(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025, was host to the session Progress and Controversies in Oncological Urology from the EAU Section of Oncological Urology. Dr. Bertrand Tombal delved into how to optimize outcomes in men with biochemical recurrence after local treatment with curative intent.
Dr. Tombal began his presentation by emphasizing that not all biochemical recurrences (BCR) are the same—some are high-risk "tigers" disguised as low-risk "kittens." He underscored the importance of using the EAU BCR risk classification to stratify patients into low- or high-risk BCR groups.
EAU Low-risk BCREAU low-risk BCR includes patients with a PSA doubling time (PSA-DT) >1 year and post-prostatectomy ISUP grade group <4 and an interval to biochemical failure >18 months. For patients with prior radiotherapy (RT), low-risk BCR includes those with an ISUP grade group <4 on biopsy.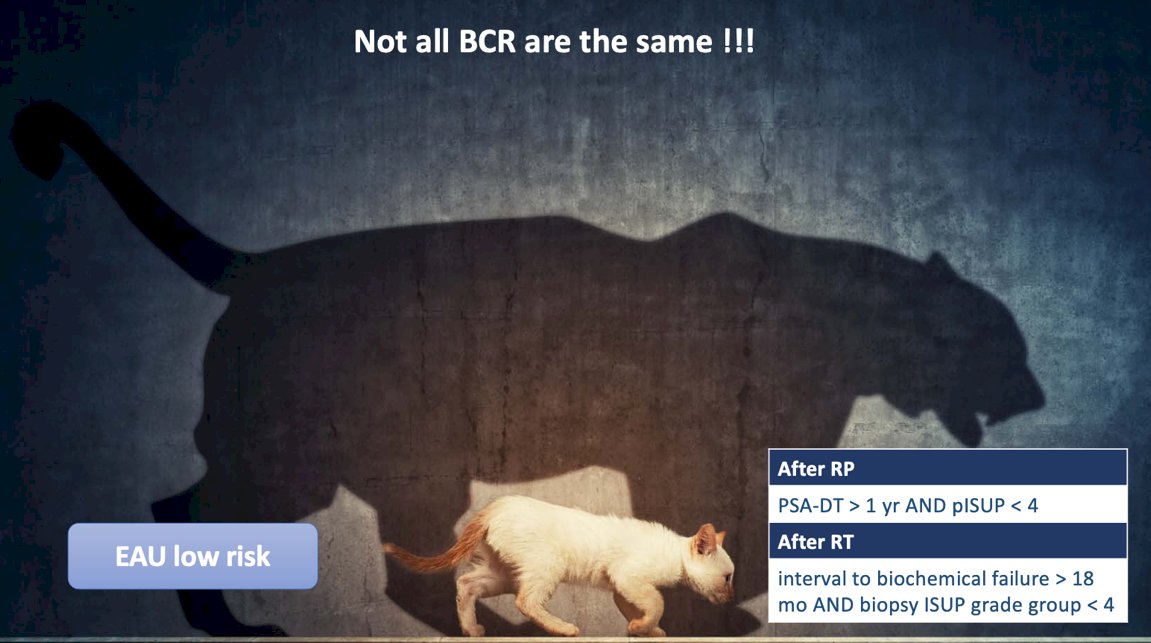
The risk of prostate cancer-specific mortality following biochemical recurrence (BCR) after radical prostatectomy (RP) was evaluated in a cohort of 5,096 patients who underwent RP at Johns Hopkins, US. Among them, 979 (19%) experienced BCR. With a median follow-up of 10.3 years after surgery and 6.8 years following PSA failure, the study identified PSA doubling time (PSA-DT) as a strong prognostic marker. Notably, when PSA-DT was less than 9 months, the hazard ratio (HR) for prostate cancer-specific mortality was as high as 27.4 (95% CI: 10.66–70.85).1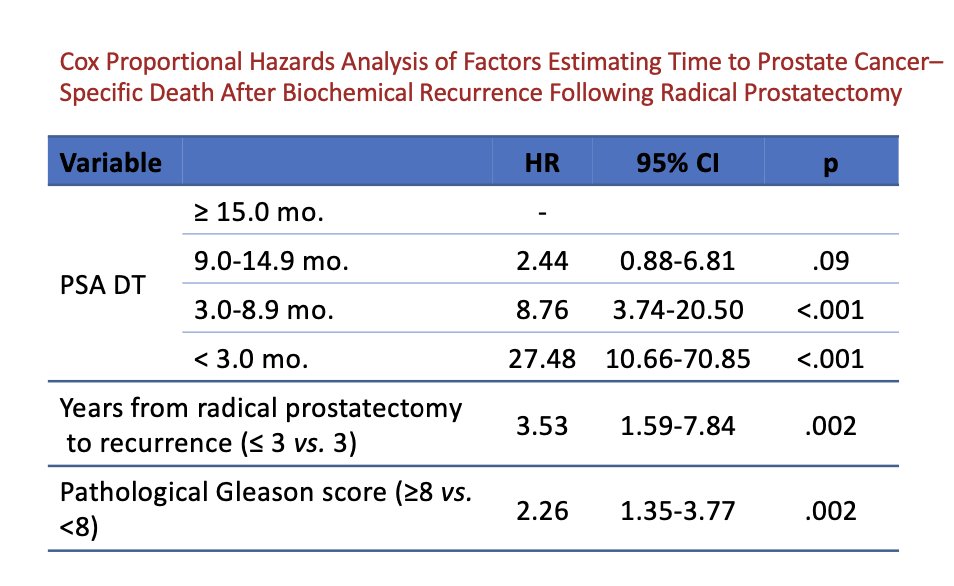
