(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025, was host to the session Progress and Controversies in Oncological Urology from the EAU Section of Oncological Urology. Dr. Alberto Bossi debated why total eradication is the way to go for de novo low-volume metastatic hormone-sensitive prostate cancer.
Dr. Bossi began his presentation by stating that when considering the contemporary management of low-volume metastatic hormone-sensitive prostate cancer, he always thinks of two key aspects: (i) the role of intensified local treatment and (ii) the role of metastasis-directed therapy. Both of these questions are particularly relevant in 2025, as the field is transitioning from an era of intensified systemic treatment to an era focused on total eradication.
The only study published so far in this disease space is the PEACE-1 trial, which included patients with de novo metastatic castration-sensitive prostate cancer. Eligible patients had distant metastatic disease, defined as at least one lesion on a bone scan and/or CT scan. Participants were randomized in a 1:1:1:1 fashion to receive standard-of-care androgen deprivation therapy plus docetaxel, with or without the addition of abiraterone or radiotherapy. The study design is illustrated below.1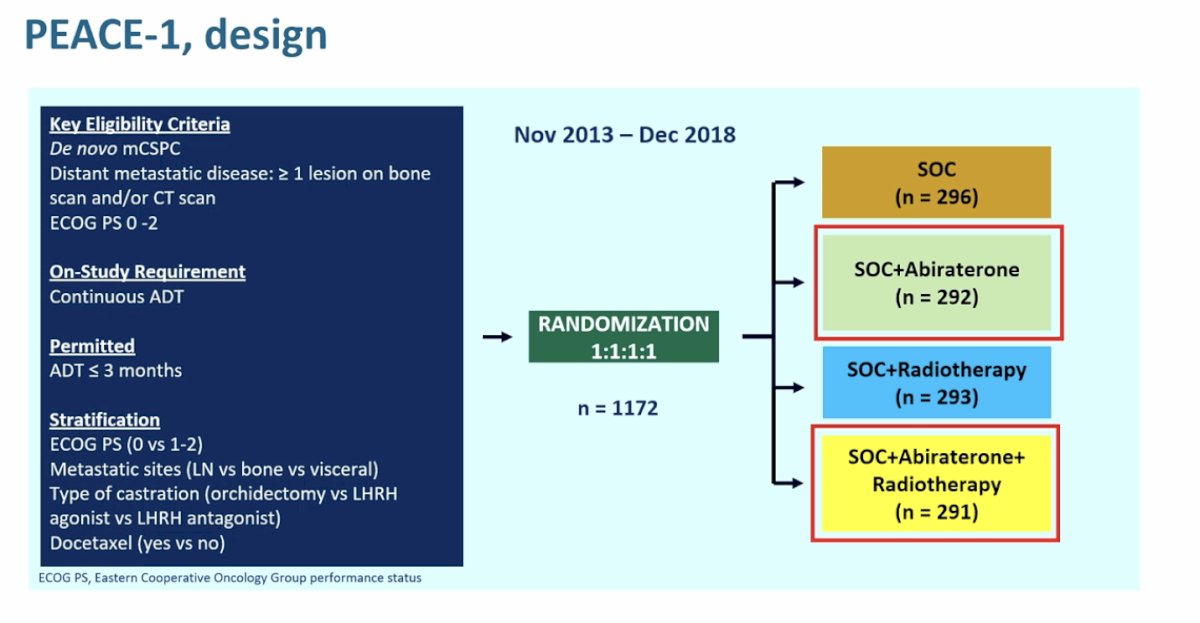
In terms of radiologic progression-free survival, achieving the highest survival curve requires radiotherapy, regardless of whether intensified systemic treatment is used. This significant impact remains evident when comparing standard of care plus abiraterone versus standard of care plus abiraterone and radiotherapy.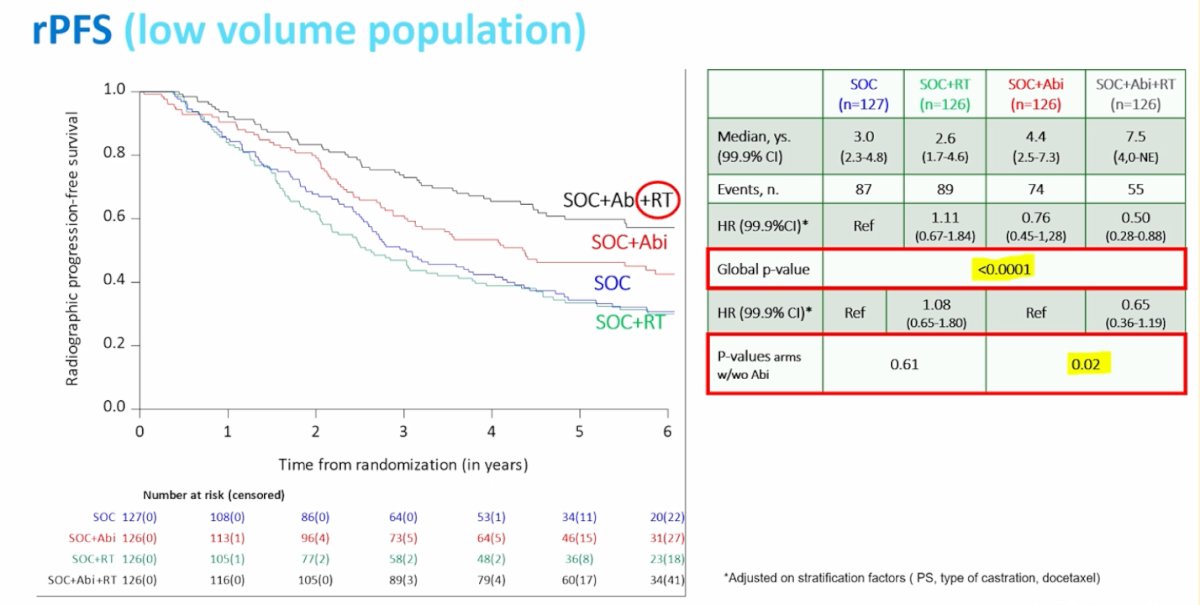
