(UroToday.com) The European Association of Urology (EAU) 2026 Annual Congress was host to the “Common Problems and Controversies in Bladder Cancer: Rapid-Fire Debates” session, developed and led by Dr. Ashish Kamat. Dr. Matthew Galsky presented a case study, following which Drs. Thomas Powles and Patrizia Giannatempo debated whether all muscle-invasive bladder cancer (MIBC) patients planned for a radical cystectomy should receive peri-operative immune-oncology (IO)-based therapy or neoadjuvant chemotherapy (NAC) followed by risk-adapted adjuvant IO therapy.
Dr. Galsky presented the case of a 58-year-old woman who initially presented with gross hematuria. Cystoscopy revealed a bladder tumor, and subsequent TURBT demonstrated an invasive high-grade papillary urothelial carcinoma with focal microcystic differentiation, invading into the muscularis propria. Her medical history was notable for type 2 diabetes mellitus. Laboratory testing showed a creatinine of 0.95 mg/dL and a random blood glucose of 170 mg/dL, making her, at least from a renal standpoint, potentially eligible for cisplatin-based therapy.
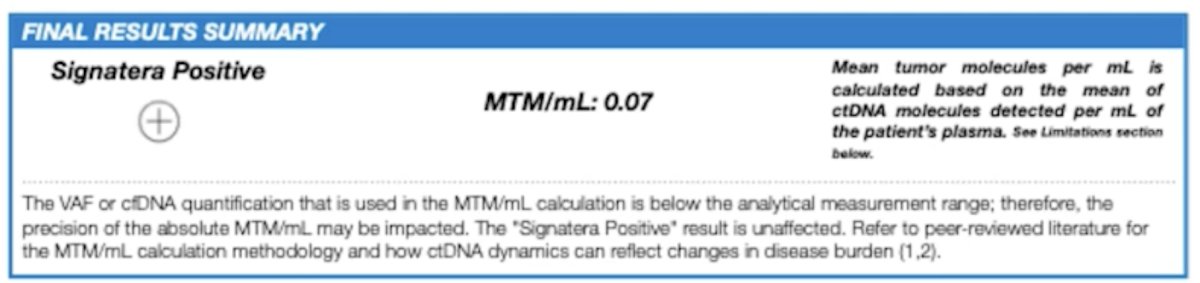
Further staging studies added complexity to the case. CT chest demonstrated a few bilateral punctate pulmonary nodules measuring up to 0.3 cm, while MRI of the abdomen and pelvis revealed a bladder tumor with nodular tissue extension into the perivesical fat, raising concern for cT3 disease. Adding to the biologic risk profile, circulating tumor DNA assessment was positive by Signatera, with a molecular tumor burden of 0.07 MTM/mL. Thus, the audience was presented with a patient who was relatively young, medically fit enough for systemic therapy, had clinically localized but high-risk disease, and already demonstrated evidence of molecular residual disease. This set the stage for the key therapeutic question: in a patient such as this, should one maximize treatment intensity early with peri-operative IO-based therapy, or reserve post-operative immunotherapy in a more selective, risk-adapted fashion?
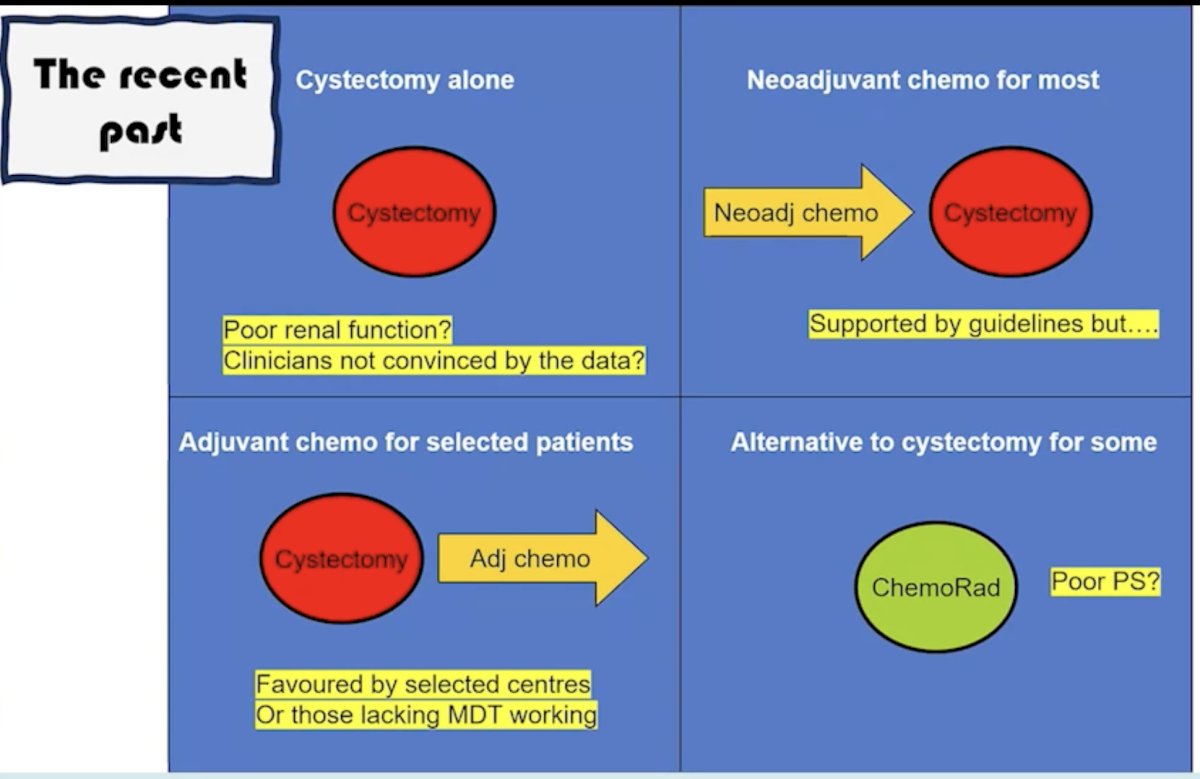
Arguing in favor of immune checkpoint inhibition for all MIBC patients planned for RC, Dr. Powles opened with a broad historical perspective. He contrasted the “recent past” in MIBC, in which many patients still underwent cystectomy alone, neoadjuvant chemotherapy for most, adjuvant chemotherapy for selected patients, or chemoradiation for a subset, with the rapidly evolving present in which peri-operative immunotherapy trials are reshaping the standard-of-care landscape. His message was that the field has moved beyond an era where cystectomy alone or even NAC alone can be comfortably viewed as sufficient for most patients. Rather, early systemic intensification is now generating not only pathologic response benefits, but also event-free survival (EFS) and, importantly, overall survival (OS) gains.
