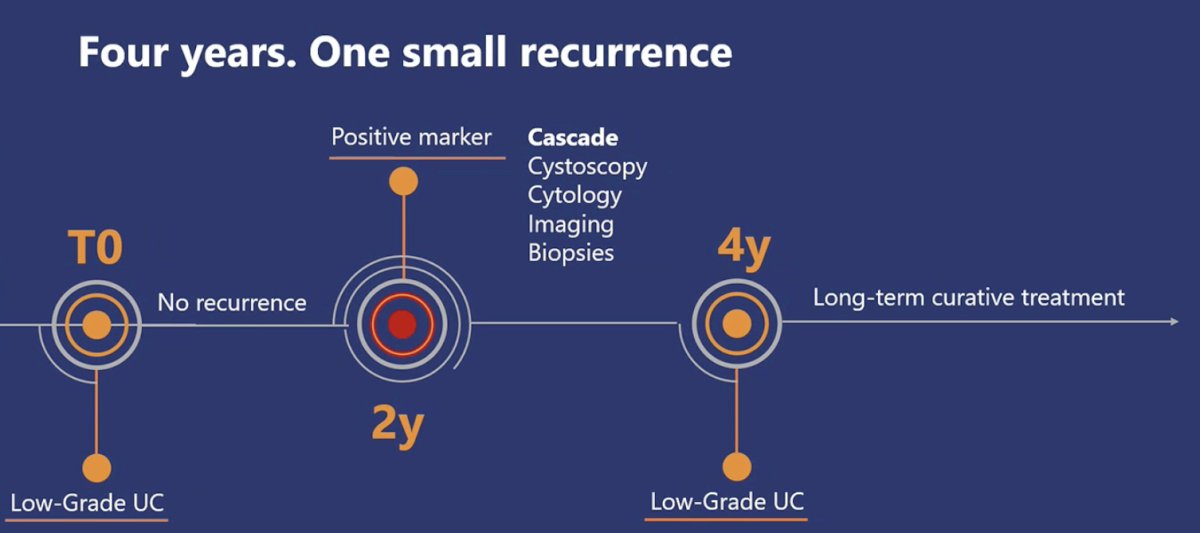
Next, Dr. Laura Mertens argued that urinary biomarkers are not yet ready to replace the gold standard – cystoscopy. She began by returning to the clinical timeline of the index case presented earlier. The patient had low-grade disease at diagnosis and, over four years of follow-up, experienced only one small recurrence. However, during surveillance, a positive urinary marker at two years triggered what Dr. Mertens described as a cascade of downstream investigations, including cystoscopy, cytology, imaging, and biopsies, all of which were negative. The patient ultimately remained recurrence-free for four years, when a small low-grade recurrence was detected. She used this timeline to illustrate the central concern with biomarker-driven surveillance: a single positive marker may initiate multiple investigations without ultimately altering the patient’s clinical course.
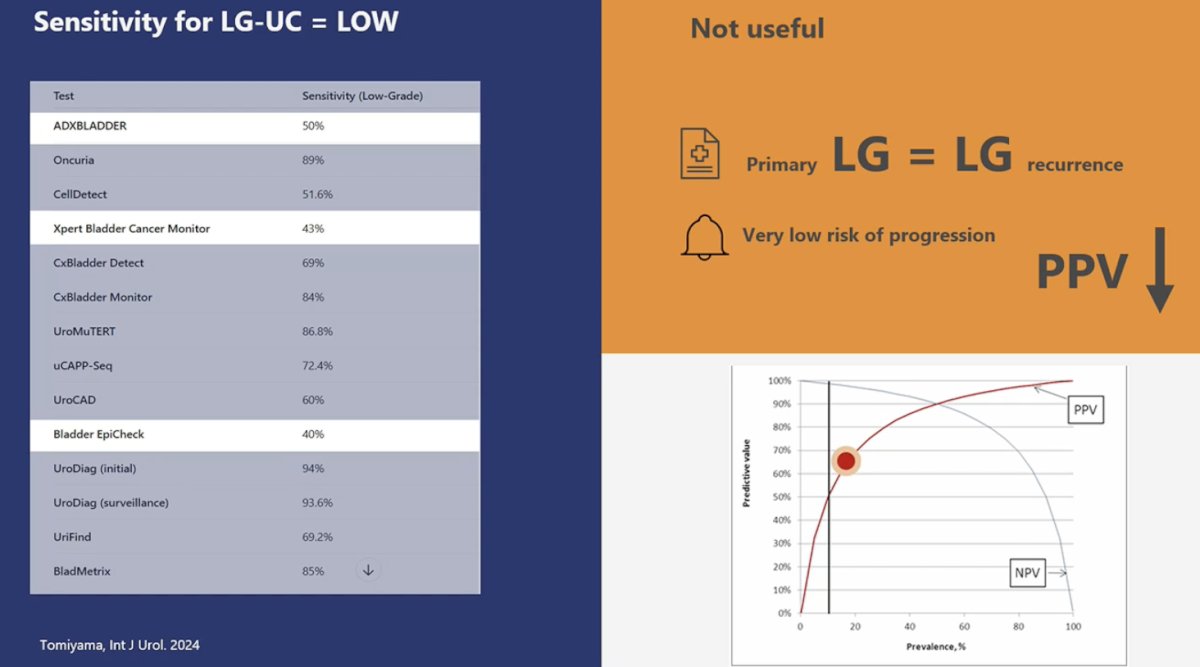
Dr. Mertens then focused on the biological limitations of urinary markers in the context of low-grade disease. She highlighted that most commercially available assays demonstrate poor sensitivity for low-grade urothelial carcinoma. Data summarized from Tomiyama et al. showed wide variability across assays, with reported sensitivities for low-grade tumors ranging from approximately 40–50% for several tests to roughly 70–90% for a minority of assays.5 For