(UroToday.com) The 2025 EAU annual meeting featured a session on managing metastatic castration resistant prostate cancer (mCRPC) after triplet therapy for metastatic hormone sensitive prostate cancer (mHSPC) and a presentation by Dr. Wolfgang Fendler discussing when we should be using LuPSMA. Dr. Fendler started his presentation stating that the combination of radioligands for diagnostics and therapy have led to the field of theranostics.
PSMA is a glutamate carboxypeptidase II protein that is highly expressed on primary and metastatic prostate cancer, making it the ideal target for radioligand therapy. The following figure highlights key clinical studies across the prostate cancer landscape using LuPSMA:
Two key trials for LuPSMA radioligand therapy for previously heavily treated mCRPC patients are the TheraP1 and VISION2 trials. TheraP was the first randomized study to evaluate LuPSMA vs cabazitaxel for men with mCRPC after docetaxel. In this open label, phase II trial, 200 men were randomized to either LuPSMA or cabazitaxel. To screen into the study, all men had both 68Ga-PSMA-11 and 18F-FDG PET/CT and were required to have high PSMA-expression (at least one site with SUVmax ≥ 20) and no sites of FDG-positive/PSMA-negative disease. All patients had progressive disease with rising PSA ≥ 20 ng/mL after docetaxel and 91% had received prior enzalutamide or abiraterone. Overall, 200 patients were randomized 1:1 to LuPSMA 6-8 GBq every 6 weeks for up to 6 cycles of therapy or cabazitaxel 20 mg/m2 every 3 weeks for up to 10 cycles. Patients were stratified based on disease burden and prior anti-androgen therapy. The trial schema for TheraP is as follows: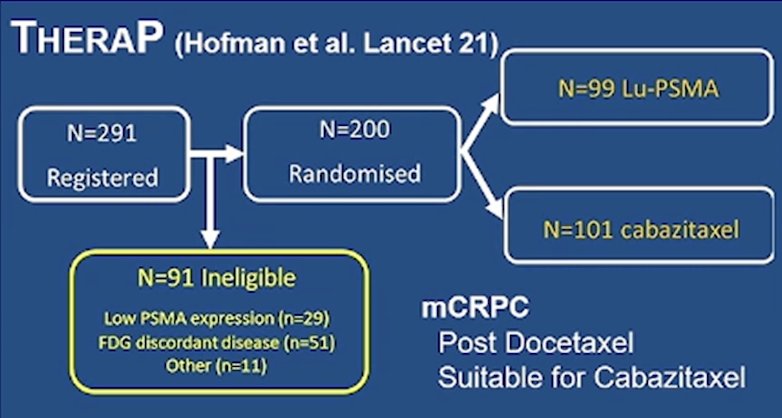