Notably, the PEACE-1 data show no significant impact on overall survival. However, when examining the survival curves, the highest-performing curve belongs to patients treated with intensified systemic therapy and radiotherapy. This is the only population that has not yet reached the median overall survival.1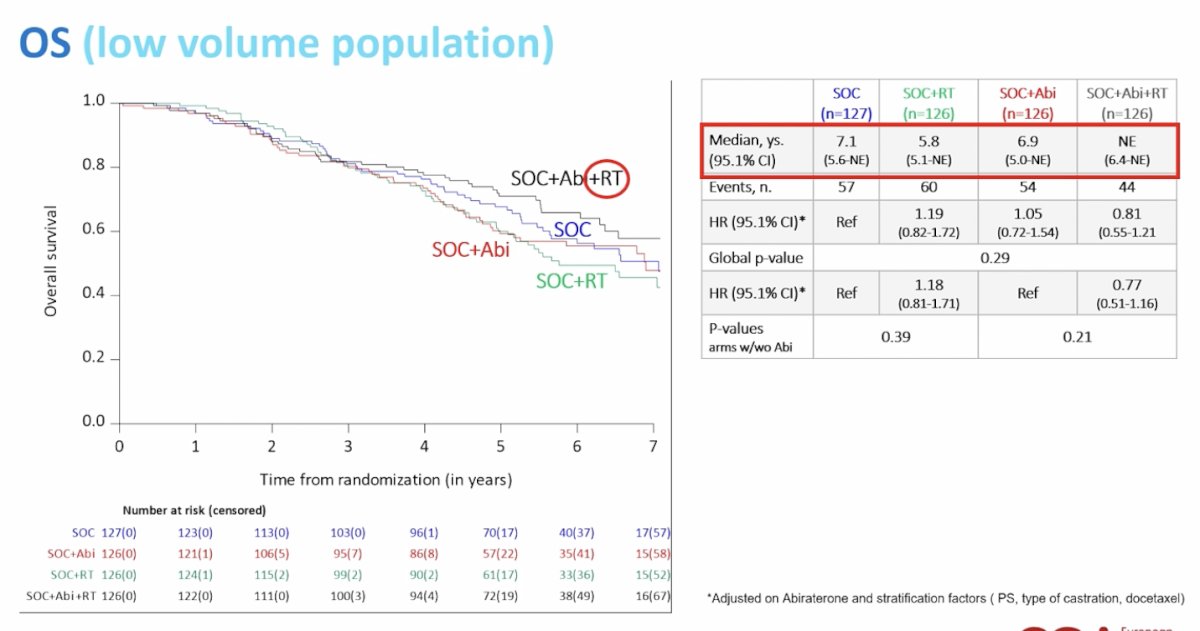
Moreover, another important endpoint was the time to serious genitourinary events, which showed a significant benefit in both the low-volume and overall populations, as illustrated in the curves below.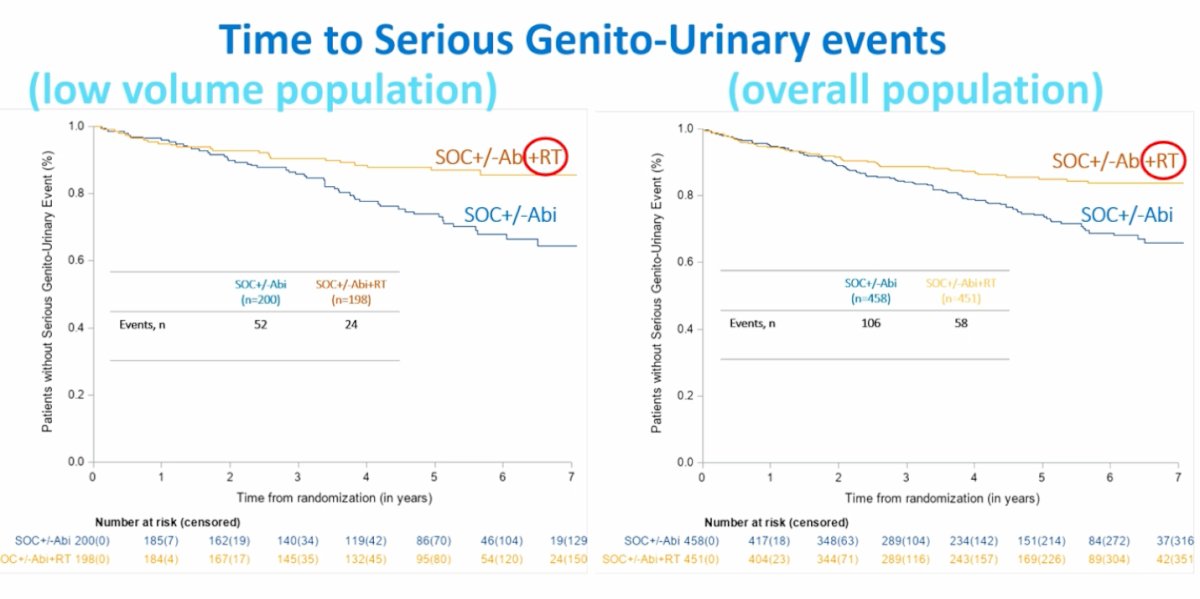
PEACE-1 was not the only study to demonstrate this; the STAMPEDE study also showed that radiotherapy to the primary tumor was associated with a significant (p=0.017) reduction in the risk of upper urinary tract obstruction.2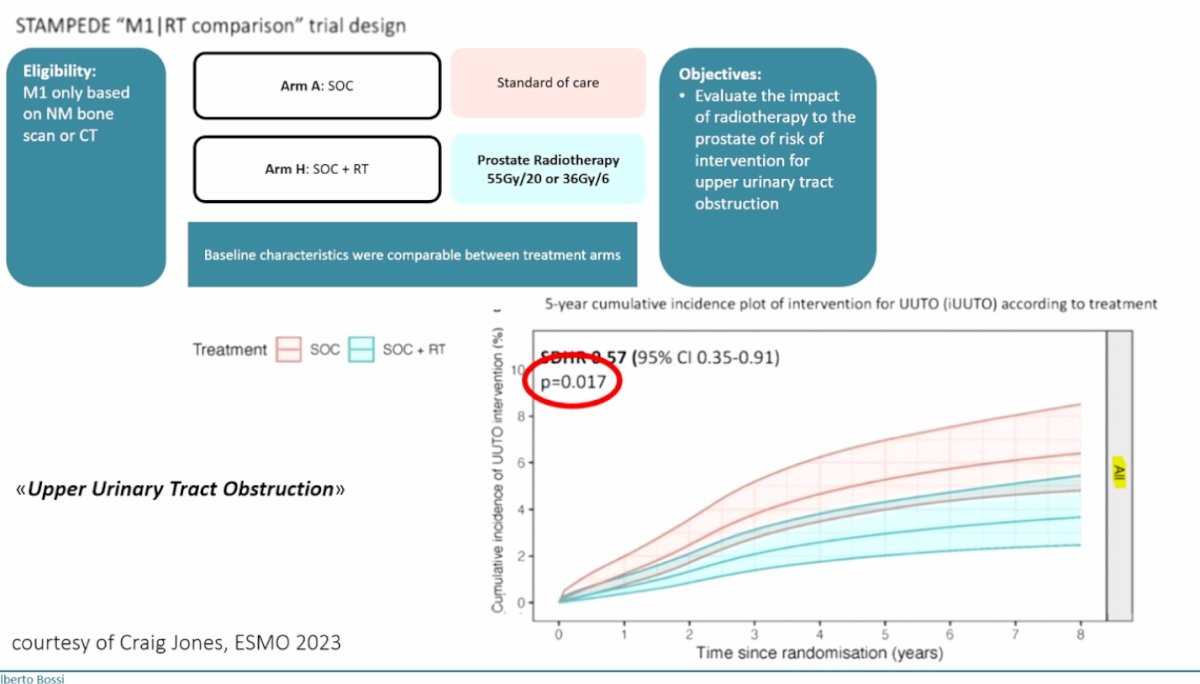