Dr. Tombal discussed the case of a 61-year-old patient with intermediate-risk localized prostate cancer (PSA 7 ng/mL, T1c, 3/12 biopsy cores Gleason 7 [4+3]). The patient underwent radical prostatectomy (RP) with limited lymph node dissection (LND). Surgical pathology revealed pT2b disease, Gleason 7 (4+3), R0 resection, N0 (with 8 lymph nodes examined), and M0 status. Over time, the patient experienced a slowly rising PSA, reaching 0.4 ng/mL. Based on risk stratification, the patient’s estimated prostate cancer-specific survival at 15 years is 94%, as shown in the table below.1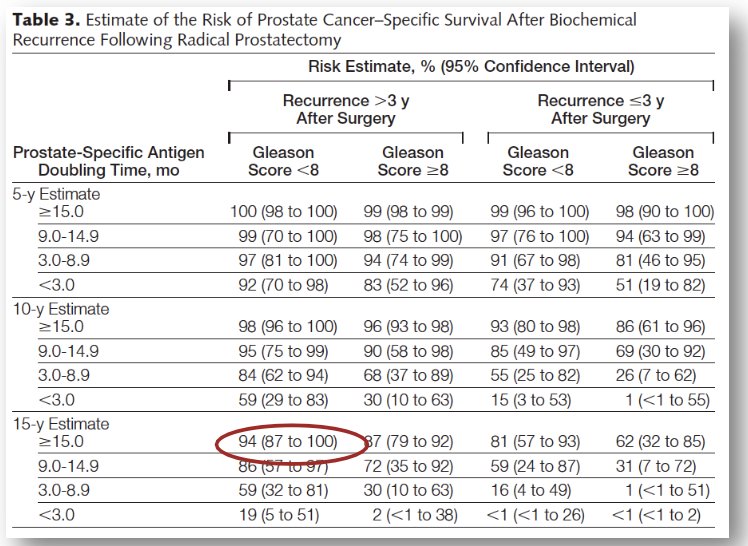
The EAU guidelines recommend offering early salvage radiotherapy (SRT) as a second-line treatment option for men experiencing biochemical recurrence (BCR) after RP.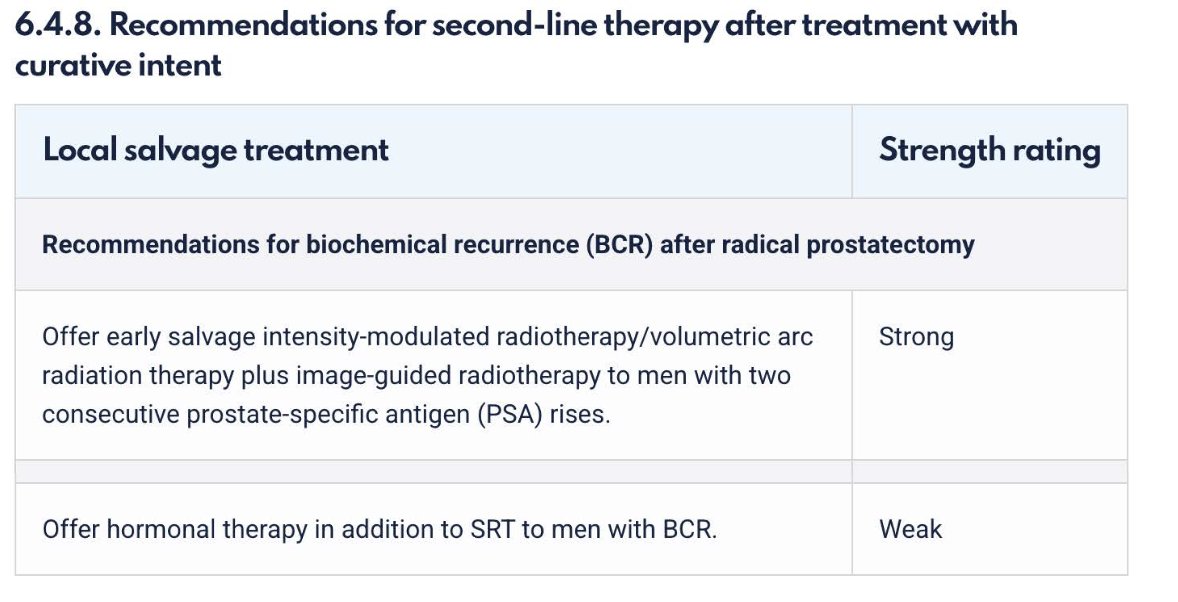
The conundrum of salvage radiotherapy (sRT)
No adequately designed randomized controlled trial (RCT) has demonstrated that sRT (early or late) improves oncological outcomes (PFS, MFS, or OS) compared to surveillance. However, three RCTs have shown that adjuvant radiotherapy vs. surveillance delays PSA progression, with one trial demonstrating a 10% improvement in metastasis free survival (MFS) at 10 years (61% vs. 71%) and an 8% improvement in OS at 10 years (66% vs. 74%). Additionally, three RCTs have established that early sRT is equivalent to adjuvant radiotherapy in terms of event-free survival. The status of salvage radiotherapy as the "standard of care" is primarily based on ambispective series showing that selected patients may experience prolonged PSA responses.
Dr. Tombal emphasized the importance of early salvage radiotherapy, noting that if administered too late, it is likely ineffective. Data from the study below demonstrate a proportional decrease in progression-free survival as PSA levels increase.2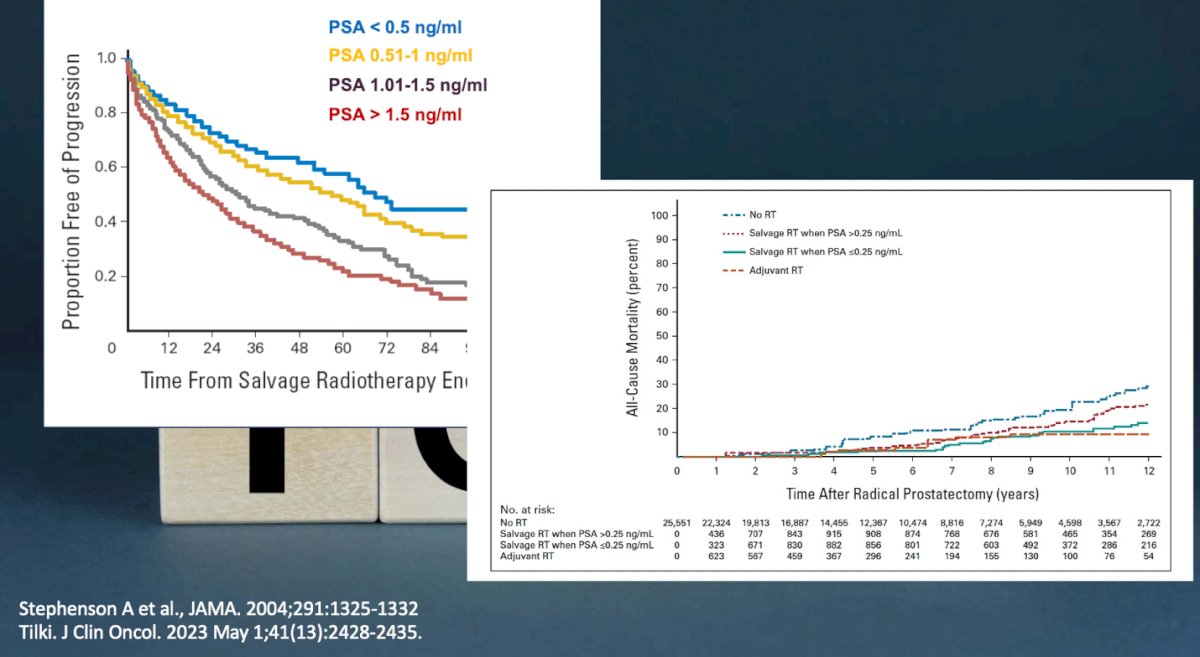
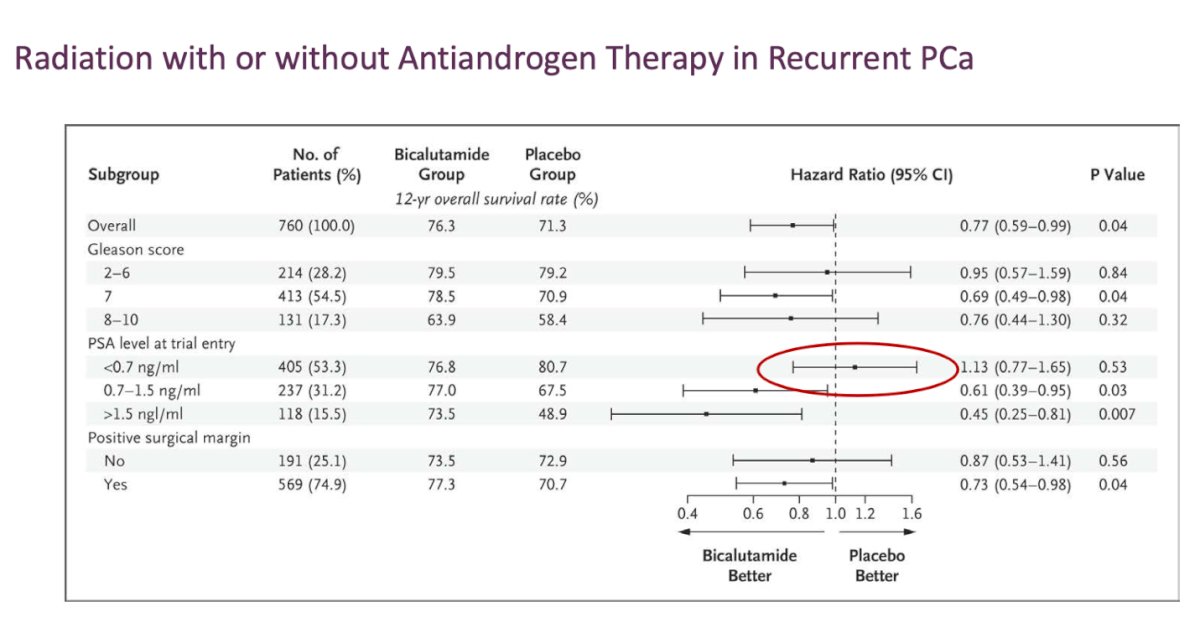