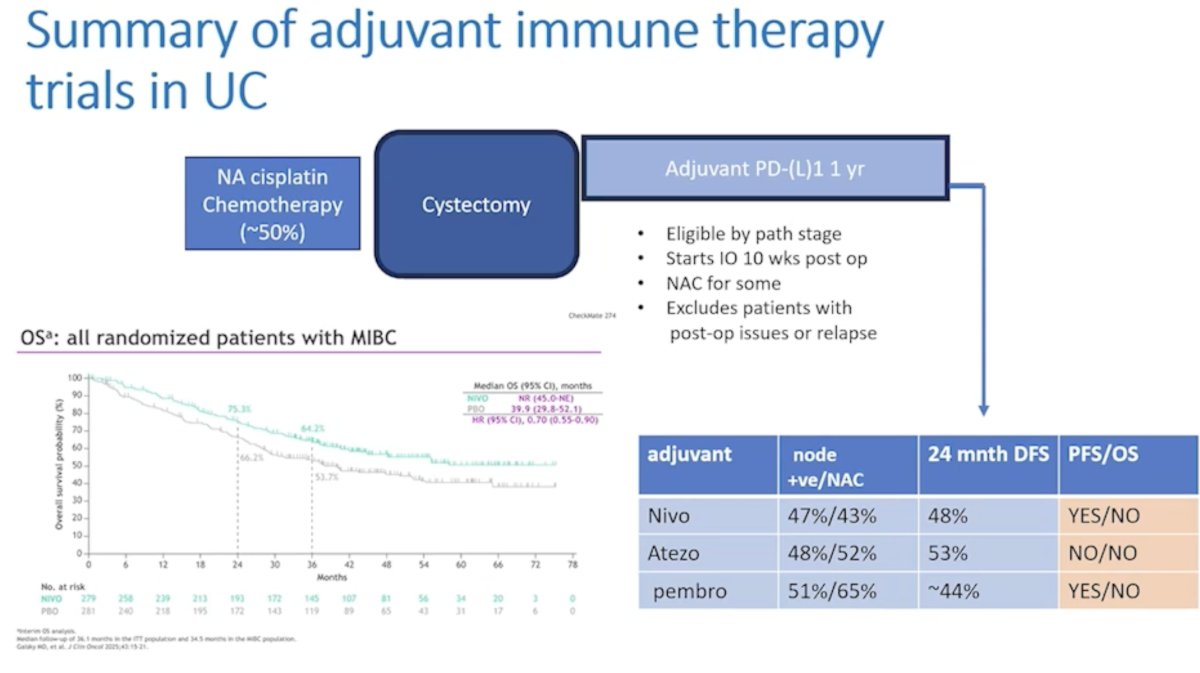
He first reviewed the adjuvant immune therapy experience in urothelial carcinoma to emphasize why a purely post-operative strategy has intrinsic limitations. In his summary slide of adjuvant immunotherapy trials, he noted that only approximately half of patients are candidates for neoadjuvant cisplatin-based chemotherapy and that adjuvant PD-(L)1 therapy is typically started 10 weeks or more after surgery, is based on post-operative pathologic stage, and excludes some patients who experience post-operative complications or early relapse. A concise comparison table highlighted the three major adjuvant IO datasets: nivolumab, atezolizumab, and pembrolizumab.1-3 While the 24-month disease-free survival figures were encouraging, approximately 48% for nivolumab, 53% for atezolizumab, and about 44% for pembrolizumab, the pattern that Dr. Powles emphasized was that progression-free or disease-free endpoints may improve, but overall survival remains less consistently demonstrated in the purely adjuvant setting. This formed a central pillar of his argument: waiting until after cystectomy may miss a meaningful therapeutic window.
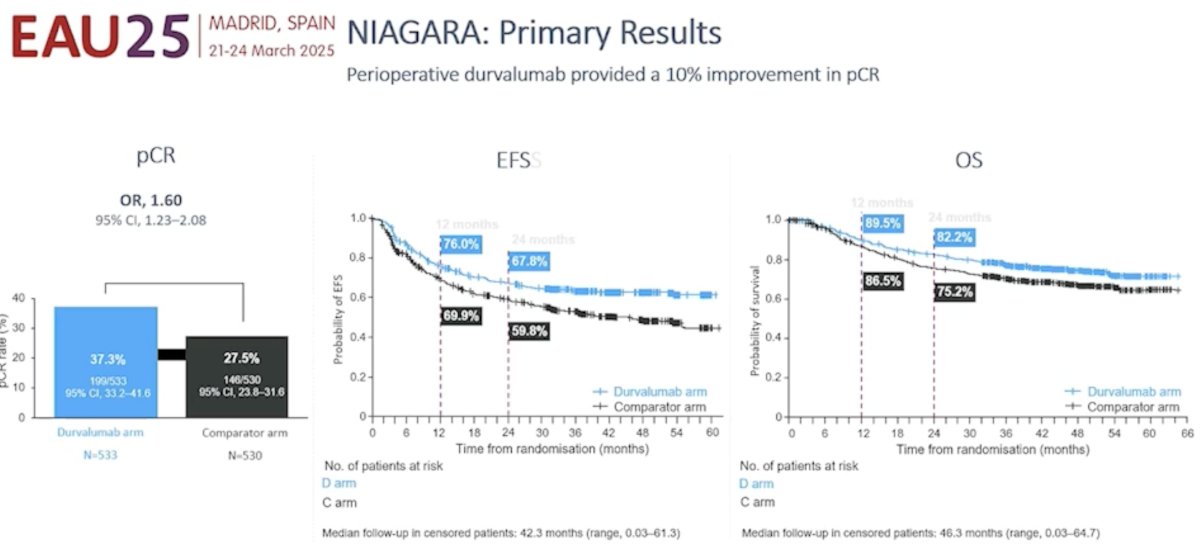
He then pivoted to the NIAGARA trial, which he described as the first immune therapy trial to achieve an overall survival benefit in perioperative bladder cancer.4 This phase III trial enrolled cisplatin-eligible patients with cT2-T4aN0M0 MIBC or clinically node-positive, non-metastatic disease and randomized them to neoadjuvant durvalumab plus gemcitabine/cisplatin for four cycles followed by radical cystectomy and eight cycles of adjuvant durvalumab, versus neoadjuvant gemcitabine/cisplatin followed by cystectomy and no adjuvant treatment. The trial accrued more than 1,000 patients, with 533 assigned to the durvalumab arm and 530 to the comparator arm. Importantly, 88% of patients underwent cystectomy, and there was no signal for increased surgical toxicity. Approximately 75% of patients in the experimental arm started adjuvant therapy, and 50% completed it.
Dr. Powles highlighted that NIAGARA met its dual peri-operative goals while also delivering what he considered the most important endpoint in oncology: overall survival. On the primary results slide, peri-operative durvalumab improved pathologic complete response from 27.5% in the comparator arm to 37.3% in the durvalumab arm, an absolute improvement of approximately 10%, with an odds ratio of 1.60 (95% CI 1.23–2.08). Event-free survival also favored durvalumab, with 12-month EFS estimates of 76% versus 69.9% and 24-month estimates of 67.8% versus 59.8%. Most importantly, the overall survival curves separated early and remained apart: 12-month OS was 89.5% with durvalumab versus 86.5% with chemotherapy alone, and 24-month OS was 82.2% versus 75.2%, respectively. This translated into a hazard ratio for death of 0.75 (95% CI 0.59–0.93). Dr. Powles used these data to argue that early IO-based peri-operative therapy is no longer merely about improving response rates; it is now about saving lives.