example, ADXBLADDER demonstrated sensitivity of approximately 50% for low-grade disease, CellDetect approximately 51.6%, Xpert Bladder Cancer Monitor approximately 43%, and Bladder EpiCheck approximately 40%. Even assays with higher overall sensitivity showed inconsistent performance, specifically in low-grade tumors.
She emphasized that this limitation is particularly important in NMIBC surveillance because the majority of recurrences in patients with low-grade disease are themselves low-grade. As she summarized on the slide, primary low-grade tumors typically recur as low-grade tumors and are associated with a very low risk of progression. Consequently, tests that perform poorly in detecting low-grade disease have limited clinical value when used as substitutes for cystoscopy.
Dr. Mertens next addressed the issue of positive predictive value. Because the prevalence of clinically significant disease during surveillance is relatively low, even tests with moderate sensitivity and specificity may produce a substantial number of false-positive results. She illustrated this using a predictive value curve, demonstrating that as disease prevalence decreases, the positive predictive value falls sharply. In practical terms, this means that many positive biomarker results in surveillance settings may not represent true tumor recurrence.
She then turned to the safety implications of this phenomenon. Dr. Mertens emphasized that specificity represents the key determinant of safety in biomarker-based surveillance strategies. Across multiple urinary markers, reported specificities range roughly between 67% and 97%. For example, ADXBLADDER demonstrated specificity of approximately 67%, CellDetect approximately 70%, Xpert Bladder Cancer Monitor approximately 76.5%, CxBladder Detect approximately 85%, and UroMUTER approximately 94–97% in reported cohorts.
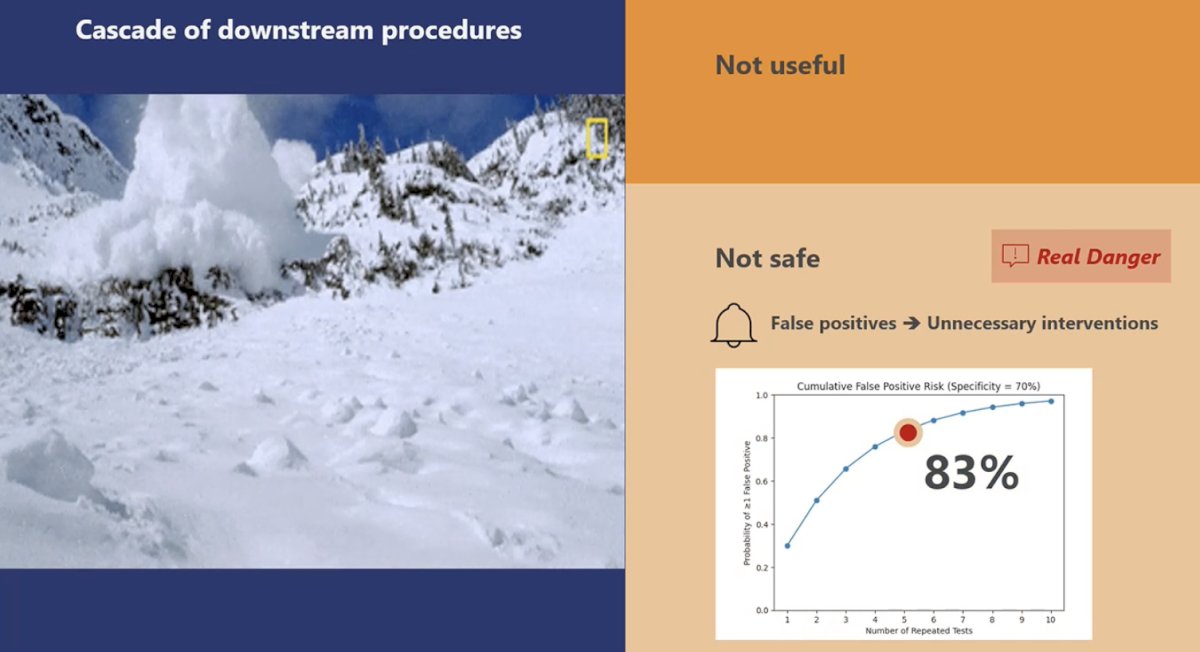
However, she noted that the impact of imperfect specificity becomes magnified with repeated testing. Modeling data presented on the slide demonstrated that with a test specificity of approximately 70%, the cumulative probability of at least one false-positive result increases substantially with repeated surveillance testing. After several rounds of testing, the cumulative false-positive risk may approach 83%. Each of these positive results can trigger additional investigations such as cystoscopy, imaging, or biopsies, even in the absence of true disease.
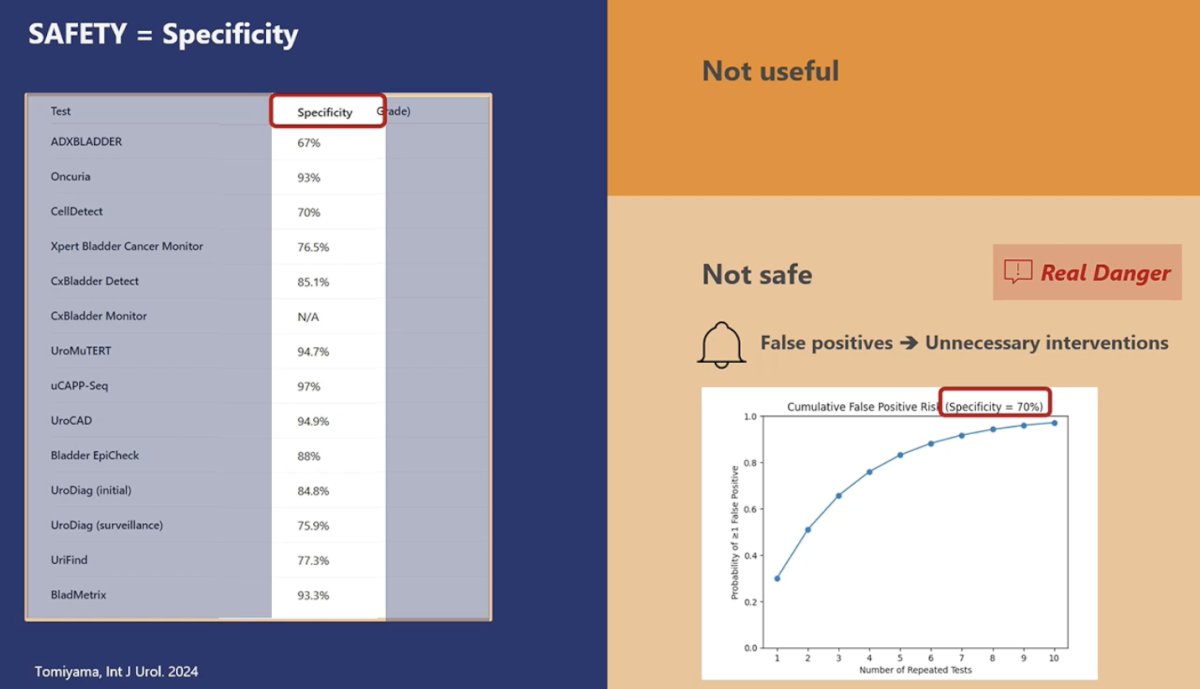
Dr. Mertens illustrated this concept using an avalanche analogy: a single biomarker trigger can initiate a cascade of downstream procedures. In this scenario, a false-positive marker result may lead to cystoscopy, upper tract imaging, cytology, or biopsy, exposing patients to unnecessary interventions without improving outcomes.