Dr. Tombal further advised against the routine use of hormone therapy solely for reassurance when administering early salvage radiotherapy. Data from a study comparing bicalutamide versus placebo showed no clear benefit of adding bicalutamide in patients with a PSA level <0.7 ng/mL, as illustrated in the forest plot below.3
Additionally, data from RADICALS-HD demonstrated no significant difference in metastasis-free survival (MFS) between long-term and short-term ADT, with similar outcomes observed in both groups.4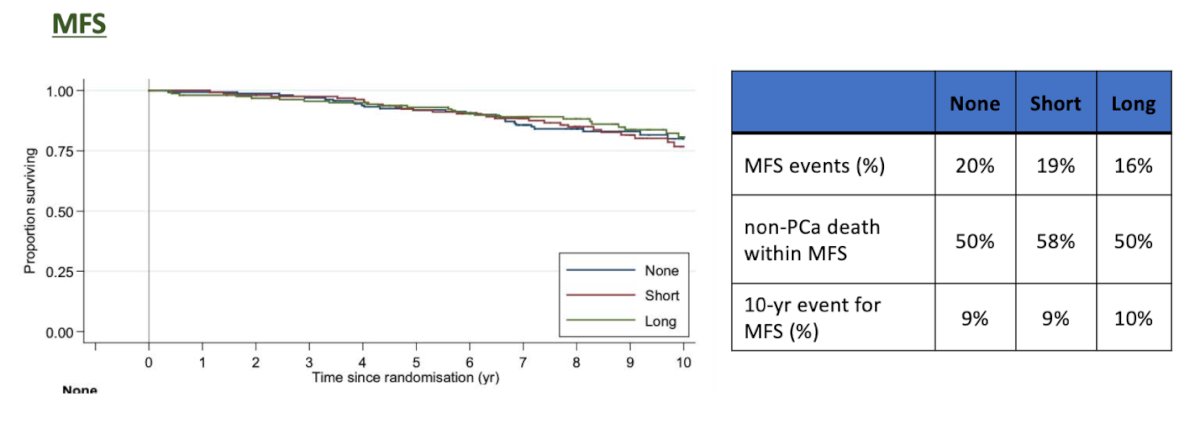
Dr. Tombal highlighted that if we can accurately identify patients at higher risk, they may benefit from the addition of ADT to sRT. He presented a study validating the 22-gene genomic classifier (Decipher) in 352 men with recurrent prostate cancer who were randomized to bicalutamide or placebo. Notably, patients with low GC scores did not derive a significant benefit from adding ADT to their sRT treatment.5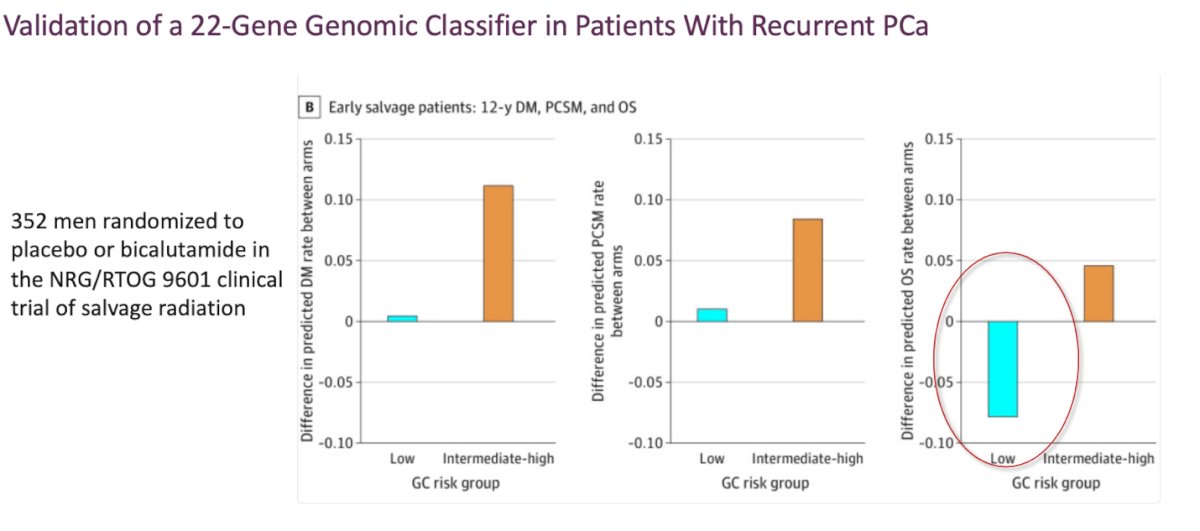
Moreover, AI may help in risk-stratifying patients who may benefit from ADT when receiving sRT. At AUA 2024, Todd Morgan presented data from 1,855 patients enrolled in the NRG 9601 and 0534 trials. The analysis incorporated clinical and histopathological data, utilizing an MMAI-derived digital pathology-based biomarker (Artera AI) to stratify patients into lower-risk and higher-risk groups. Notably, only patients classified as high-risk by MMAI demonstrated a significant benefit from the addition of ADT, as illustrated below.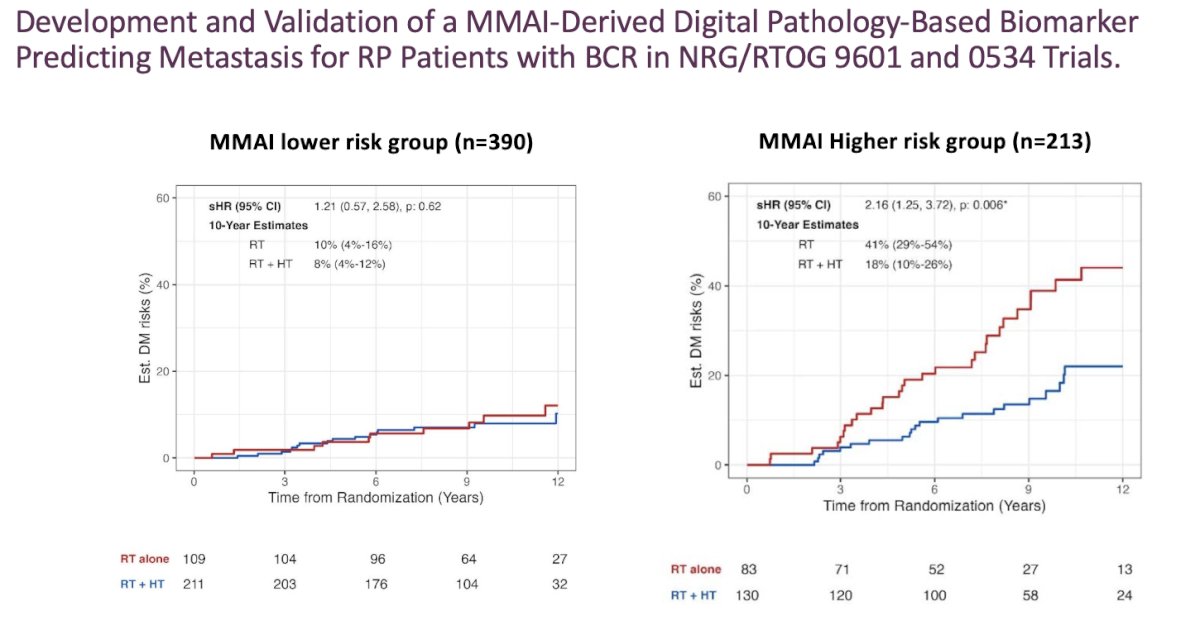
EAU High-risk BCR
According to the EAU BCR risk classification, high-risk biochemical recurrence (BCR) includes patients with a PSA doubling time (PSA-DT) ≤1 year or pISUP grade 4-5 after radical prostatectomy (RP) and an interval to biochemical failure ≤18 months, or those with a biopsy ISUP grade group ≥4 after radiotherapy (RT).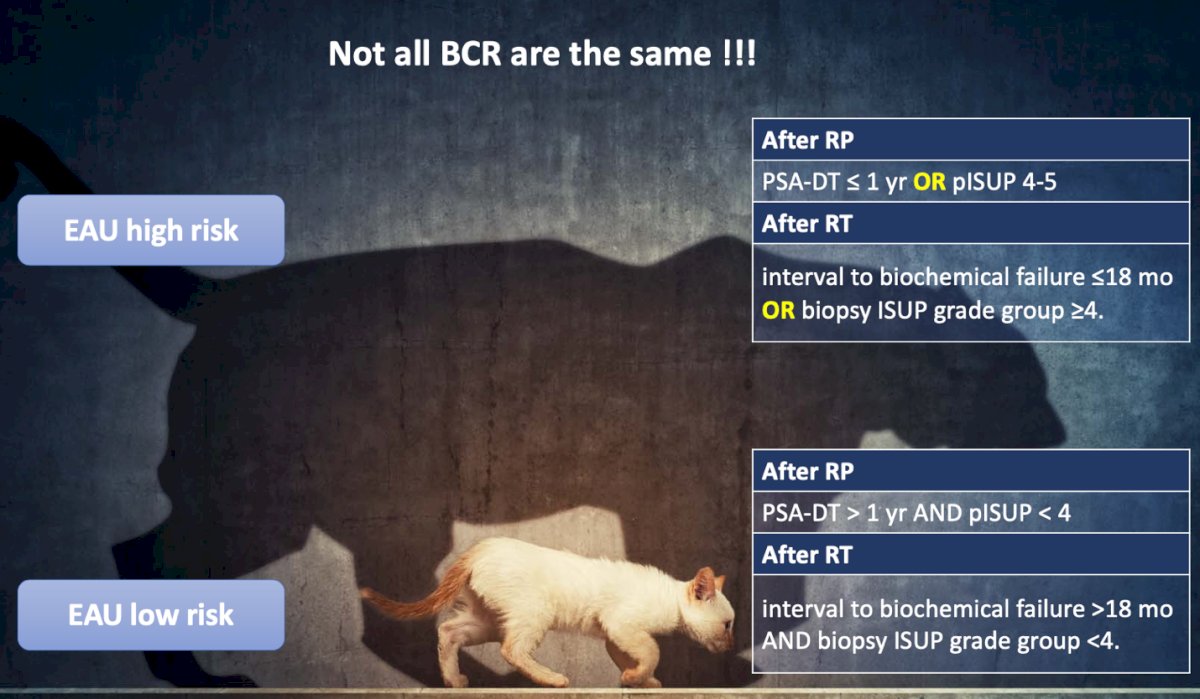