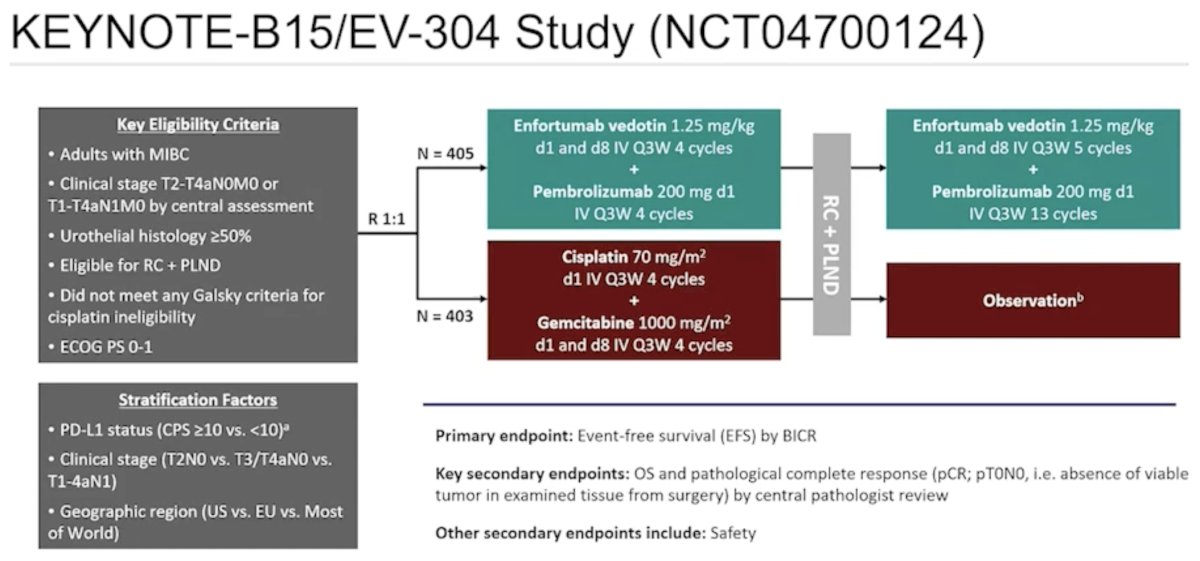
He next turned to KEYNOTE-B15/EV-304, a study that, in his presentation, further strengthened the case for front-loaded peri-operative intensification. This trial enrolled 808 cisplatin-eligible patients with MIBC who were fit for radical cystectomy and pelvic lymph node dissection, randomizing them 1:1 to enfortumab vedotin plus pembrolizumab (EV+P) for four cycles before surgery, followed by adjuvant EV+P, versus standard cisplatin/gemcitabine for four cycles before surgery, followed by observation. The design slide emphasized that this was not simply a chemotherapy substitution study; rather, it was a comprehensive peri-operative regimen testing whether antibody-drug conjugate plus IO therapy could outperform cisplatin-based NAC.
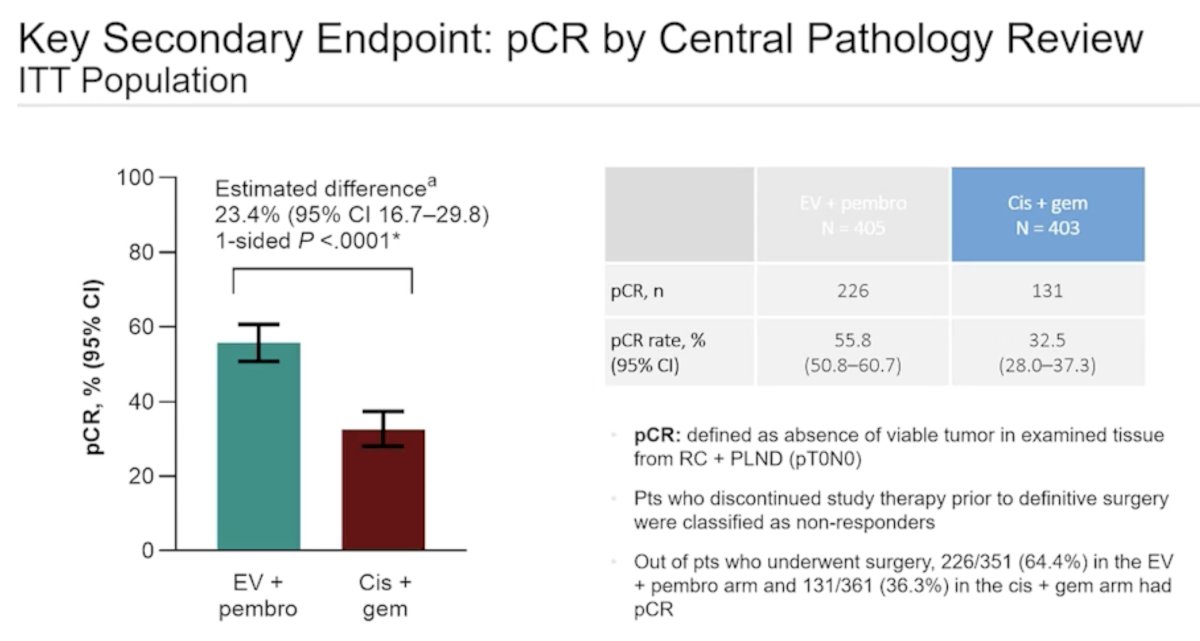
For the key secondary endpoint of pathologic complete response (pCR) by central pathology review in the intention-to-treat population, the pCR rate was 55.8% with EV+P versus 32.5% with cisplatin/gemcitabine, an estimated absolute difference of 23.4% (95% CI 16.7–29.8; one-sided p<0.0001). He also pointed out that among patients who underwent surgery, 226 of 351 patients (64.4%) in the EV+P arm achieved a pCR versus 131 of 361 (36.3%) in the cisplatin/gemcitabine arm.5 Dr. Powles argued that this reinforced the biologic potency of early IO-containing therapy.