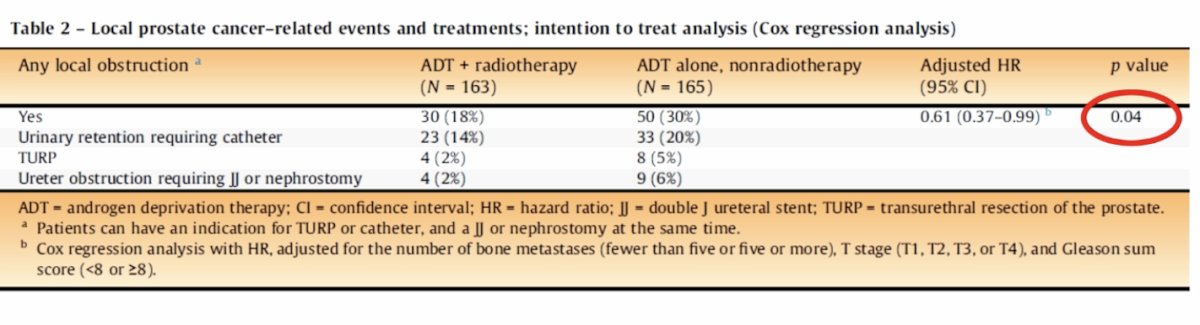
More recently, the HORRAD group also confirmed a significant impact of radiotherapy in reducing urinary obstruction events requiring intervention, including urinary catheter placement, transurethral resection of the prostate (TURP), and ureteral obstruction requiring urinary diversion.3
Furthermore, another important outcome is that radiotherapy to the primary tumor also delays the development of castration-resistant disease in both the overall and low-volume populations as shown in the curves below.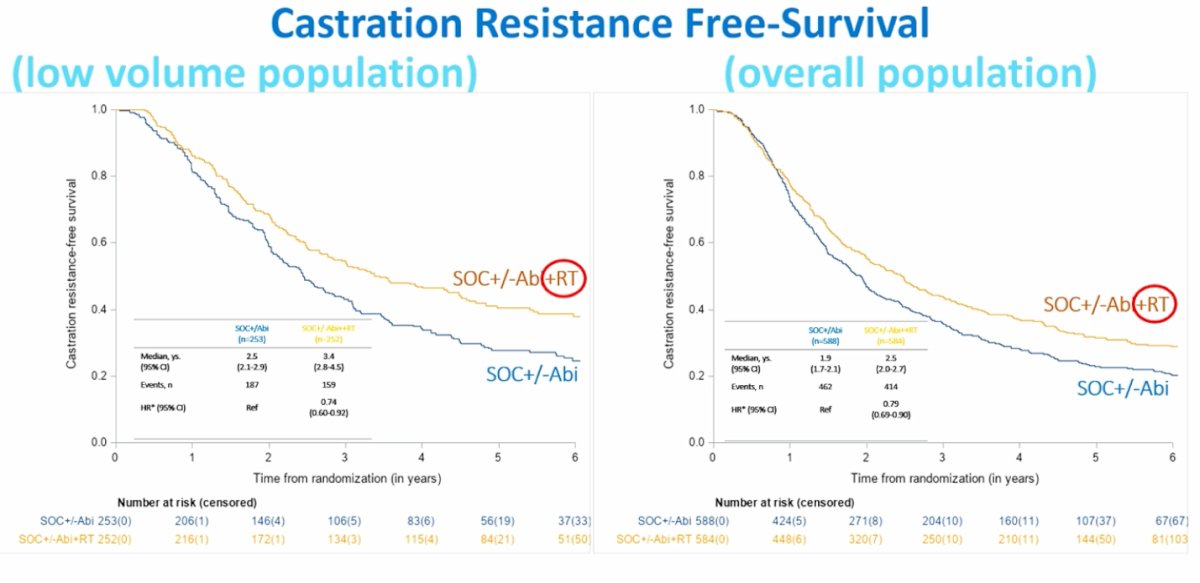
Based on this data, the European Association of Urology guidelines recommend radiotherapy for patients with metastatic hormone-sensitive prostate cancer who have low-volume disease and strongly advise against offering radical prostatectomy outside of a clinical trial setting.