When patients are classified as high-risk according to the EAU BCR criteria, an effective systemic treatment is needed, as salvage radiotherapy (sRT) alone may be insufficient. Dr. Tombal emphasized that for these patients, sRT might be administered too late to be effective. He presented data from the ICECaP database, showing that EAU high-risk patients have poor PSA progression outcomes when treated with sRT alone, as illustrated below.6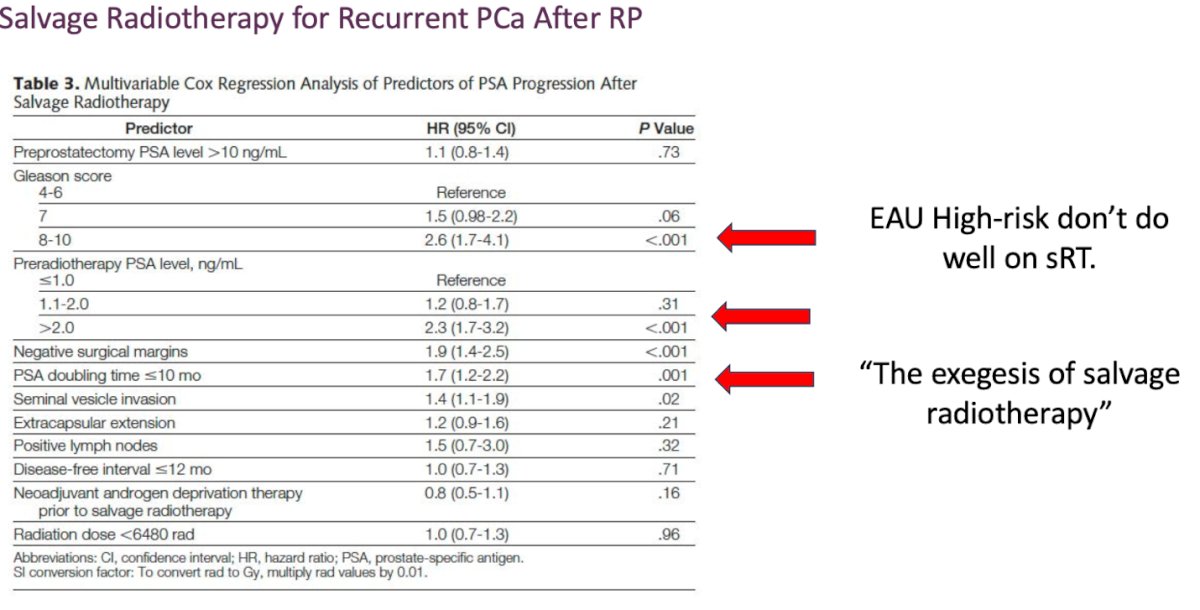
Moreover, prognostic factors in the post-prostatectomy salvage radiotherapy (sRT) setting, with and without hormone therapy, were analyzed in an individual patient data (IPD) study using the ICECaP database. This analysis included 647 subjects from GETUG-AFU-16, NRG/RTOG-9601, and a subset of EORTC-22911. Among the factors assessed, pathological Gleason score and PSA level at the time of sRT were identified as the strongest predictors of survival outcomes (PFS, MFS, OS).6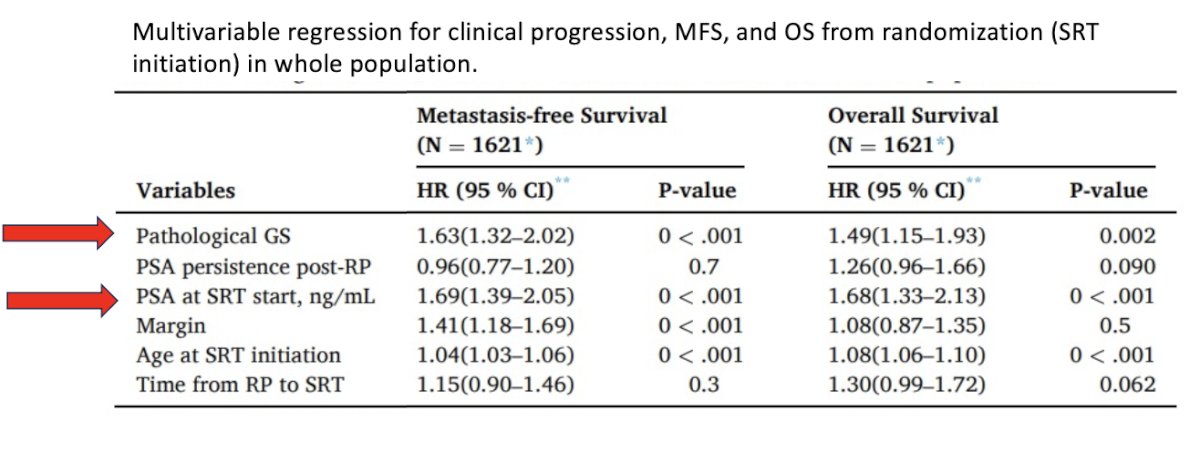
Dr. Tombal highlighted that since ADT is not particularly effective in this setting and carries significant toxicity, delaying its initiation appears reasonable. He discussed the role of immediate versus deferred ADT in prostate cancer patients with PSA-only relapse. Data from an observational follow-up study, which defined disease progression as metastasis on any imaging technique, severe cancer-related symptoms, PSA doubling time <12 months if PSA ≥10 ng/mL, or PSA doubling time ≤6 months based on three measurements, showed no difference in all-cause mortality at 10 years and only a 0.9% difference in prostate cancer-specific mortality.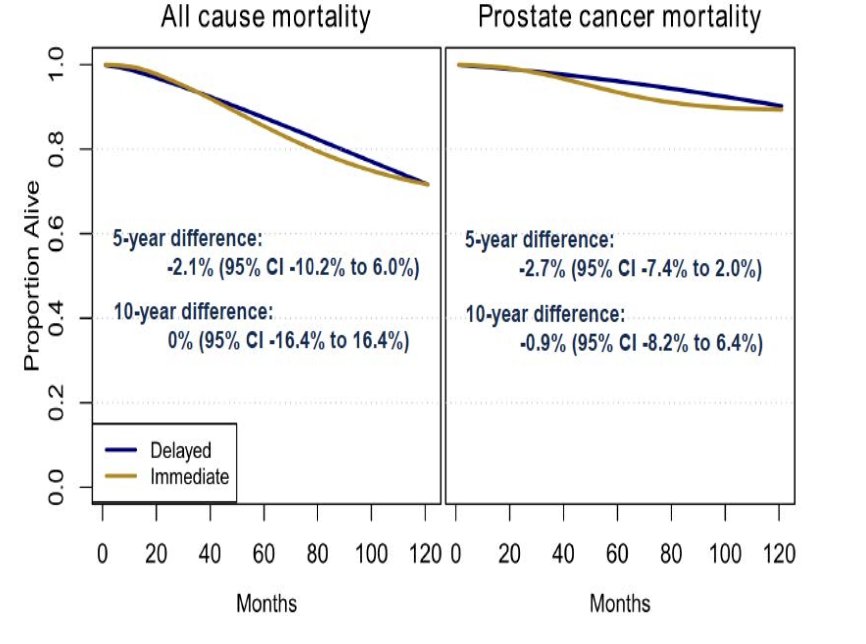