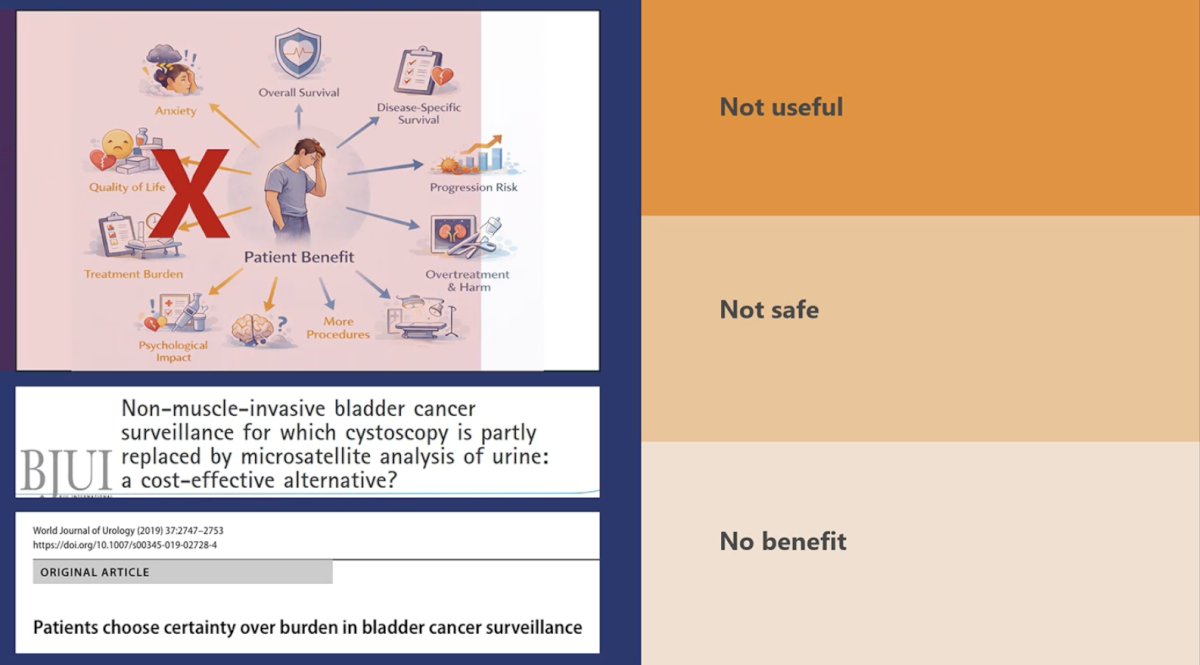
She also addressed the assumption that replacing cystoscopy with biomarkers would necessarily improve patient-centered outcomes. While cystoscopy is invasive and burdensome, data evaluating patient preferences suggest that patients often prioritize diagnostic certainty. She cited work published in BJU International evaluating NMIBC surveillance strategies, which demonstrated that patients frequently prefer approaches that maximize certainty of recurrence detection, even if this involves more invasive testing.6,7
Dr. Mertens, therefore, summarized her position across three key dimensions:
- Urinary markers are not sufficiently useful in the current setting because of limited sensitivity for low-grade tumors
- Biomarker-driven surveillance may not be safe due to cumulative false positives leading to unnecessary downstream procedures.
- Replacing cystoscopy has not yet demonstrated a clear patient-centered benefit.
She concluded by emphasizing that urinary biomarkers remain promising tools, but current evidence does not support abandoning cystoscopy as the standard of care for NMIBC surveillance. Rather than replacing cystoscopy entirely, she suggested that the future lies in smarter integration of biomarkers within surveillance algorithms. The goal should be to “test smarter, not harder.”
Presented by:
- Paolo Gontero, MD, Professor, Chairman Department of Urology, Molinette Hospital, University School of Medicine, Torino, Italy
- Jeremy Teoh, MBBS, FRCSEd (Urol), FCSHK, FHKAM (Surgery), Associate Professor, The Chinese University of Hong Kong, Hong Kong
- Laura S. Mertens, MD, PhD, Nederlands Kanker Instituut, Amsterdam, The Netherlands
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
Related content: Cystoscopy vs Urinary Markers: A Debate on Bladder Cancer Surveillance Strategies - Jeremy Teoh & Laura Mertens