Regarding metastasis-directed therapy, Dr. Bossi highlighted the conflicting evidence on whether it should be offered to patients with oligometastatic disease (1-5 metastases). He pointed to the table below, in which Dr. James emphasized that metastasis-directed therapy remains under evaluation in both synchronous and metachronous settings. Currently, there are no solid randomized data demonstrating that metastasis-directed therapy in this context alters the natural history of the disease.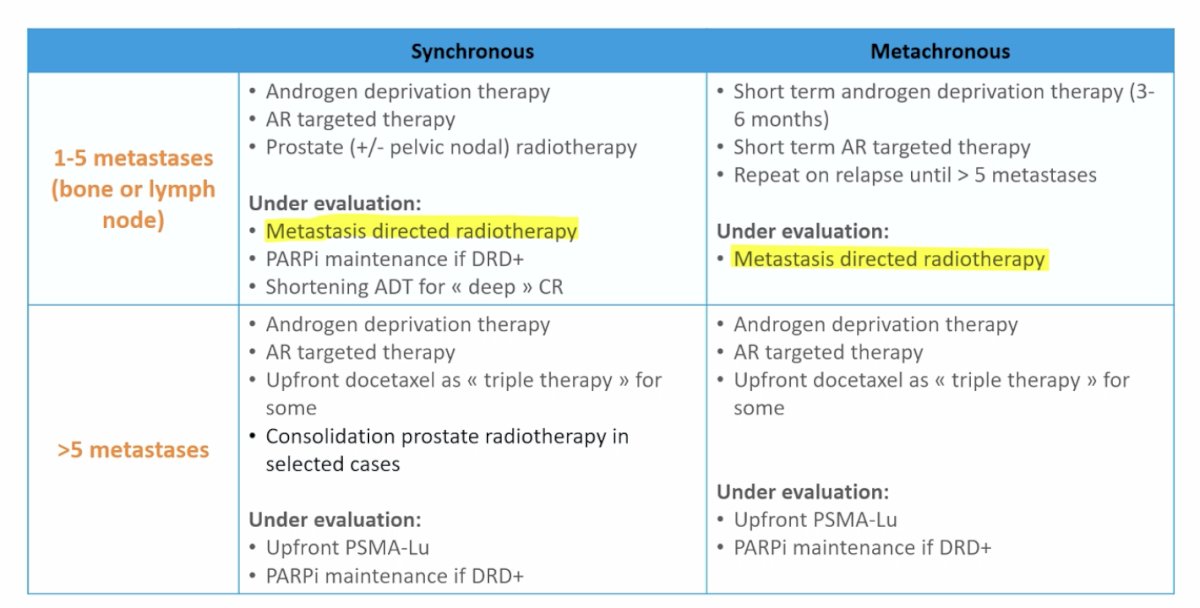
The WOLVERINE meta-analysis, presented at ASCO GU this year, included five randomized controlled trials comparing standard-of-care treatment with or without metastasis-directed therapy. The analysis found similar proportions of patients with synchronous and metachronous disease in both treatment arms.