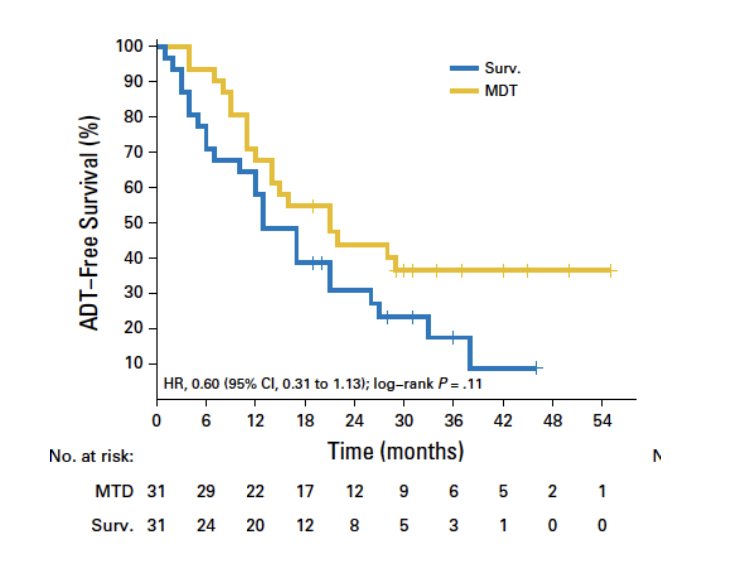
Dr. Tombal addressed the role of new imaging modalities like PSMA PET and their impact on treatment decisions. Data from a prospective, randomized, multicenter phase II trial evaluating surveillance versus metastasis-directed therapy (MDT) for oligometastatic prostate cancer recurrence showed that while ADT-free survival was longer in the MDT group, the difference was not statistically significant. This raises questions about whether MDT alone is sufficient to delay systemic therapy or if additional interventions are needed for better long-term outcomes.6
Moreover, when analyzing long-term outcomes and genetic predictors of response to metastasis-directed therapy versus observation, the median delay in initiating androgen deprivation therapy was approximately six months. However, no significant benefit was observed in terms of progression to castration-resistant prostate cancer, overall survival, or radiographic progression-free survival, suggesting that while metastasis-directed therapy may transiently postpone systemic therapy, its impact on long-term disease control remains uncertain.6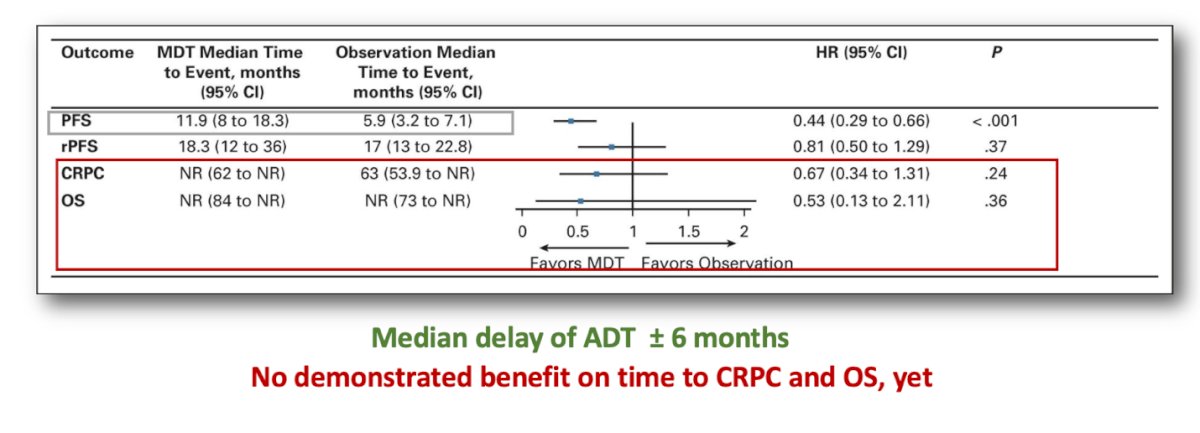
With the advent of treatment intensification trials such as EMBARK, the question arises whether delaying enzalutamide remains a viable option. EMBARK was a randomized phase III trial evaluating enzalutamide in combination with leuprolide acetate, as well as enzalutamide monotherapy, in patients with high-risk biochemical recurrence. At a median follow-up of five years, the combination of enzalutamide and leuprolide demonstrated a significant improvement in metastasis-free survival compared to leuprolide alone, highlighting the potential benefit of early treatment intensification in this setting.7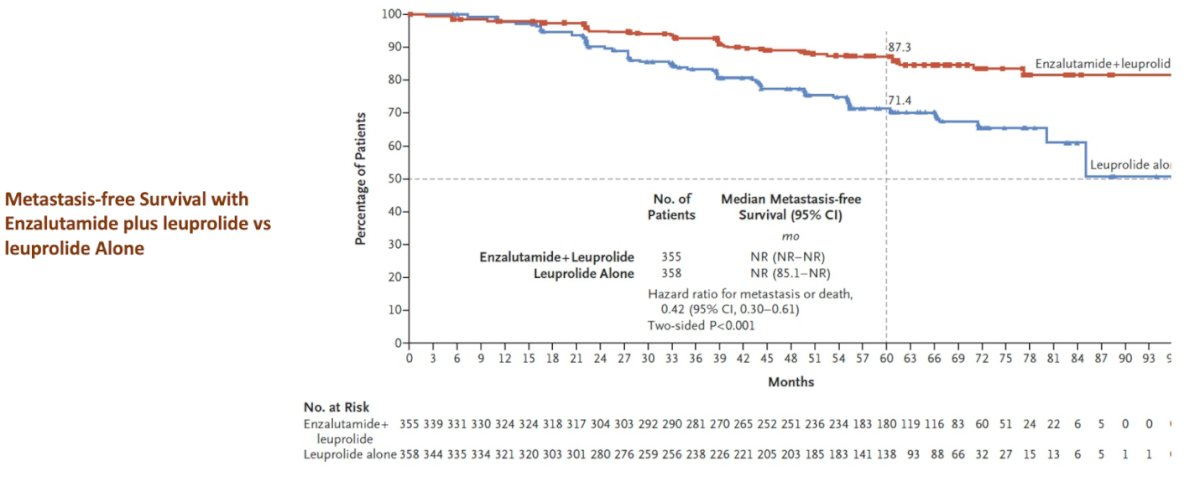