The primary endpoint of this study was a PSA decline of 50% (PSA50) and secondary endpoints included PSA-PFS and overall. After a median follow up of 13 months, LuPSMA significantly improved PSA-PFS compared with cabazitaxel (HR 0.63, 95% CI 0.46 to 0.86) and had a much higher PSA50 rate (66% vs 37%):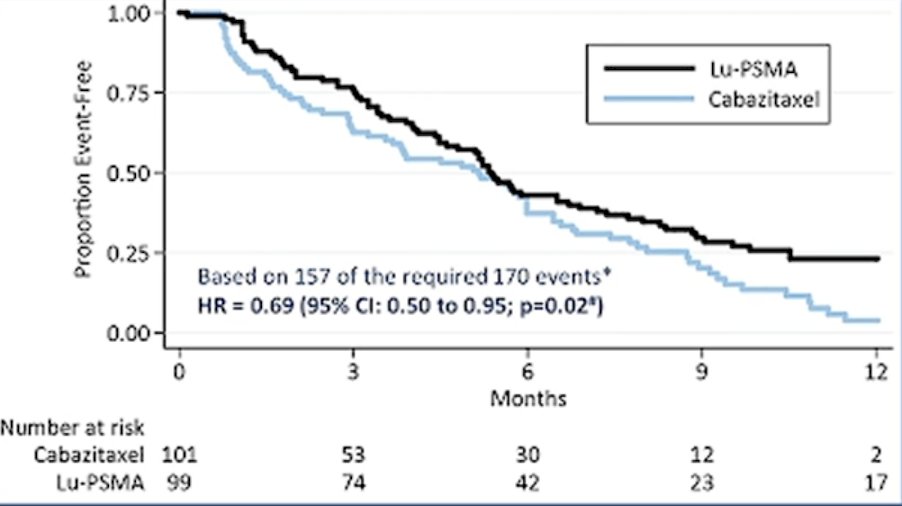
VISION was an international, randomized, open-label phase III study evaluating LuPSMA in men with PSMA-positive mCRPC who had previously received treatment with a next-generation androgen receptor signaling inhibition (abiraterone, enzalutamide, etc) and one or two prior lines of taxane chemotherapy. Patients must have had an ECOG performance status of 0-2 and a life expectancy of at least 6 months. Importantly, patients must have had PSMA-positive disease on the basis of a central review of 68Ga-PSMA-11 staging scans. PSMA positivity was defined as uptake greater in metastatic lesions than in the liver. Furthermore, patients could have no PSMA-negative metastatic lesions. Following enrollment, patients were randomized in a 2:1 fashion to receive either LuPSMA (7.4 GBq every 6 weeks x 6 cycles) plus standard of care or standard of care alone. Standard of care treatments were at the discretion of the treating investigator; however, cytotoxic chemotherapy, immunotherapy, and radium-223 were explicitly excluded. The trial design for VISION is as follows: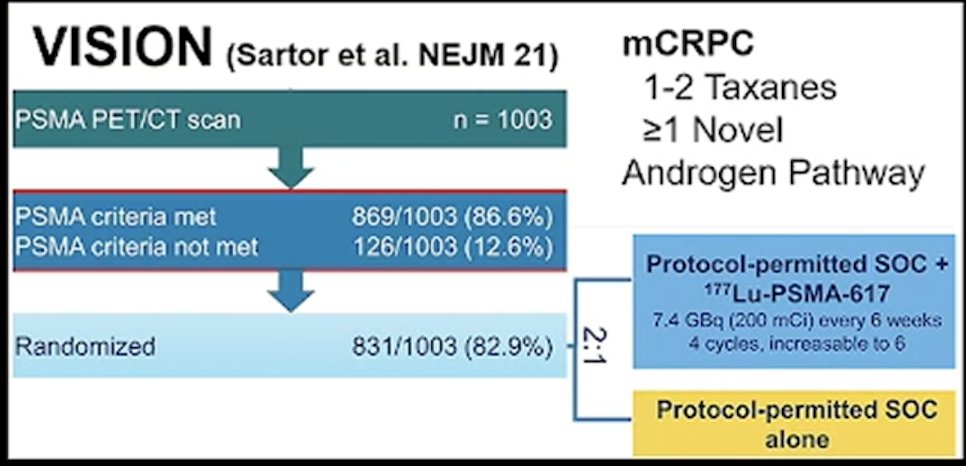
With regards to the co-primary endpoint of radiographic progression free survival, treatment with LuPSMA + standard of care significantly improved radiographic progression free survival by a median 5.3 months (median: 8.7 vs 3.4 months; HR 0.40, 99.2% CI 0.29 to 0.57; p < 0.001, one-sided):
