(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain was host to a thematic session on clinically relevant questions in the management of advanced, hormone-sensitive prostate cancer. Dr. Valerie Fonteyne discussed the role of radiotherapy for high-risk, biochemically recurrent prostate cancer patients with a positive PSMA PET scan.
The session started with a case presentation of a 71-year-old patient with significant co-morbidities who underwent a radical prostatectomy for Grade Group 5 pT2N0R0 prostate cancer. He subsequently developed biochemical failure with a PSA increase to 1.02 ng/ml one year post-operatively. Conventional imaging staging scans were negative
Dr. Fonteyne noted that this patient meets the eligibility criteria for EMBARK, with a PSA >1 ng/ml and a PSA doubling time (PSADT) of ≤9 months.1 He also meets the EAU high-risk biochemical recurrence criteria, given his PSADT of <1 year and Grade Group 5 disease:
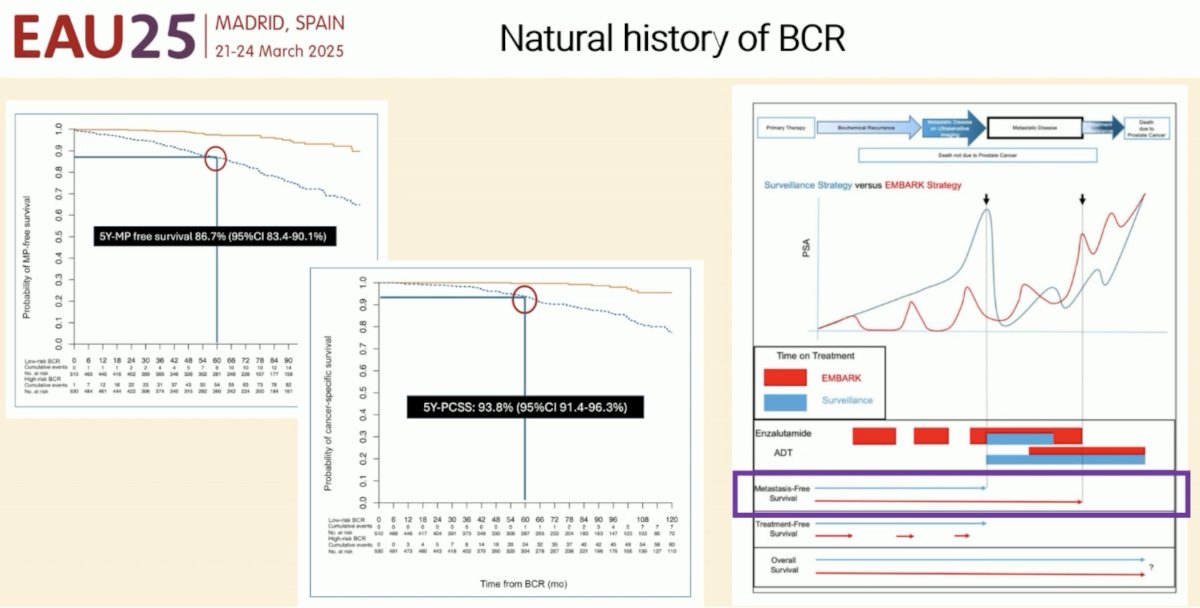
But does this patient, and all such patients meeting these criteria, really need intensified systemic therapy with enzalutamide +/- ADT, per the results of the EMBARK trial? Dr. Fonteyne remarked that the majority of these patients actually do quite well without intensified systemic therapy. Highlighting data from a retrospective series by Tilki et al from 2019, she noted that the 5-year metastasis-free survival of these patients is 87%, and the corresponding 5-year prostate cancer-specific survival is 94%.2
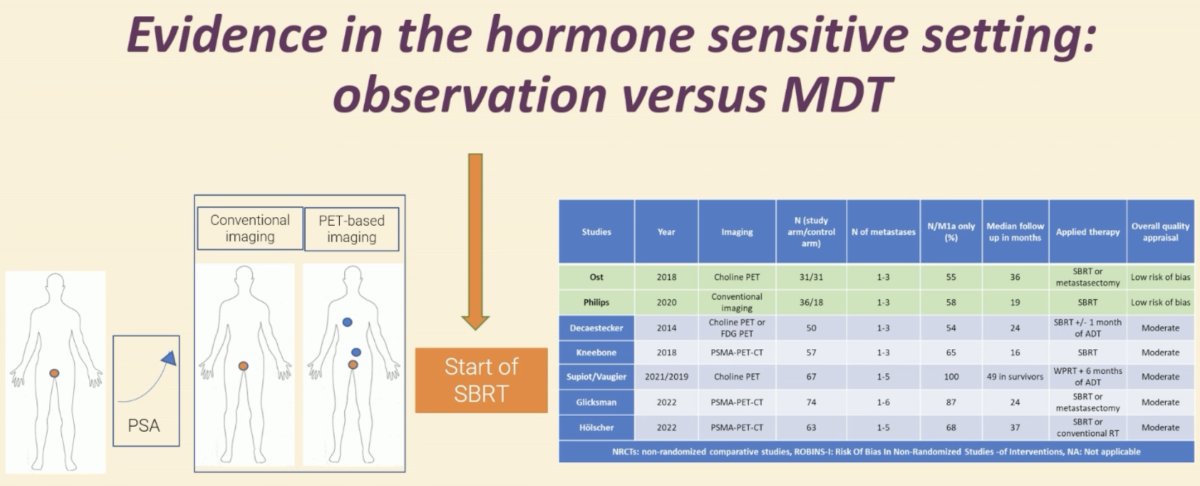
Can we use alternative strategies in this setting? One such option is metastasis-directed therapy using stereotactic body radiotherapy (SBRT) in select patients with oligometastatic disease.
