(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a high-risk non-muscle invasive bladder cancer session and a presentation by Dr. Dingwei Ye discussing results of a phase 1/2 study of an anti-PD-L1/IL-15 variant fusion protein (SIM0237) in BCG unresponsive high-risk non-muscle invasive bladder cancer.
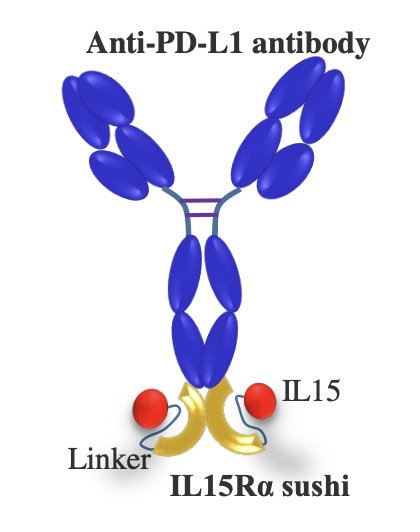
Treatment options for BCG-unresponsive non-muscle invasive bladder cancer are limited. Anti-PD-1 monotherapy and IL-15 agonist in combination with BCG have shown clinical efficacy in BCG-unresponsive CIS non-muscle invasive bladder cancer. However, it remains unclear whether targeting both PD-(L)1 and IL-15 has a synergistic effect in non-muscle invasive bladder cancer. SIM0237 is an anti-PD-L1/IL-15 variant fusion protein, which has shown a good safety profile and promising efficacy signal in patients with BCG-unresponsive non-muscle invasive bladder cancer in the dose escalation part of this trial:
At EAU 2026, Dr. Ye and colleagues reported data from the dose escalation and expansion parts of SIM0237 monotherapy from this ongoing phase 1/2 study.
Patients with BCG-unresponsive high-risk non-muscle invasive bladder cancer received intravesical SIM0237 following the standard induction + maintenance treatment schedule. A re-induction course was allowed if the patients had persistent CIS or high-grade Ta at month 3. Key study endpoints included dose-limiting toxicity, safety, tolerability, pharmacokinetics, and efficacy, defined as (i) the complete response rate and duration of complete response for CIS non-muscle invasive bladder cancer, or (ii) disease-free survival and disease-free survival rate at specific time points for papillary-only non muscle invasive bladder cancer:

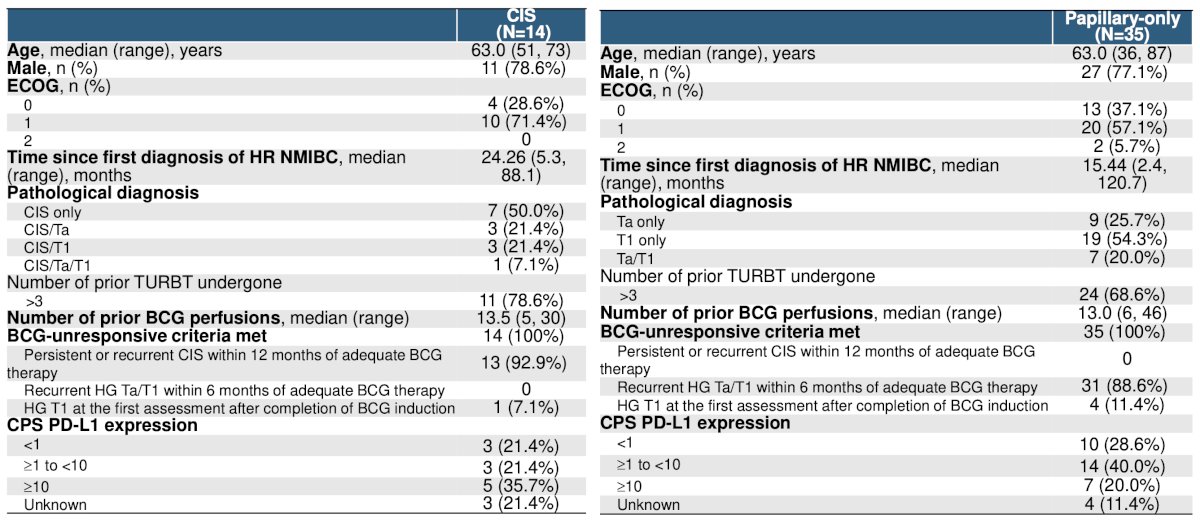
From January 10, 2024, to the data cutoff date of November 28, 2025, a total of 49 patients (14 CIS with or without Ta/T1, 35 papillary-only) have received SIM0237 monotherapy. In the CIS with or without papillary group, the median age was 63 years (range: 51-73), with 78.6% male, and a median number of prior BCG doses of 13.5 (range: 5-30). In the papillary only group, the median age was 63 years (range: 36-87), with 77.1% male, and a median number of prior BCG doses of 13 (range: 6-46):
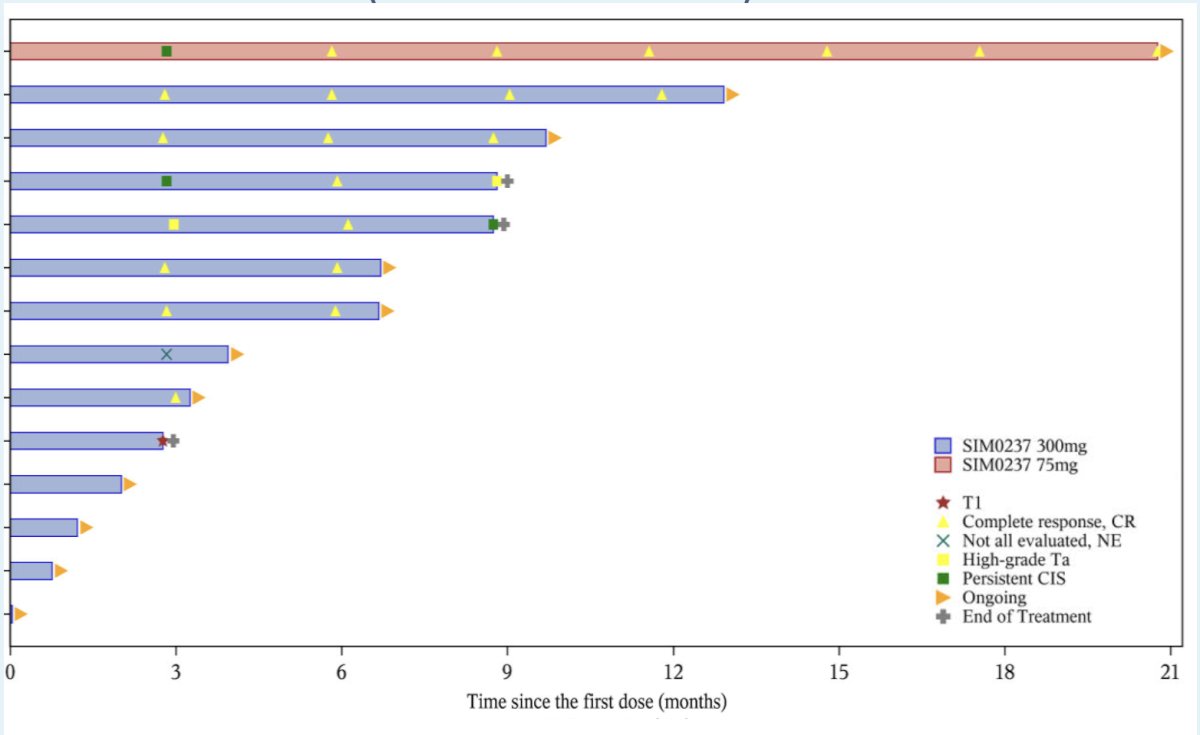
The median follow-up was 6.7 months (range: 0-20.8 months). Of the 10 CIS patients who had at least 1 post-baseline tumor assessment, 8 achieved a best response of complete response, with a median duration of complete response immature, and a probability of duration of complete response 12+ months of 71.4% (95% CI 25.8-92.0%):
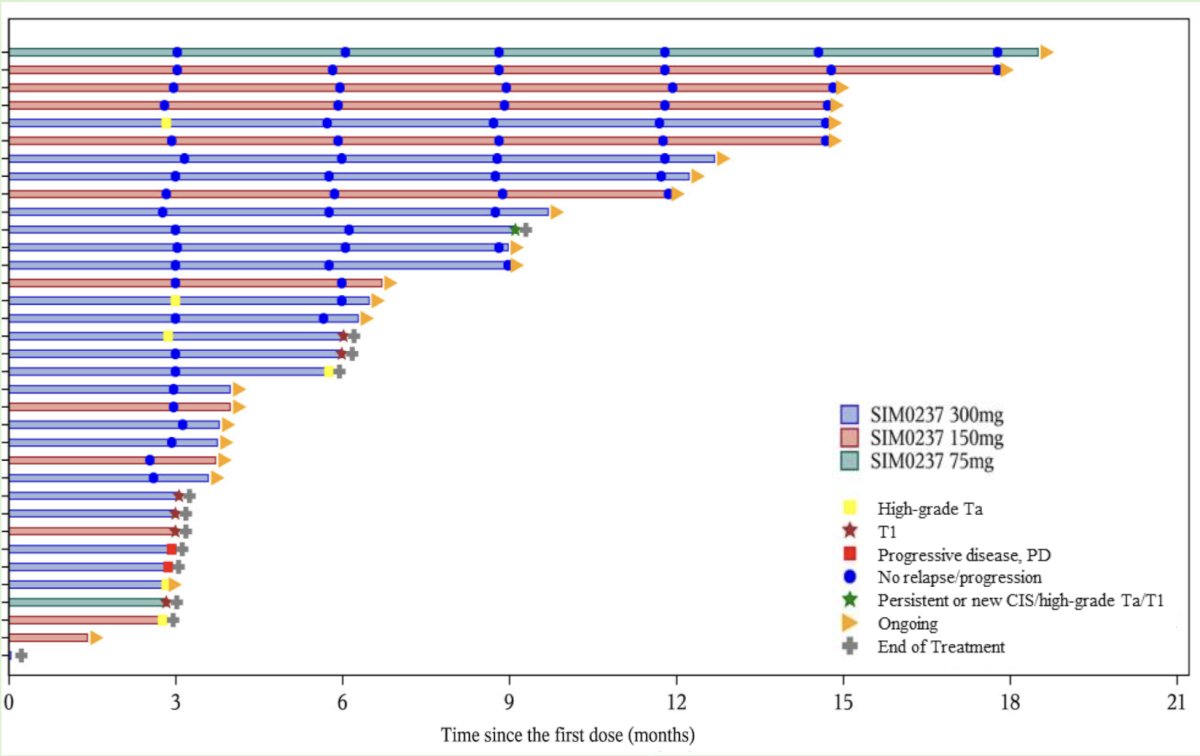
In the 35 papillary-only patients, the median disease-free survival was immature, with a 12-month disease-free survival rate of 65.8% (95% CI, 44.1%-80.7%):
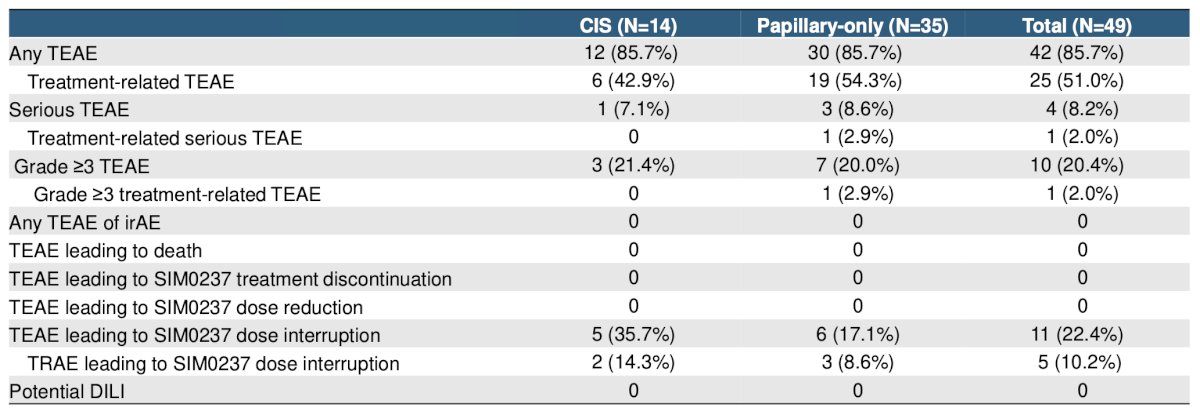