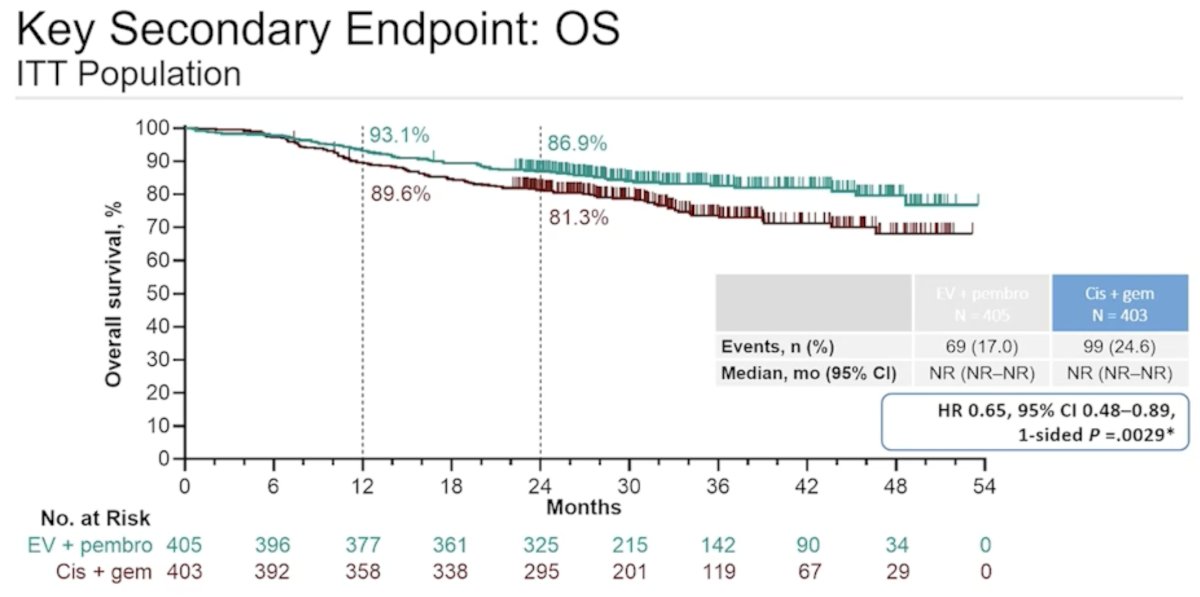
He also highlighted the overall survival signal from KEYNOTE-B15/EV-304. At the time of presentation, the OS curves again favored early IO-based therapy, with 12-month OS of 93.1% versus 89.6% and 24-month OS of 86.9% versus 81.3% for EV+P versus cisplatin/gemcitabine. This corresponded to a hazard ratio for death of 0.65 (95% CI 0.48–0.89; one-sided p=0.0029). These results highlight that early intensification with perioperative IO therapy not only improves pathologic endpoints but also results in fewer recurrences and fewer deaths.
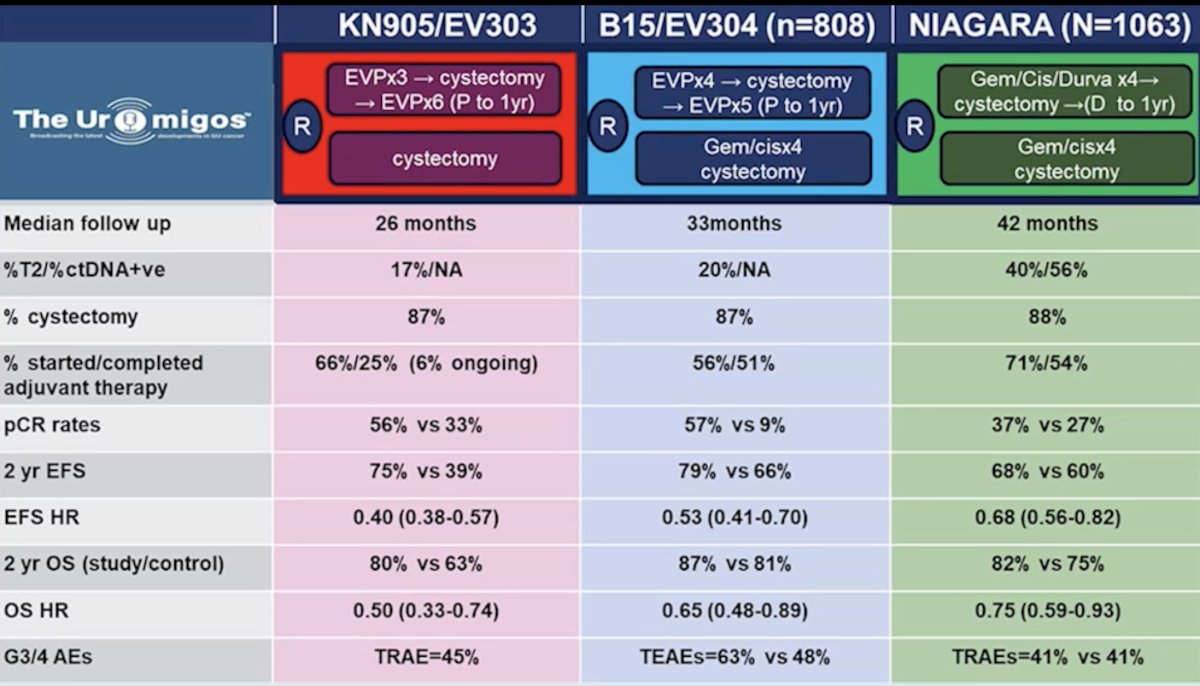
Another important aspect of his argument was that the benefits of perioperative IO are now being seen across multiple studies rather than in a single isolated dataset. One of his comparative summary slides juxtaposed KN905/EV303, B15/EV304, and NIAGARA. The table emphasized several common themes. Median follow-up ranged from 26 months in KN905/EV303 to 33 months in B15/EV304 and 42 months in NIAGARA. Cystectomy rates were high across all three studies, approximately 87% in KN905/EV303, 87% in B15/EV304, and 88% in NIAGARA, helping rebut concerns that pre-operative intensification necessarily compromises definitive surgery. pCR rates were consistently higher in the experimental arms:
- 56% versus 33% in KN905/EV303
- 57% versus 9% in B15/EV304
- 37% versus 27% in NIAGARA
Two-year EFS also favored the experimental arms across studies: 75% versus 39%, 79% versus 66%, and 68% versus 60%, respectively. Most importantly, 2-year OS again favored the experimental regimens, approximately 80% versus 63%, 87% versus 81%, and 82% versus 75%, with corresponding OS hazard ratios of 0.50, 0.65, and 0.75, respectively. This slide reinforces a simple, but forceful point: immune therapy is now repeatedly showing an overall survival advantage in MIBC.