The STOMP trial was a multicenter, randomized phase II trial that prospectively evaluated the effects of MDT for patients with evidence of oligometastatic disease on choline PET/CT (up to three extracranial sites) who had received prior treatment with curative intent and had evidence of biochemical recurrence with testosterone >50 ng/ml (i.e. metachronous, oligometastatic mCSPC). Between 2012 and 2015, 62 patients were randomized 1:1 and MDT was either SBRT or metastasectomy. With a median follow up of 5.3 years, the five-year ADT-free survival was 8% in the surveillance arm compared to 34% for the MDT group (HR: 0.57, 95% CI: 0.38-0.84, log-rank p=0.06). The secondary endpoint of CRPC-free survival at 5 years was 53% in subjects under surveillance and 76% in those receiving MDT (HR: 0.62, 80% CI: 0.35-1.09.3
The ORIOLE trial was a randomized phase II trial of 54 men with metachronous, oligometastatic mCSPC (up to three sites). Metastatic sites were diagnosed via conventional imaging (CT, MRI, and/or radionuclide bone scan). Between 2016 and 2018, patients were randomized in a 2:1 fashion to receive SABR or observation. The primary outcome was progression at 6 months, defined as serum PSA increase, progression detected by conventional imaging, symptomatic progression, ADT initiation for any reason, or death. Progression at six months occurred in 7 of 36 patients (19%) receiving SABR and 11 of 18 patients (61%) undergoing observation (p=0.005). Treatment with SABR improved median PFS (not reached versus 5.8 months; HR: 0.30; 95% CI: 0.11 – 0.81; p=0.002). No grade ≥3 toxic effects were observed.4
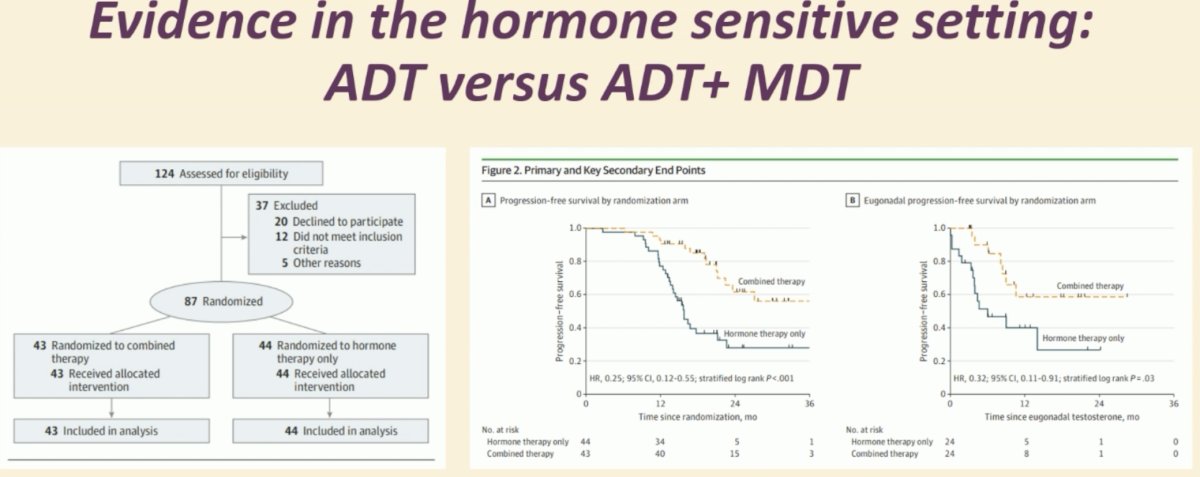
While MDT with SBRT can be used to delay time to ADT initiation, MDT can also be combined with ADT in the hormone-sensitive setting to improve survival outcomes. EXTEND was a phase II trial of prostate cancer patients with ≤5 metastatic sites of disease who were randomized to MDT + 6 months of hormone therapy versus 6 months of hormone therapy alone. After 6 months, patients were given a hormone therapy break, after which hormone therapy was resumed for evidence of biochemical and/or radiographic progression.