Dr. Tombal emphasized that, whether one agrees or not, the standard of care for very high-risk patients is androgen receptor pathway inhibitor therapy with or without androgen deprivation therapy for nine months, as established by the EMBARK trial. However, there remains an opportunity to build upon these findings by further increasing response rates and prolonging off-treatment duration. One potential approach to achieving this could be the incorporation of MDT.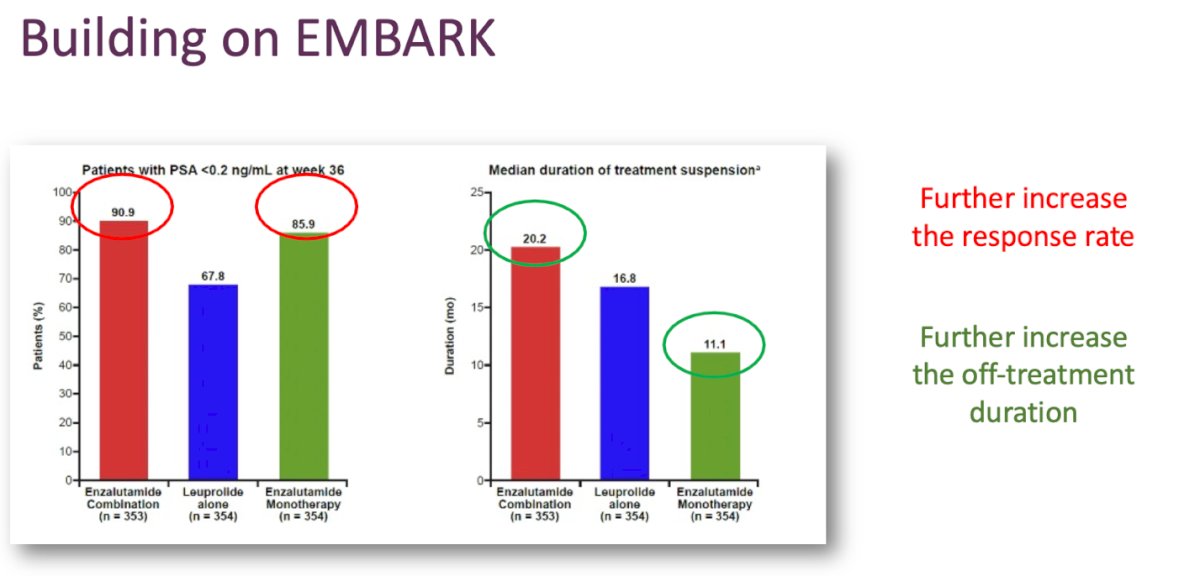
The EXTEND trial was a phase 2 randomized clinical study that evaluated 87 patients with oligometastatic prostate cancer receiving androgen deprivation therapy plus androgen receptor pathway inhibitor therapy, with or without metastasis-directed therapy. Notably, the combined treatment arm demonstrated a significant improvement in progression-free survival (hazard ratio 0.25, 95% confidence interval 0.12–0.55), as illustrated by the Kaplan-Meier curves below.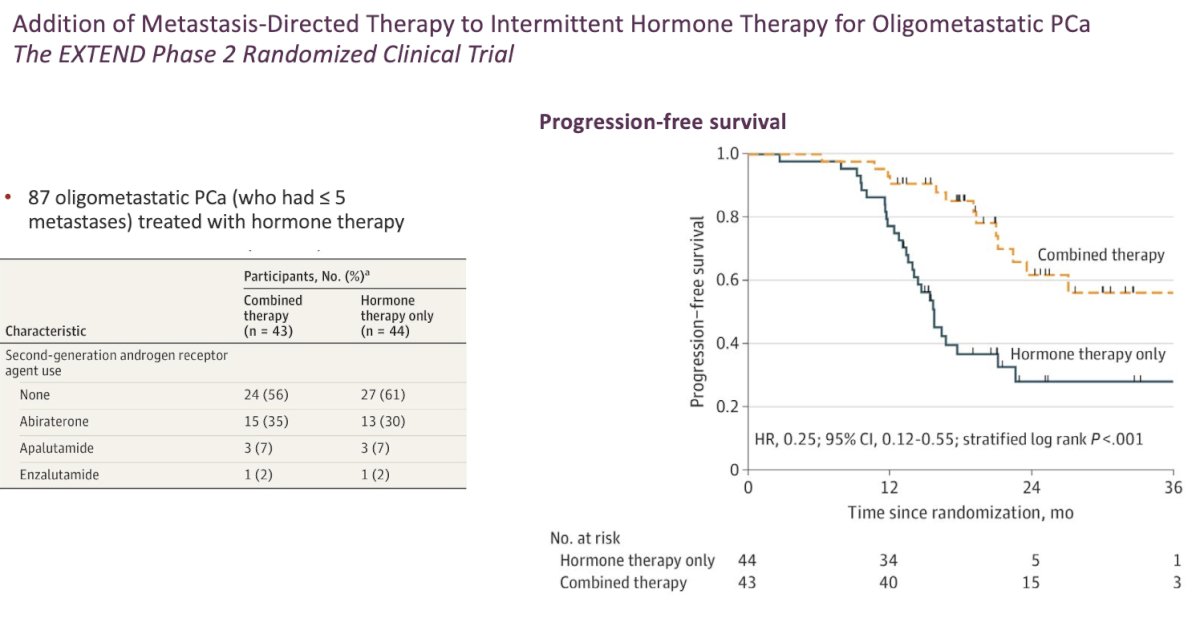
At the 2024 Advanced Prostate Cancer Consensus Conference, panelists were asked about their preferred approach for most patients with high-risk non-metastatic hormone-sensitive and oligometastatic prostate cancer detected on prostate-specific membrane antigen positron emission tomography. Notably, 70% of panelists voted in favor of a combination approach using ADT + MDT.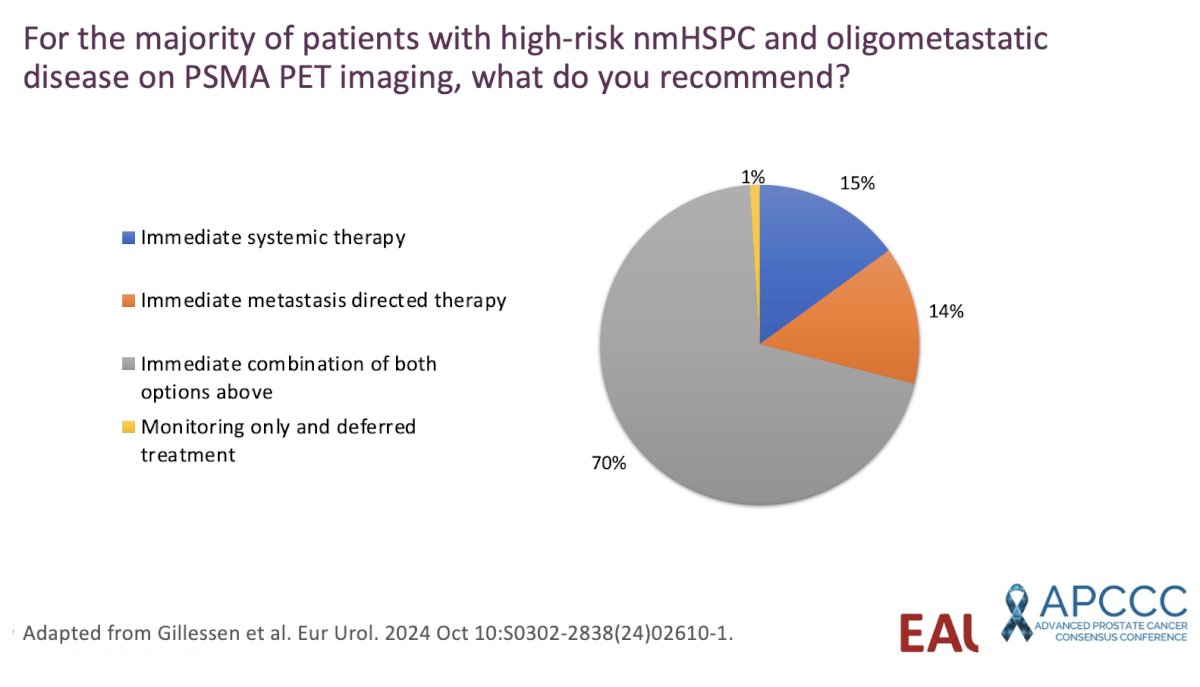
Dr. Tombal concluded his presentation with the following key messages:
- Not all biochemical recurrences are the same.
- Low-risk biochemical recurrence should be monitored closely rather than aggressively treated—these patients likely need reassurance rather than intervention.