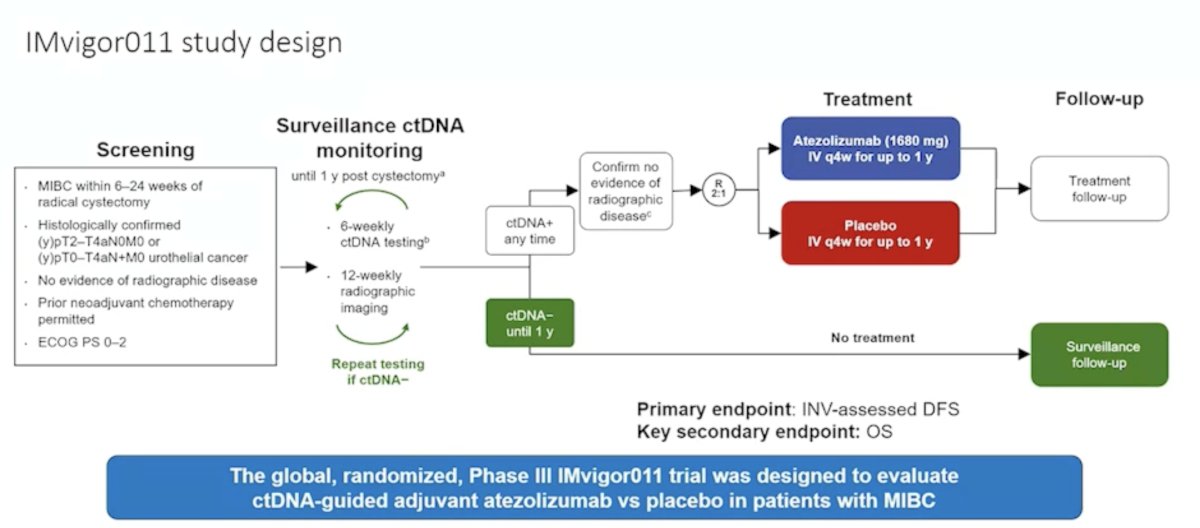
Dr. Powles did, however, acknowledge the potential role of post-operative risk adaptive approaches. He highlighted the ongoing IMvigor011 study, which is evaluating ctDNA-guided adjuvant atezolizumab versus placebo after radical cystectomy in patients with MIBC. In this design, patients undergo serial surveillance ctDNA testing every 6 weeks with imaging every 12 weeks; those who become ctDNA-positive are randomized to atezolizumab or placebo, whereas ctDNA-negative patients continue surveillance. Dr. Powles acknowledged that this is an intellectually appealing strategy and directly relevant to the case presented by Dr. Galsky, whose patient was already Signatera-positive. However, his framing was that while such studies are important, they do not yet override the now-available randomized evidence supporting early peri-operative immunotherapy.
Dr. Powles concluded his argument in favor of perioperative IO therapy for all MIBC patients receiving neoadjuvant chemotherapy prior to radical cystectomy, as follows:
- Things are changing rapidly in bladder cancer, with four immune therapy trials now achieving overall survival gains in MIBC.
- Early immune therapy saves lives in MIBC.
- Although not all patients have molecular residual disease prior to neoadjuvant treatment, the overall population remains at sufficiently high risk that the balance strongly favors early immune therapy for all rather than delayed, selective escalation.
- The field may ultimately be moving toward a model in which enfortumab vedotin plus pembrolizumab is delivered first, and the remaining questions are sorted out afterwards, rather than the reverse.
Taken together, Dr. Powles argued that the center of gravity in resectable MIBC is shifting decisively toward peri-operative IO-based therapy delivered up front. His case was built not on theoretical advantages, but on the convergence of multiple randomized datasets showing improved pCR, improved event-free survival, and, critically, improved overall survival. From that perspective, he contended that clinicians should maximize therapy early rather than reserve immunotherapy only for those who recur or prove to be high risk post-operatively.
Arguing for NAC followed by risk-adapted adjuvant IO rather than universal peri-operative IO for all patients undergoing radical cystectomy, Dr. Patrizia Giannatempo grounded her position in a simple, but important, principle: not every patient needs post-operative immunotherapy, and the field should now move toward better selection rather than blanket escalation.
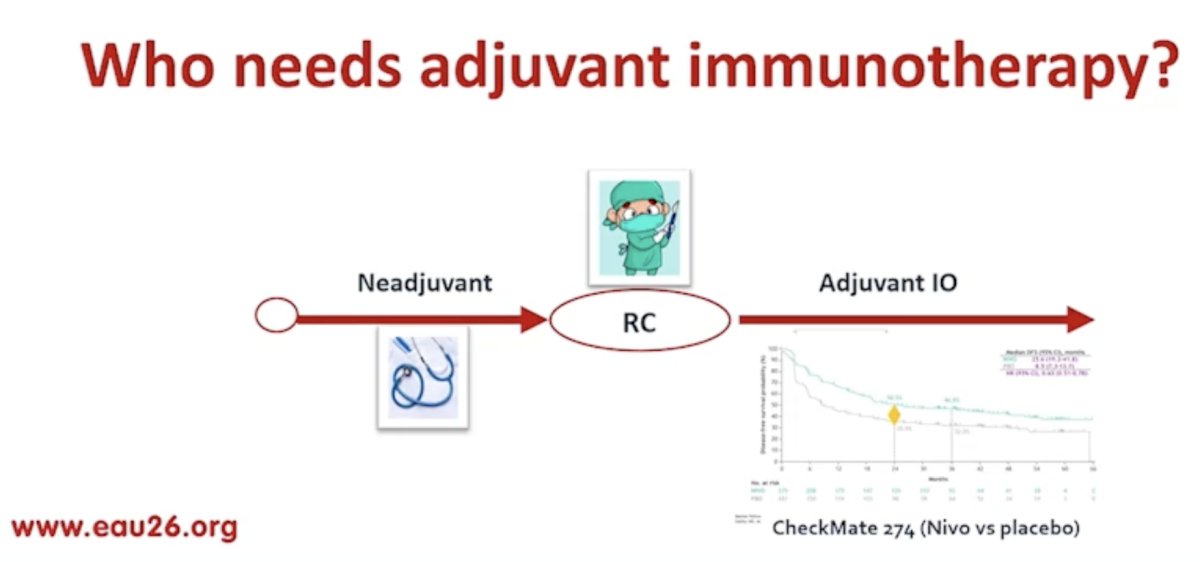
She opened with a conceptual slide asking, “Who needs adjuvant immunotherapy?” The framework was straightforward: patients receive neoadjuvant therapy, undergo radical cystectomy, and only then should clinicians determine whether adjuvant IO is necessary. In her view, the central mistake in an “IO for all” strategy is the assumption that every patient who enters the peri-operative pathway carries the same residual risk after surgery. Her argument was that response to neoadjuvant therapy, and increasingly molecular residual disease assessment, should influence what happens next.
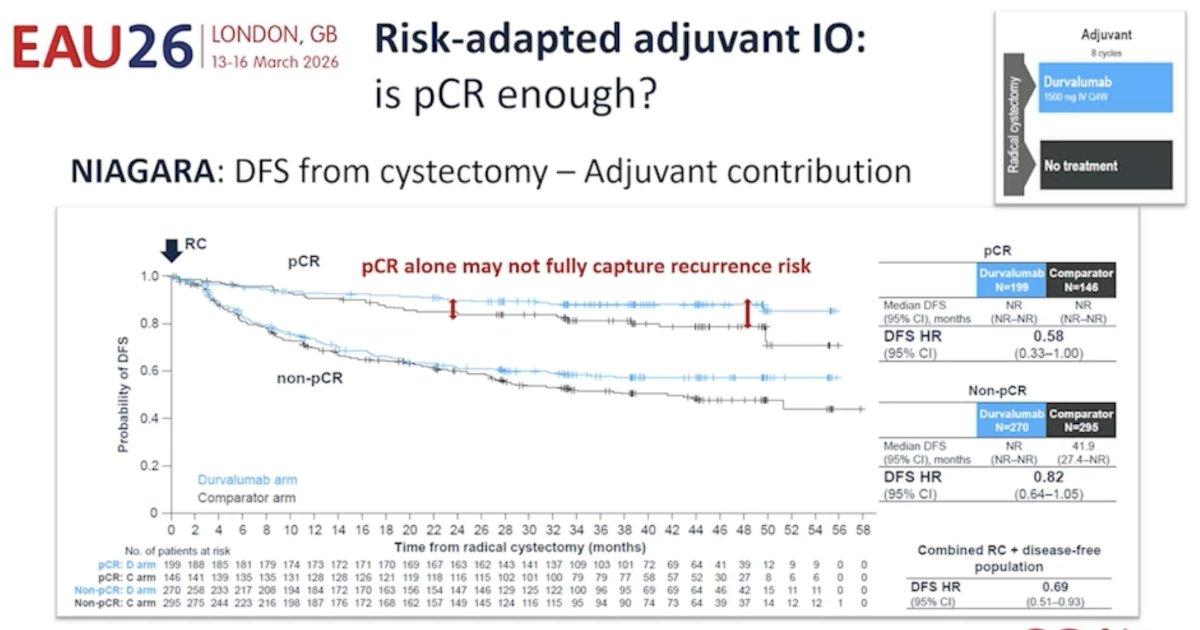
She first focused on the subgroup of patients who achieve a pCR. Her key question was explicit: do we need adjuvant immunotherapy in pCR patients? This was an important pivot in the debate because the pro-escalation argument relies on population-level improvements in peri-operative trials, whereas Dr. Giannatempo’s counterargument emphasized that the decision after surgery should be individualized according to residual risk. She used NIAGARA to explore this question more closely, specifically examining disease-free survival (DFS) from the time of cystectomy in relation to adjuvant contribution.