This data must be interpreted within its limitations, but it still demonstrates a significant improvement in progression-free survival in patients treated with metastasis-directed therapy, both at the trial level analysis and in the Cox regression analysis stratified by trial. However, there is currently no demonstrated impact on overall survival. Dr. Bossi emphasized that overall survival should not be the sole outcome of interest, as there are many other clinically meaningful endpoints to consider.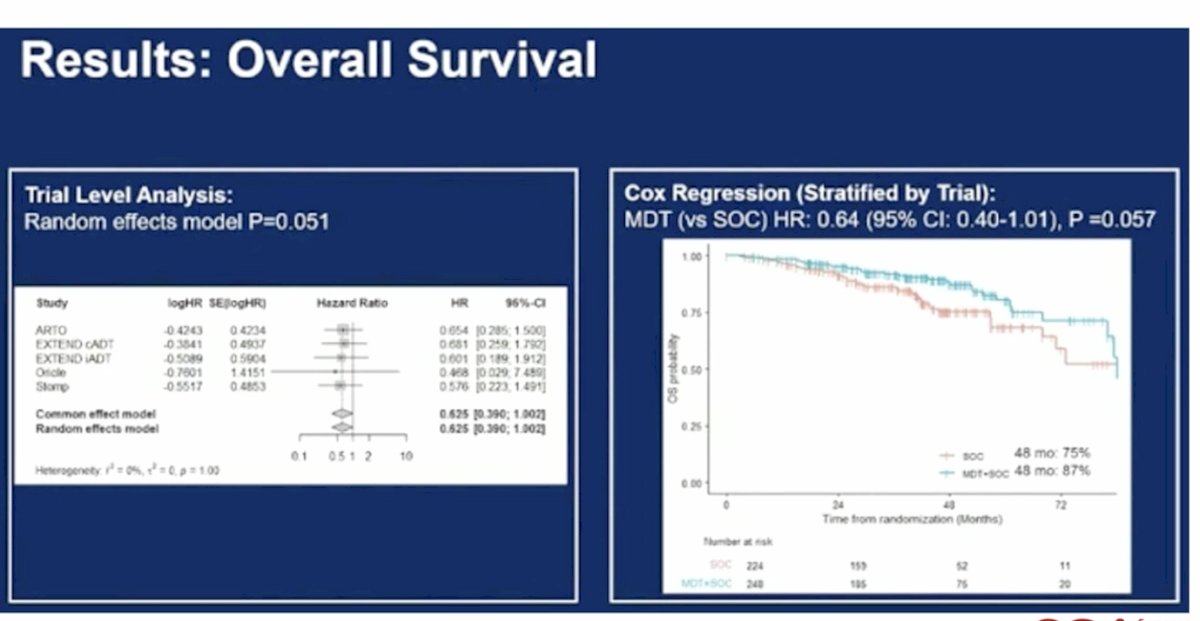
Dr. Bossi concluded his presentation by highlighting the ongoing randomized trials in this space, which are summarized in the table below. These trials aim to further clarify the role of metastasis-directed therapy and intensified treatment approaches in metastatic hormone-sensitive prostate cancer.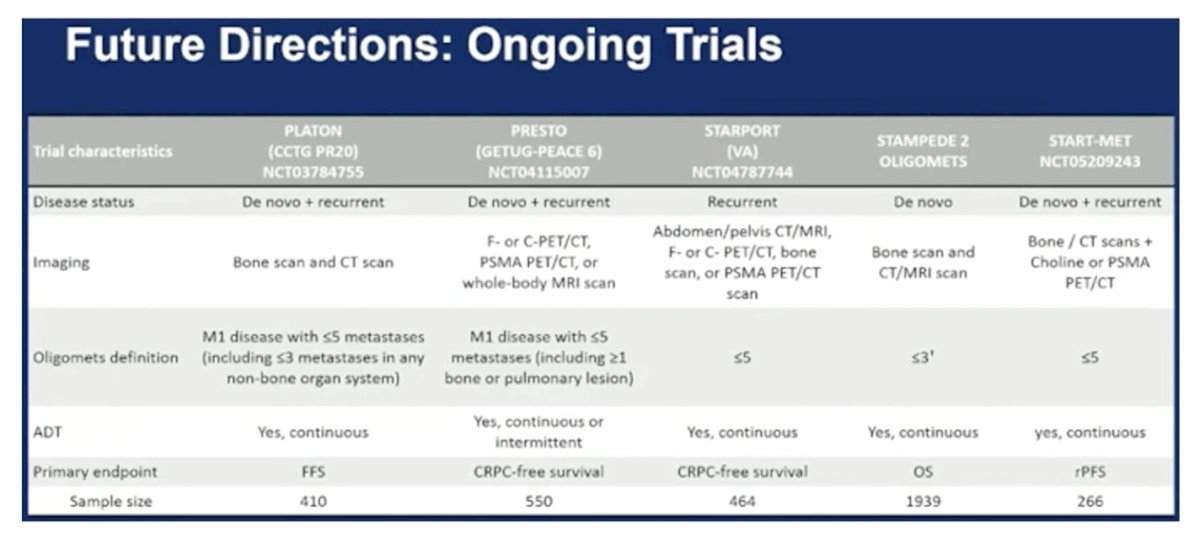
Presented by: Alberto Bossi, MD, Head of the Urology and Prostate Brachytherapy Unit at the Gustave Roussy Cancer Institute in Villejuif, France
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:- Bossi A, Foulon S, Maldonado X, Sargos P, MacDermott R, Kelly P, Fléchon A, Tombal B, Supiot S, Berthold D, Ronchin P, Kacso G, Salem N, Calabro F, Berdah JF, Hasbini A, Silva M, Boustani J, Ribault H, Fizazi K; PEACE-1 investigators. Efficacy and safety of prostate radiotherapy in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2024 Nov 23;404(10467):2065-2076. doi: 10.1016/S0140-6736(24)01865-8. PMID: 39580202.