Over a median study follow-up of 20.9 months, treatment with LuPSMA + standard of care significantly improved overall survival by a median of 4.0 months (median: 15.3 vs 11.3 months; HR 0.62, 95% CI 0.52 to 0.74; p < 0.001, one-sided), compared to standard of care alone, in the overall cohort of all randomized patients. Dr. Fendler noted that enrollment after triple therapy was possible in VISION if the patient’s physician deemed him unsuitable to receive a second taxane regimen (ie. frailty assessed by geriatric or health status evaluation or intolerance, etc). This may have been possible, given the time since prostate cancer diagnosis among those in VISION: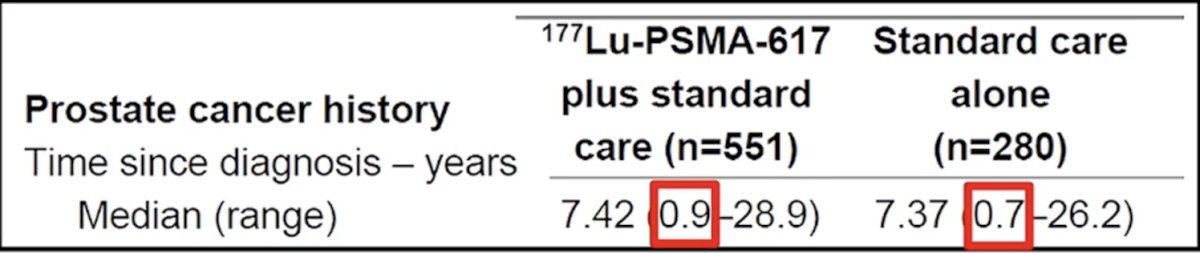
In the second-line setting, Dr. Fendler discussed the PSMAfore trial3 which assessed whether we can use LuPSMA before chemotherapy. Eligible adults for PSMAfore had mCRPC, were candidates for androgen receptor pathway inhibitor change after one progression on prior androgen receptor pathway inhibitor, and had ≥1 PSMA positive lesions and no exclusionary PSMA negative lesions by 68Ga-PSMA-11 PET/CT. Randomization was 1:1 to open-label LuPSMA (7.4 GBq every 6 weeks for 6 cycles) or androgen receptor pathway inhibitor change (abiraterone or enzalutamide). Importantly, patients randomized to androgen receptor pathway inhibitor could crossover to LuPSMA following centrally reviewed radiographic progression. The trial design for PSMAfore is as follows:
At the time of the second data cutoff, the primary endpoint of radiographic progression free survival was met (HR 0.43, 95% CI 0.33 to 0.54), favoring the LuPSMA arm: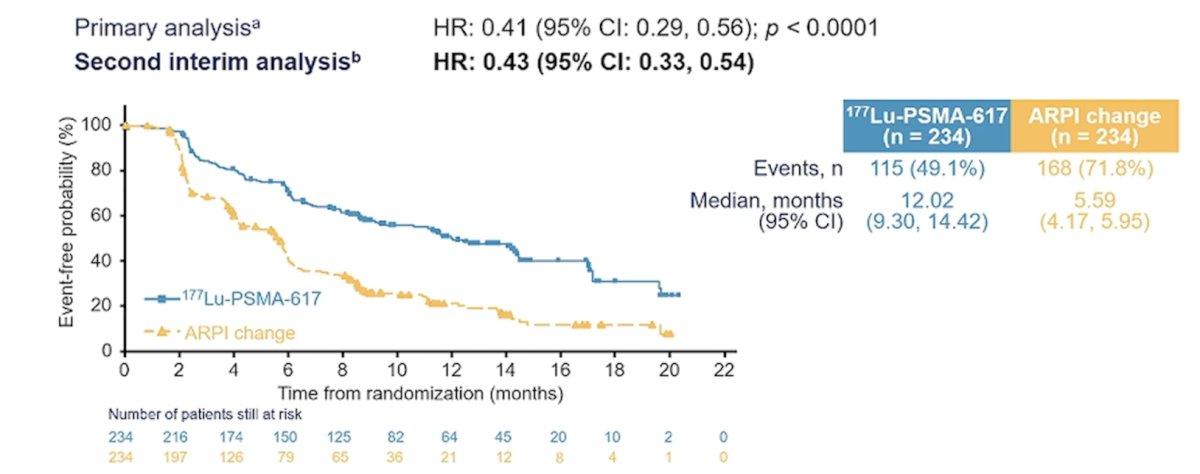