Treatment-emergent adverse events occurred in 42 (85.7%) patients, and 25 (51.0%) patients had treatment-related adverse events. The majority of treatment-related adverse events were grade 1/2 and limited to the urinary system. Overall, there were 10 (20.4%) patients who had grade 3+ treatment-emergent adverse events and 1 (2.0%) grade 3+ treatment-related adverse event. No grade 4 or 5 treatment emergent adverse events were reported. Four (8.2%) patients had serious adverse events, and 1 (2.0%) had a treatment-related serious adverse event of urinary bladder hemorrhage and prostatic hemorrhage. Eleven (22.4%) patients had dose interruptions due to treatment-emergent adverse events, and 5 (10.2%) had dose interruptions due to treatment-related adverse events. There were no dose-limiting toxicities, immune-related adverse events, or adverse events leading to SIM0237 discontinuation. Pharmacokinetics data showed undetectable systemic exposure of SIM0237 in all 29 patients with serum samples analyzed:
Dr. Ye concluded this presentation discussing results of a phase 1/2 study of SIM0237 in BCG-unresponsive high-risk non-muscle invasive bladder cancer with the following take-home points:
- Intravesical SIM0237 was safe and well-tolerated, with promising clinical efficacy in patients with BCG-unresponsive high-risk non-muscle invasive bladder cancer
- A phase 3 study of SIM0237 monotherapy in this patient population is being planned
Presented by: Dingwei Ye, Professor, Fudan University Shanghai Cancer Center, Shanghai, China
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.