- Parker CC, James ND, Brawley CD, Clarke NW, Ali A, Amos CL, Attard G, Chowdhury S, Cook A, Cross W, Dearnaley DP, Douis H, Gilbert DC, Gilson C, Gillessen S, Hoyle A, Jones RJ, Langley RE, Malik ZI, Mason MD, Matheson D, Millman R, Rauchenberger M, Rush H, Russell JM, Sweeney H, Bahl A, Birtle A, Capaldi L, Din O, Ford D, Gale J, Henry A, Hoskin P, Kagzi M, Lydon A, O'Sullivan JM, Paisey SA, Parikh O, Pudney D, Ramani V, Robson P, Srihari NN, Tanguay J, Parmar MKB, Sydes MR; STAMPEDE Trial Collaborative Group. Radiotherapy to the prostate for men with metastatic prostate cancer in the UK and Switzerland: Long-term results from the STAMPEDE randomised controlled trial. PLoS Med. 2022 Jun 7;19(6):e1003998. doi: 10.1371/journal.pmed.1003998. PMID: 35671327; PMCID: PMC9173627.
- Boevé LMS, Hulshof MCCM, Vis AN, Zwinderman AH, Twisk JWR, Witjes WPJ, Delaere KPJ, Moorselaar RJAV, Verhagen PCMS, van Andel G. Effect on Survival of Androgen Deprivation Therapy Alone Compared to Androgen Deprivation Therapy Combined with Concurrent Radiation Therapy to the Prostate in Patients with Primary Bone Metastatic Prostate Cancer in a Prospective Randomised Clinical Trial: Data from the HORRAD Trial. Eur Urol. 2019 Mar;75(3):410-418. doi: 10.1016/j.eururo.2018.09.008. Epub 2018 Sep 25. PMID: 30266309.