On the NIAGARA stratified slide, she showed separate DFS curves for pCR and non-pCR patients and highlighted that the contribution of adjuvant durvalumab appears very different across these groups. In the pCR subgroup, the hazard ratio for DFS was 0.58, with the confidence interval extending to 1.00, suggesting possible benefit but also considerable uncertainty. In the non-pCR subgroup, the hazard ratio was 0.82, again with confidence intervals crossing 1.0. Meanwhile, in the combined radical cystectomy plus disease-free population, the DFS hazard ratio was 0.69 (95% CI 0.51–0.93). Her message was not that adjuvant therapy has no role, but rather that these subgroup data do not support the conclusion that all patients, especially those achieving pCR, uniformly require adjuvant IO. She emphasized this further with the annotated message that “pCR alone may not fully capture recurrence risk,” making the point that pathologic response is helpful, but imperfect, as a sole guide for post-operative treatment decisions.
How can ctDNA be helpful in this setting? Dr. Giannatempo argued that minimal residual disease detected by ctDNA provides additional prognostic information beyond conventional pathologic response and can help distinguish patients who truly remain at high risk from those who may safely avoid further treatment.
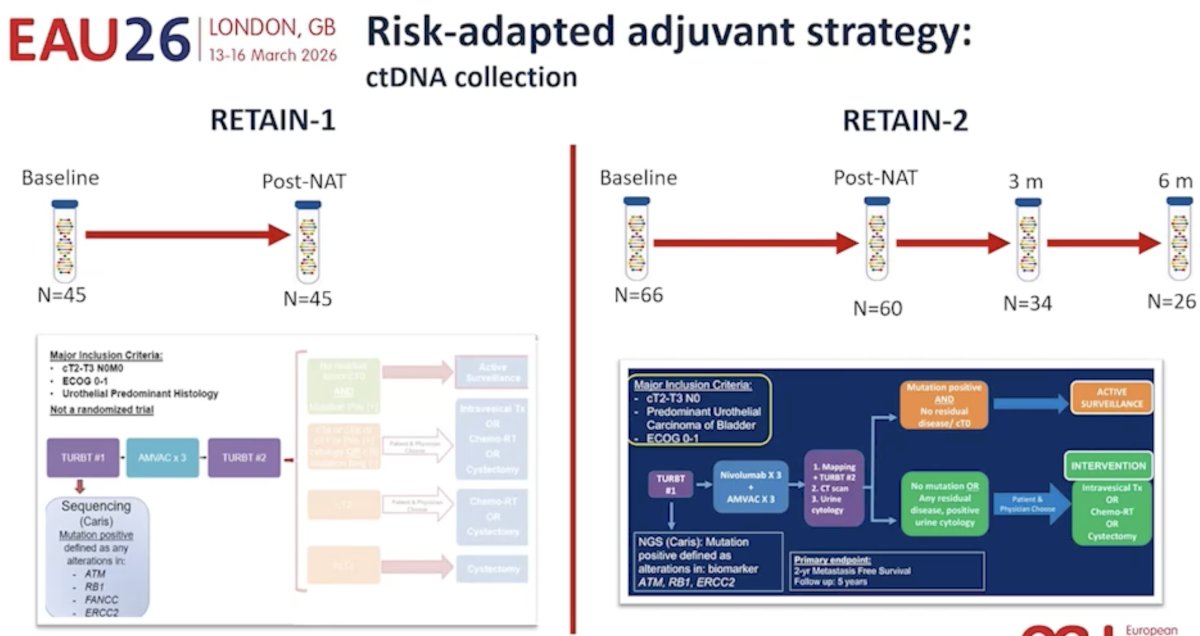
To support this, she reviewed risk-adapted adjuvant strategies from the RETAIN program. On the RETAIN-1 and RETAIN-2 slides, she outlined how serial ctDNA collection was incorporated at baseline, after neoadjuvant treatment, and during longitudinal surveillance. RETAIN-1 included 45 patients with ctDNA collected at baseline and post-neoadjuvant therapy, while RETAIN-2 expanded this concept with 66 baseline samples, 60 post-NAT samples, and additional longitudinal sampling at 3 and 6 months. These studies were not presented as definitive practice-changing trials, but rather as proof-of-principle that ctDNA dynamics can be incorporated into real-world post-operative decision making.
