(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain was host to the clinically relevant questions in the management of advanced, hormone-sensitive prostate cancer: Thematic session. Dr. Ursula Vogl discussed treatment options for patients with high-volume disease at HSPCA and with poor response to triple therapy.
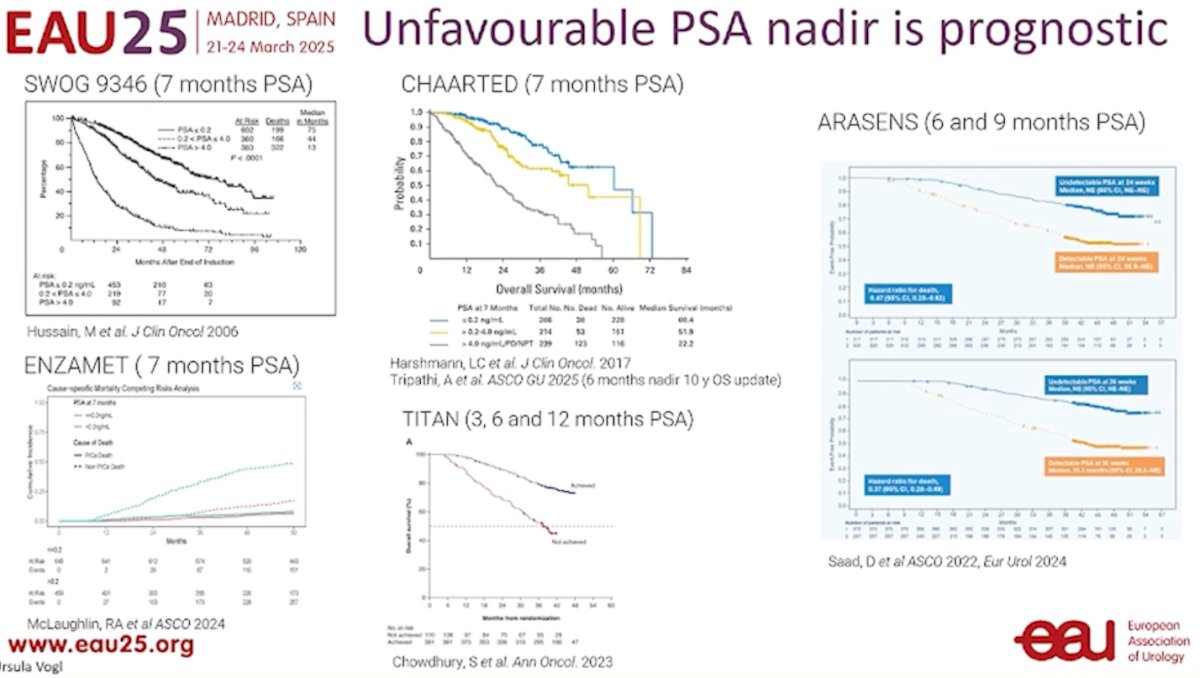
We have a benchmark for what is considered a PSA nadir (PSA <0.2), which is a well-established prognostic marker. The time required to reach this nadir is also clinically significant. Data supporting this come from studies on ADT monotherapy, ADT combined with docetaxel, and doublet trials involving ADT plus an ARPI as shown below.
The genomic profile plays a role in predicting outcomes in mHSPC. Evidence suggests that time to CRPC is shorter in patients with alterations in AR, TP53, PTEN, and RB1. Moreover, AR aberrations detected in ctDNA at baseline have been associated with shorter OS, as shown in an exploratory biomarker analysis from the phase 3 TITAN trial.1 Tumor sequencing from STAMPEDE has also linked an increasing copy number burden with a higher risk of progression and death in both high- and low-volume disease.2 However, Dr. Vogl noted that while this data is promising, it is not yet applicable in daily clinical practice and does not currently guide treatment decisions for patients with mHSPC.
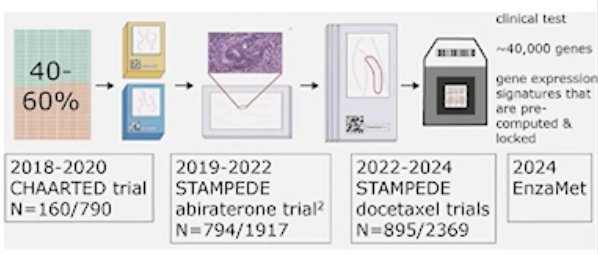
A study profiling 160 patients from CHAARTED using the Decipher microarray platform was the first to comprehensively map the transcriptomic landscape of mHSPC. A high Decipher score identified synchronous M1 PCa patients who benefited from the addition of docetaxel to ADT in mHSPC, a finding also observed in the STAMPEDE trial.
The Decipher genomic classifier has been shown to be strongly prognostic in advanced prostate cancer, as demonstrated in an ancillary study of STAMPEDE (Arm G: ADT + abiraterone). A similar profiling study from ENZAMET is currently analyzing data, with results expected soon.
Dr. Vogl emphasized that, to date, there is no evidence to change the treatment strategy based on PSA nadir. However, it is essential to ensure the following:
- Testosterone suppression (<1.7 nmol/L or <50 ng/dL)
- Compliance with oral LHRH antagonists and/or ARPI
- In de novo low-volume disease, radiotherapy to the prostate ± metastasis-directed therapy (MDT) should be included
- Regular imaging every six months
If PSA nadir is poor, we should be prepared for mCRPC, because it will likely develop soon. For these patients, we should start performing somatic NGS, genetic counseling, and germline testing.