Also in the second line disease space is the SPLASH trial, first presented at ESMO 2024. SPLASH is a phase III, randomized trial evaluating 177Lu-PNT2002 in mCRPC patients experiencing disease progression following an androgen receptor pathway inhibitor. Patients were randomized 2:1 to 177Lu-PNT2002 every 8 weeks for 4 cycles versus the alternative androgen receptor pathway inhibitor (enzalutamide or abiraterone). Patients also had to have PSMA-avid PET imaging and an ECOG performance status of 0-1. The primary endpoint was radiographic progression free survival, and key secondary endpoints included overall survival and safety. Over a median follow-up of ~12 months, the SPLASH trial met its primary endpoint of a radiographic progression free survival benefit with 177Lu-PNT2002 (median: 9.5 versus 6 months; HR 0.71, 95% CI 0.55–0.92):
In the first line setting, particularly in poor risk patients, Dr. Fendler also highlighted the ENZA-p trial.4 ENZA-p randomly assigned 162 participants to enzalutamide 160 mg daily alone, or in combination with (2 or 4 doses) LuPSMA 7.5 GBq. Eligible participants had mCRPC not previously treated with chemotherapy or an androgen receptor pathway inhibitor for mCRPC, 68Ga-PSMA PET-avid disease, and at least 2 risk factors (LDH >= ULN, ALP >= ULN, albumin <35 g/L, de novo metastatic disease at diagnosis, <3 Years since initial diagnosis, >5 bone metastasis, visceral metastasis, PSA doubling time < 84 days, pain requiring opiates > 14 days, prior abiraterone) for early disease progression on enzalutamide-alone: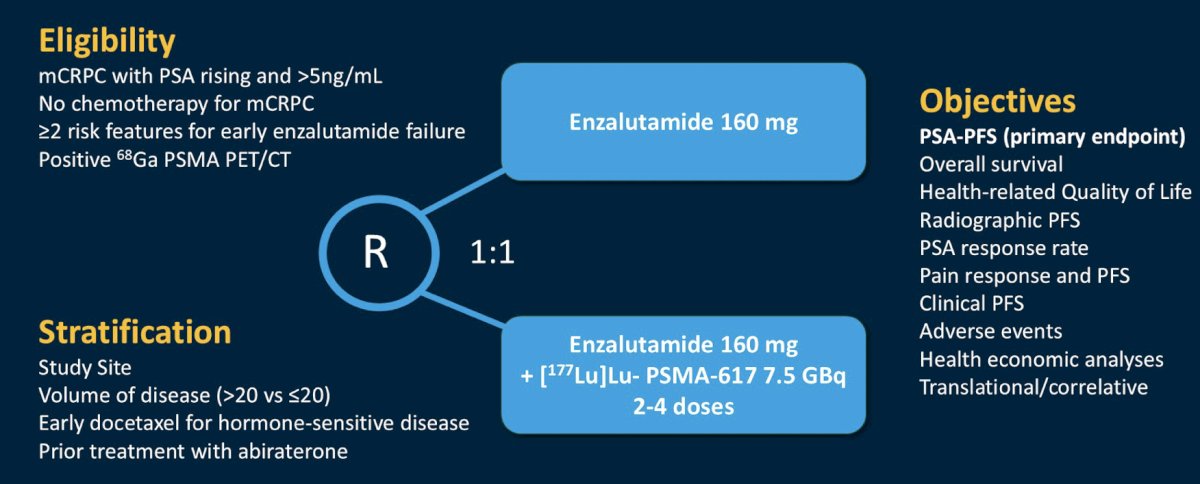