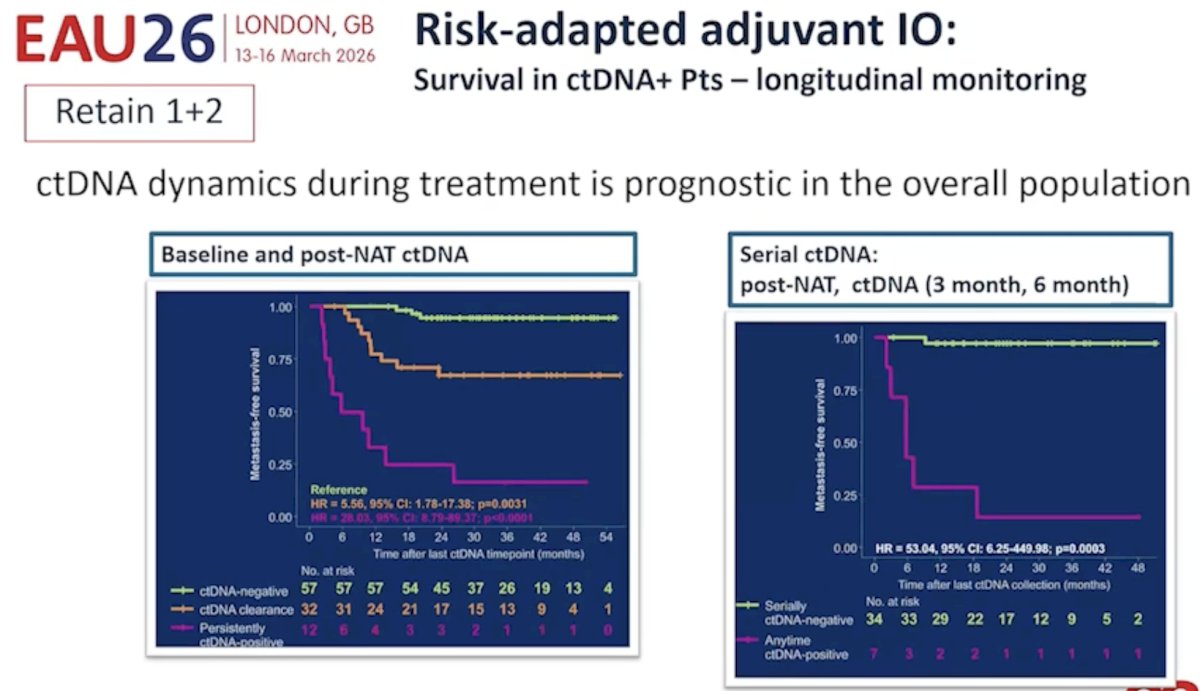
She then showed the longitudinal survival data from the combined RETAIN 1&2 experience. The left panel demonstrated that ctDNA dynamics during treatment were prognostic in the overall population – patients who remained ctDNA-negative had the best metastasis-free survival, those who cleared ctDNA had intermediate outcomes, and those with persistent positivity or conversion fared worst. The right-hand panel reinforced the power of serial monitoring after neoadjuvant therapy, showing a marked divergence in metastasis-free survival between patients who remained serially ctDNA-negative and those who became positive at any point. Her argument was that ctDNA is not merely a binary baseline marker; its dynamics over time may offer a more clinically useful measure of residual disease biology than pCR alone.
From there, Dr. Giannatempo delivered one of the clearest practical takeaways of the presentation: no adjuvant IO for ctDNA-negative patients. She argued that if a patient is ctDNA-negative after radical cystectomy, especially with longitudinal confirmation, these patients may not need further systemic treatment. This was not framed as therapeutic nihilism, but rather as an effort to reduce overtreatment. She used the IMvigor011 trial design to illustrate how the field is moving toward this exact question in a prospective, randomized manner.
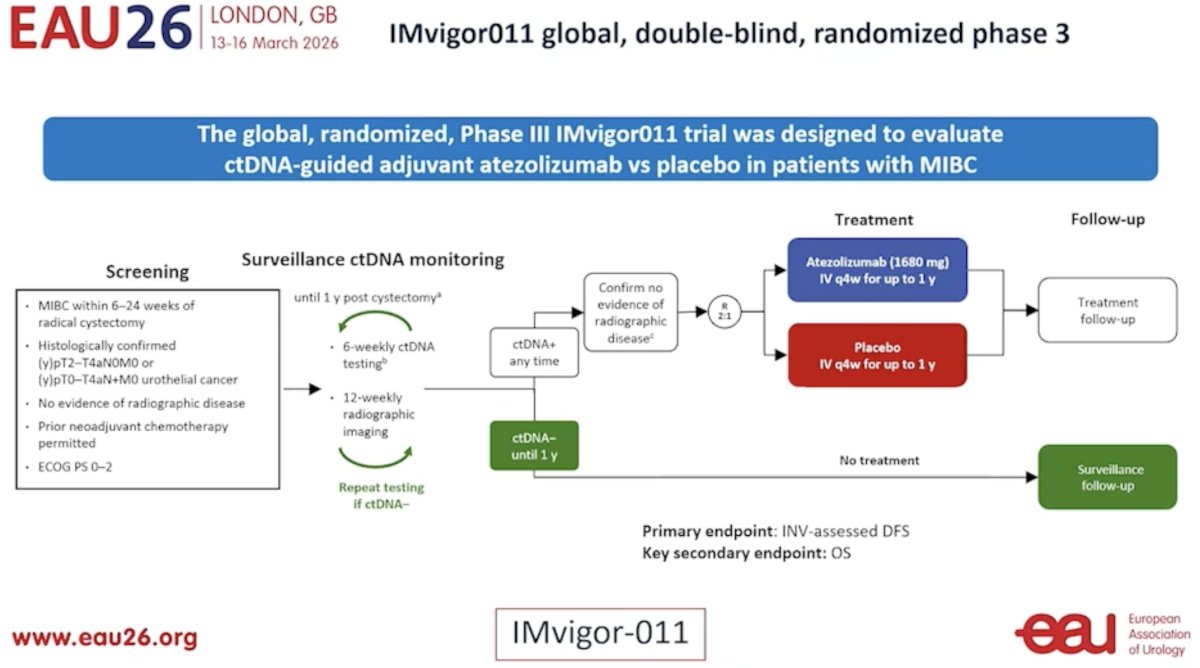
IMvigor011 is a global, double-blind, randomized phase III trial designed to evaluate ctDNA-guided adjuvant atezolizumab versus placebo in patients with MIBC. Surveillance ctDNA monitoring is performed for up to 1 year after cystectomy, with testing every 6 weeks and imaging every 12 weeks. Those who remain ctDNA-negative continue surveillance without treatment, whereas those who become ctDNA-positive are randomized to atezolizumab or placebo after confirmation of no radiographic disease. The primary endpoint is investigator-assessed DFS, with OS as a key secondary endpoint. For Dr. Giannatempo, this study embodies the future direction of the field: not adjuvant IO for everyone, but adjuvant IO for the biologically selected patients most likely to benefit.
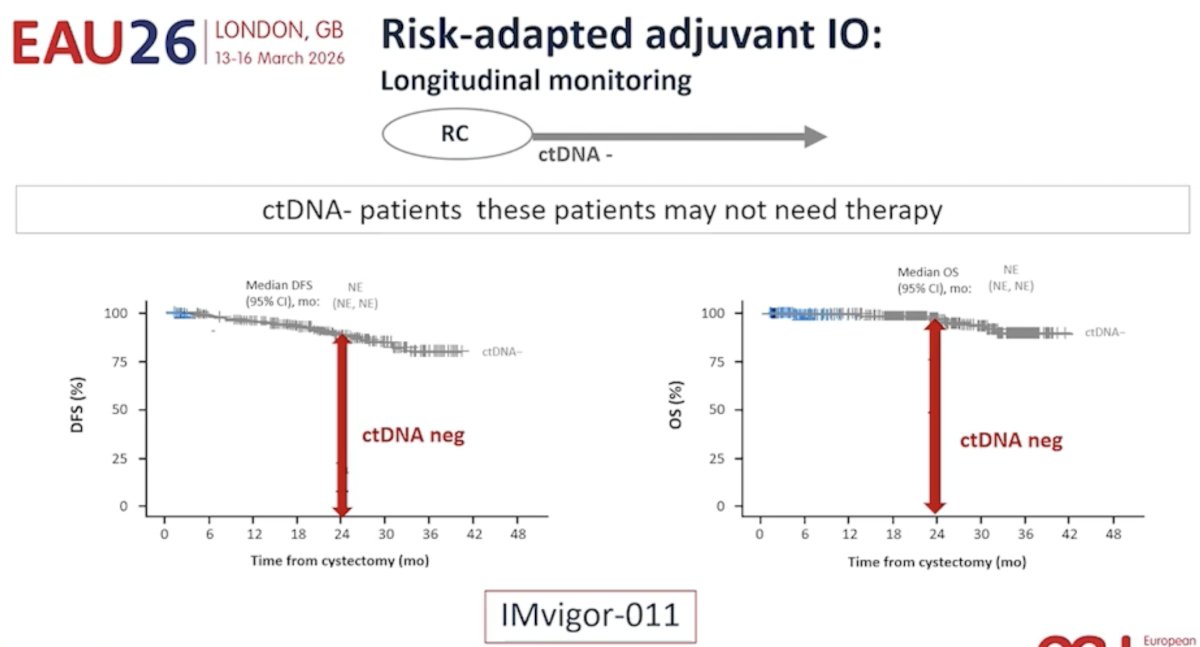
She then highlighted longitudinal IMvigor011 data further supporting this risk-adapted paradigm. In the ctDNA-negative subgroup, both DFS and OS curves were highly favorable, with median DFS and median OS not reached. Her message was clear: patients who remain ctDNA-negative after cystectomy do very well, and this group may be safely observed rather than automatically exposed to a year of adjuvant immunotherapy.