- High-risk biochemical recurrence, however, requires early and intensive treatment:
- Initiate androgen receptor pathway inhibitor plus androgen deprivation therapy.
- Ideally, enroll the patient in a clinical trial to optimize strategies for imaging, radiotherapy, and treatment intensification.
- Use imaging to guide treatment decisions, treat aggressively when necessary, and consider de-escalation after nine months.
Presented by: Bertrand Tombal, MD, PhD, Professor of Physiology and Chair of the Division of Urology at the Université Catholique de Louvain and its Associated Hospital, the Cliniques Universitaires Saint-Luc, in Brussels, Belgium.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:- Freedland SJ, Humphreys EB, Mangold LA, Eisenberger M, Dorey FJ, Walsh PC, Partin AW. Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy. JAMA. 2005 Jul 27;294(4):433-9. doi: 10.1001/jama.294.4.433. PMID: 16046649.
- Thompson IM, Tangen CM, Paradelo J, Lucia MS, Miller G, Troyer D, Messing E, Forman J, Chin J, Swanson G, Canby-Hagino E, Crawford ED. Adjuvant radiotherapy for pathological T3N0M0 prostate cancer significantly reduces risk of metastases and improves survival: long-term followup of a randomized clinical trial. J Urol. 2009 Mar;181(3):956-62. doi: 10.1016/j.juro.2008.11.032. Epub 2009 Jan 23. PMID: 19167731; PMCID: PMC3510761.
- Shipley WU, Seiferheld W, Lukka HR, Major PP, Heney NM, Grignon DJ, Sartor O, Patel MP, Bahary JP, Zietman AL, Pisansky TM, Zeitzer KL, Lawton CA, Feng FY, Lovett RD, Balogh AG, Souhami L, Rosenthal SA, Kerlin KJ, Dignam JJ, Pugh SL, Sandler HM; NRG Oncology RTOG. Radiation with or without Antiandrogen Therapy in Recurrent Prostate Cancer. N Engl J Med. 2017 Feb 2;376(5):417-428. doi: 10.1056/NEJMoa1607529. PMID: 28146658; PMCID: PMC5444881.