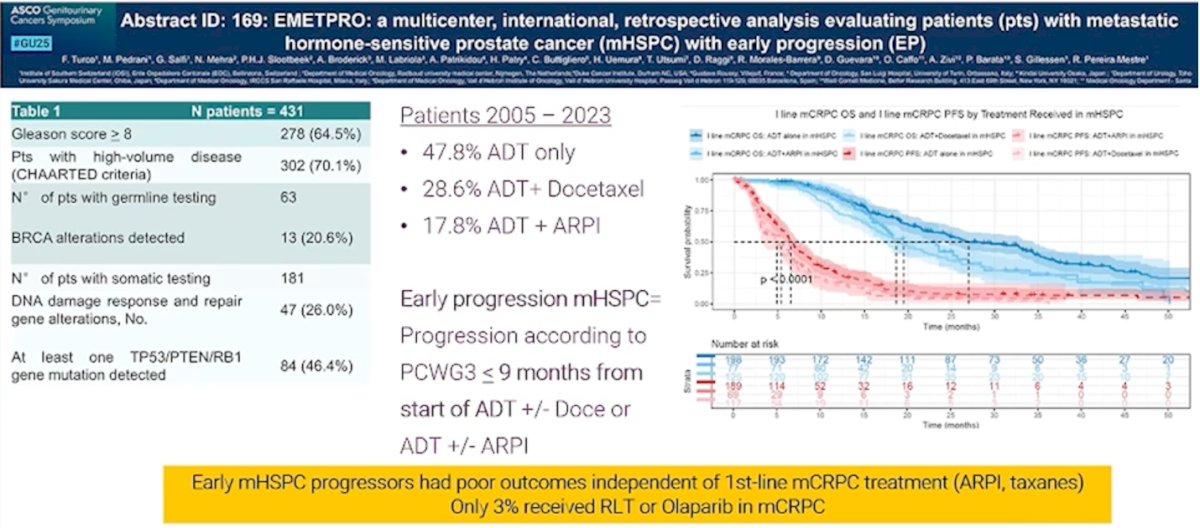
PSA poor responders do not automatically equate to early progressors. Data from the EMETPRO study, presented at ASCO GU, analyzed 431 patients with mHSPC. Early progression in mHSPC was defined as progression per PCWG3 criteria within ≤9 months from the start of ADT ± docetaxel or ADT ± ARPI. These early progressors had poor outcomes regardless of first-line mCRPC treatment. Limitations were the retrospective study design and only 3% of patients in this study received radioligand therapy (RLT) or olaparib in the mCRPC setting. However, it remains unclear whether these therapies could effectively rescue early progressors.
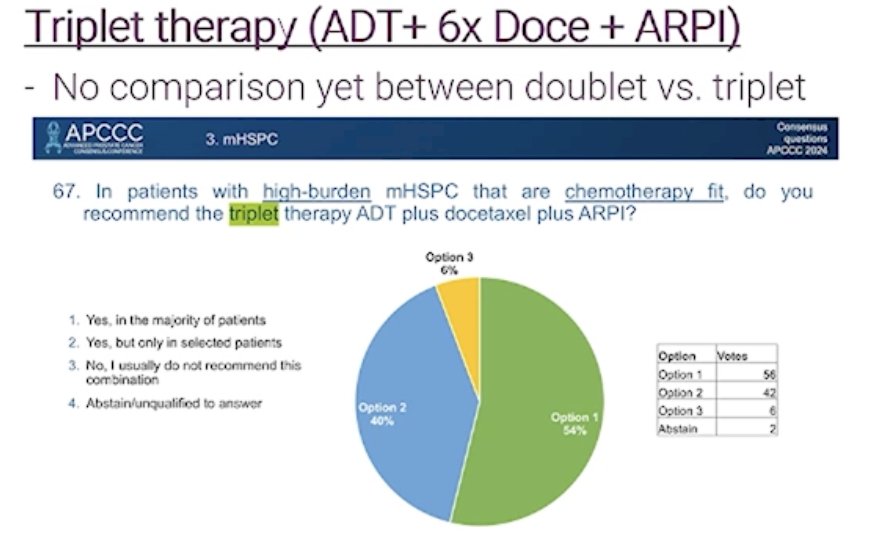
At APCC 2024, the audience was asked whether they would recommend triplet therapy for chemotherapy-fit patients with high-volume mHSPC. Notably, only 6% of panelists would not recommend this combination. There is a growing trend in daily clinical practice to offer triplet therapy to these patients. The key question now is: what do we offer patients treated with triplet therapy who progress to mCRPC?
Dr. Vogl concluded her presentation by discussing potential strategies for poor responders or early progressors with mHSPC. The key considerations were:
- If we choose Cabazitaxel: Is it as effective in ARPI- and docetaxel-pretreated mHSPC patients as in mCRPC? Phase 3 trials (TROPIC and CARD) included patients who had failed ARPI and docetaxel in the mCRPC setting.
- Can modern agents in first-line mCRPC treatment (177Lu-PSMA, PARP inhibitors for BRCA-mutated/selected HRD-mutated patients) improve prognosis?
- Should we use modern drugs (RLT, PARP inhibitors, targeted therapies) earlier in mHSPC?
Presented by: Ursula Vogl, MD, Medical Oncologist at Ente Ospedaliero Cantonale, Bellinzona, Switzerland.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:- Neeraj Agarwal et al. Genomic aberrations associated with overall survival (OS) in metastatic castration-sensitive prostate cancer (mCSPC) treated with apalutamide (APA) or placebo (PBO) plus androgen deprivation therapy (ADT) in TITAN.. JCO 40, 5066-5066(2022).DOI:10.1200/JCO.2022.40.16_suppl.5066
- Emily Grist et al. Copy number profiles of primary tumors for risk stratification of advanced prostate cancer: A biomarker study embedded in the multicenter STAMPEDE trial.. JCO 39, 5021-5021(2021). DOI:10.1200/JCO.2021.39.15_suppl.5021