The addition of MDT improved progression-free survival, with median PFS not reached in the MDT + ADT arm versus 16 months in the ADT alone arm (HR: 0.29, p<0.001). Eugonodal progression-free survival, defined as time from the demonstration of eugonadal testosterone levels (>150 ng/dL) to progression, was also significantly prolonged in the MDT + ADT arm (p=0.025).5
At GU ASCO 2025, Dr. Chad Tang presented WOLVERINE, an analysis from the X-MET collaboration leveraging individual patient data from randomized trials of MDT in oligometastatic prostate cancer. This collaboration includes 5 trials of 472 oligometastatic prostate cancer patients followed for a median of 41 months. These patients were randomized 1:1 to MDT + standard of care (n=248) or standard of care alone (n=224). The addition of MDT was associated with improved:
- PFS: HR 0.44, 95%, p<0.001
- rPFS: HR 0.59, p<0.001
- Freedom from castration-resistance: HR 0.58, p=0.02
- Overall survival: HR 0.64, p=0.057

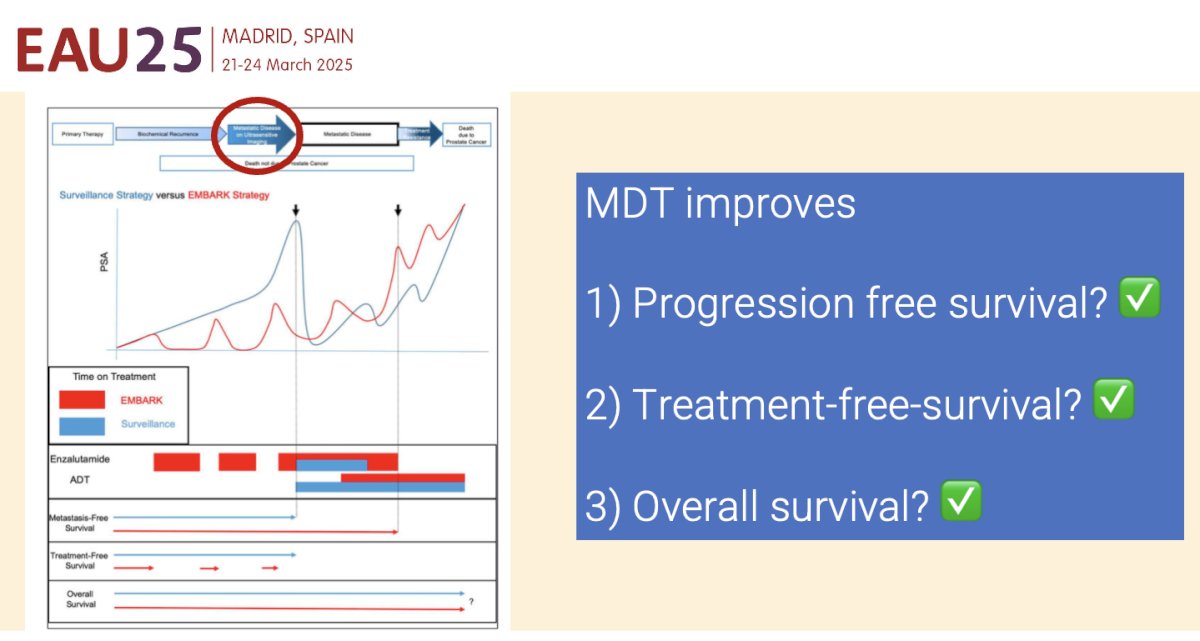
Based on these results, Dr. Fonteyne concluded that MDT improves:
- Progression-free survival
- Treatment-free survival
- Overall survival
Presented by: Valerie Fonteyne, MD, PhD, Associate Professor, Radiation Oncology, University of Ghent, East Flanders, Belgium
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:
- Freedland SJ, de Almeida Luz M, De Giorgi U, et al. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med. 2023; 389(16): 1453-65.
- Tilki D, Preisser F, Graefen M, Huland H, Pompe RS. External Validation of the European Association of Urology Biochemical Recurrence Risk Groups to Predict Metastasis and Mortality After Radical Prostatectomy in a European Cohort. Eur Urol. 2019; 75(6): 896-900.
- Ost P, Reynders D, Decaestecker K, et al. Surveillance of metastasis-directed therapy for oligometastatic cancer recurrence: A prospective, randomized, multicenter phase II trial. J Clin Oncol. 201; 36(5):446-453.
- Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol. 2020; 6(5) :650-659.
- Tang C, Sherry AD, Haymaker C, et al. Addition of Metastasis-Directed Therapy to Intermittent Hormone Therapy for Oligometastatic Prostate Cancer: The EXTEND Phase 2 Randomized Clinical Trial. JAMA Oncol. 2023; 9(6): 825-34.