A total of 96 deaths were reported after a median follow-up of 34 months (IQR 29-39): 53 among those assigned enzalutamide-alone and 43 among those assigned enzalutamide + LuPSMA. Overall survival was longer in the enzalutamide + LuPSMA group than the enzalutamide-alone group: median 34 months versus 26 months (HR 0.55, 95% CI 0.36 to 0.84; p = 0.005):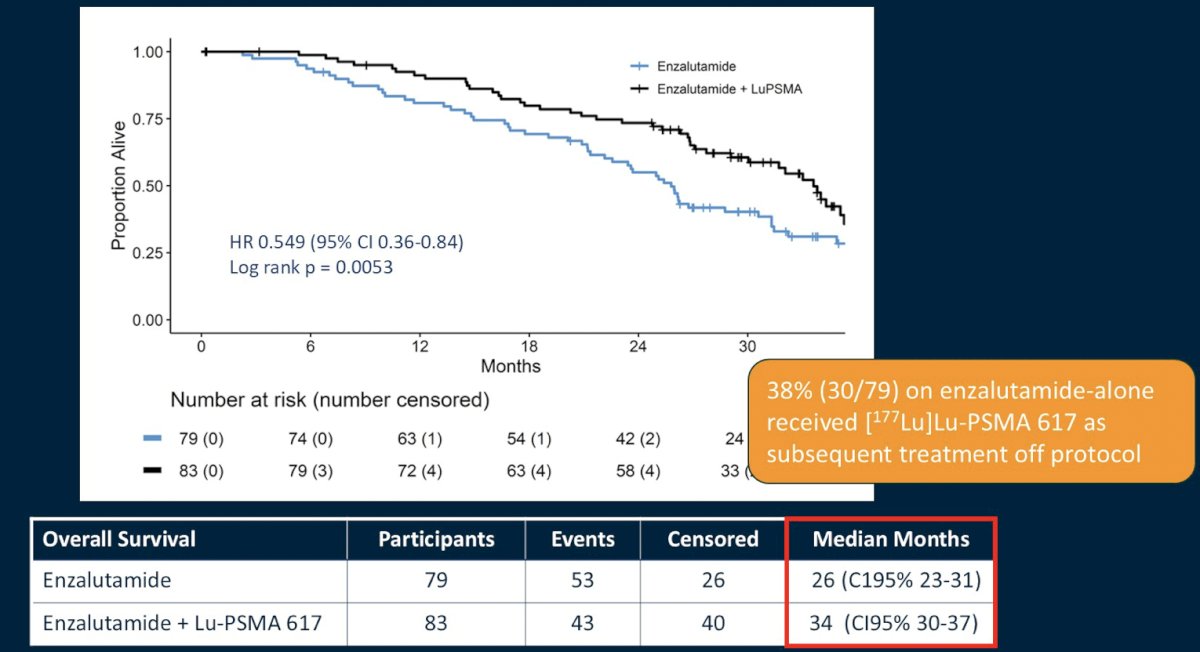
To summarize, Dr. Fendler emphasized that LuPSMA radioligand therapy is approved and reimbursed for prostate cancer therapy based on VISION in the third line mCRPC setting after an androgen receptor pathway inhibitor and chemotherapy. Moreover, there is phase III evidence for second line mCRPC looking at LuPSMA versus an androgen receptor pathway inhibitor switch based on PSMAfore and SPLASH. There is also phase II (randomized) evidence for first line mCRPC LuPSMA + enzalutamide versus enzalutamide from the ENZA-p trial, as well as LuPSMA + docetaxel versus docetaxel in the upfrontPSMA trial. mCRPC after triplet therapy was allowable in the VISION trial, however no subgroup evidence has been published.
Dr. Fendler concluded his presentation discussing when we should be using LuPSMA by noting that there is robust first line and second line mCRPC data for LuPSMA.
Presented by: Wolfgang Fendler, MD, University Hospital Essen, Essen, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:
- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021 Feb 27;397(10276):797-804.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.
- Emmett L, Subramaniam S, Crumbaker M, et al. Overall survival and quality of life with [177Lu]Lu-PSMA-617 plus enzalutamide versus enzalutamide alone in metastatic castration-resistant prostate cancer (ENZA-p): Secondary outcomes from a multicentre, open-label, randomized, phase 2 trial. Lancet Oncol. 2025 Feb 12 [online ahead of print].