- Parker CC, Clarke NW, Cook AD, Petersen PM, Catton CN, Cross WR, Kynaston H, Persad RA, Saad F, Logue J, Payne H, Amos C, Bower L, Raman R, Sayers I, Worlding J, Parulekar WR, Parmar MKB, Sydes MR; RADICALS Investigators. Randomised Trial of No, Short-term, or Long-term Androgen Deprivation Therapy with Postoperative Radiotherapy After Radical Prostatectomy: Results from the Three-way Comparison of RADICALS-HD (NCT00541047). Eur Urol. 2024 Nov;86(5):422-430. doi: 10.1016/j.eururo.2024.07.026. Epub 2024 Aug 31. PMID: 39217077; PMCID: PMC7617288.
- Pommier P, Xie W, Ravi P, Carrie C, Dignam JJ, Feng F, Sargos P, Sommer SG, Spratt DE, Tombal B, Van Poppel H, Sweeney C. Prognostic factors in post-prostatectomy salvage radiotherapy setting with and without hormonotherapy: An individual patient data analysis of randomized trials from ICECaP database. Radiother Oncol. 2024 Dec;201:110532. doi: 10.1016/j.radonc.2024.110532. Epub 2024 Sep 13. PMID: 39278317.
- Ost P, Reynders D, Decaestecker K, Fonteyne V, Lumen N, De Bruycker A, Lambert B, Delrue L, Bultijnck R, Claeys T, Goetghebeur E, Villeirs G, De Man K, Ameye F, Billiet I, Joniau S, Vanhaverbeke F, De Meerleer G. Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. J Clin Oncol. 2018 Feb 10;36(5):446-453. doi: 10.1200/JCO.2017.75.4853. Epub 2017 Dec 14. PMID: 29240541.
- Freedland SJ, de Almeida Luz M, De Giorgi U, Gleave M, Gotto GT, Pieczonka CM, Haas GP, Kim CS, Ramirez-Backhaus M, Rannikko A, Tarazi J, Sridharan S, Sugg J, Tang Y, Tutrone RF Jr, Venugopal B, Villers A, Woo HH, Zohren F, Shore ND; EMBARK Study. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med. 2023 Oct 19;389(16):1453-1465. doi: 10.1056/NEJMoa2303974. PMID: 37851874.