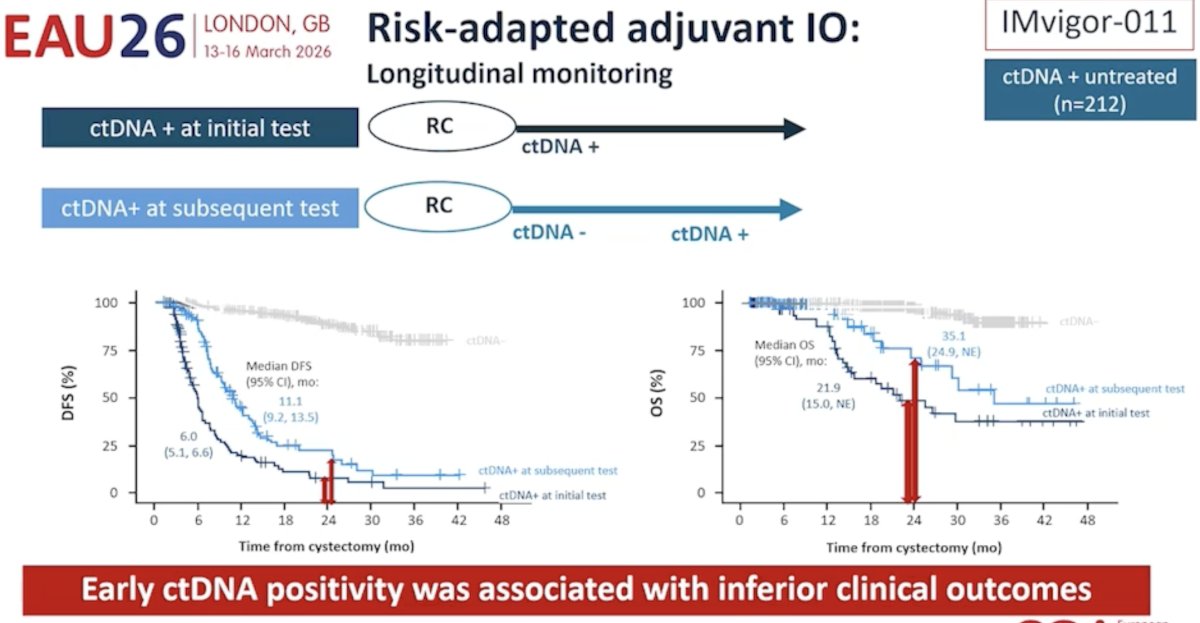
By contrast, early ctDNA positivity was associated with significantly worse outcomes. In the ctDNA-positive untreated cohort from IMvigor011, patients positive at the initial post-cystectomy test had poor DFS, with a median of 6.0 months (95% CI 5.1–6.6), whereas those who first became positive at a subsequent test had somewhat better but still clearly inferior outcomes, with a median DFS of 11.1 months (95% CI 9.2–13.5). The OS panel showed the same pattern: median OS was 21.9 months (15.0, not estimable) for patients positive at the initial test versus 35.1 months (24.9, not estimable) for those converting positive later. Her summary statement on the slide was that early ctDNA positivity was associated with inferior clinical outcomes. This allowed her to refine the post-operative therapeutic question even further: rather than asking whether all patients need peri-operative IO, clinicians should ask which patients are molecularly declaring themselves to be at the highest risk after surgery and therefore most appropriate for escalation.
Dr. Giannatempo’s take home messages from her argument in favor of a risk-adapted approach to adjuvant IO therapy were as follows:
- Risk-adapted approaches aim to reduce overtreatment
- Minimal residual disease detected by ctDNA may provide additional information beyond pathologic responses
- ctDNA assessment, particularly dynamic monitoring, may help refine risk stratification and guide post-operative management.
Taken together, Dr. Giannatempo’s counterargument was that universal peri-operative IO risks overtreating a substantial proportion of patients, particularly those who achieve an excellent response and remain molecularly negative after surgery. While she acknowledged the importance of the recent peri-operative IO datasets, her position was that pCR alone is insufficient to guide all decisions, ctDNA can better capture residual biologic risk, and post-operative immunotherapy should increasingly be deployed in a selective, risk-adapted manner rather than as a one-size-fits-all strategy for every patient proceeding to cystectomy.
Presented by:- Matthew Galsky, MD, Professor of Medicine, Hematology and Medical Oncology, Director of Genitourinary Medical Oncology, Co-Director of the Center of Excellence for Bladder Cancer at The Tisch Cancer Institute, and Associate Director for Translational Research at The Tisch Cancer Institute, New York, NY
- Thomas Powles, MBBS, MRCP, MD, Professor of Genitourinary Oncology, Director, Barts Cancer Centre at St. Bartholomew's Hospital, London, UK
- Patrizia Giannatempo, MD, Genitourinary Medical Oncology, Fondazione IRCCS - Istituto Nazionale dei Tumori. Milan, Italy.
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Bellmunt J, Hussain M, Gschwend JE, et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2021;22(4):525-37.
- Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant Nivolumab versus Placebo in Muscle-Invasive Urothelial Carcinoma. N Engl J Med. 2021;384(22):2102-14.
- Apolo AB, Ballman KV, Sonpavde G, et al. Adjuvant Pembrolizumab versus Observation in Muscle-Invasive Urothelial Carcinoma. N Engl J Med. 2025;392:45-55.
- Powles T, Catto JWF, Galsky MD, et al. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024;391:1773-86.
- Galsky MD, Valderrama BP, Maruzzo M, et al. Neoadjuvant and adjuvant enfortumab vedotin (EV) plus pembrolizumab (pembro) for participants with muscle-invasive bladder cancer (MIBC) who are eligible for cisplatin: Randomized, open-label, phase 3 KEYNOTE-B15 study. J Clin Oncol. 2026;44(7_suppl).