(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025, was host to the clinically relevant questions in the management of advanced, hormone-sensitive prostate cancer: Thematic session. Dr. Antti Sakari Rannikko discussed why systemic treatment intensification is the way to go for High-risk biochemical recurrence with positive PSMA PET.
Prior to Dr. Ranniko’s debate, Dr. Pawel Rajwa presented a case of a patient with cT2N0M0 prostate cancer (PSA 11.3 ng/mL, Grade Group 4) who underwent radical prostatectomy, revealing pT2N0M0 with Grade Group 5 disease. During follow-up, the patient experienced biochemical recurrence (PSA 1.02 ng/mL, PSA doubling time <6 months) and was found to have oligometastatic disease on PSMA PET/CT.
Dr. Rannikko highlighted three key questions when approaching a case like this: When should salvage radiotherapy (sRT) be given? What is the optimal systemic therapy and when should it be initiated? And importantly, is the patient young, healthy, and asymptomatic considering they may require lifelong treatment, how will this impact their quality of life?
In conventional imaging, disease volume in mHSPC is crucial, as radiotherapy (RT) has shown a survival benefit only in patients with low-volume disease.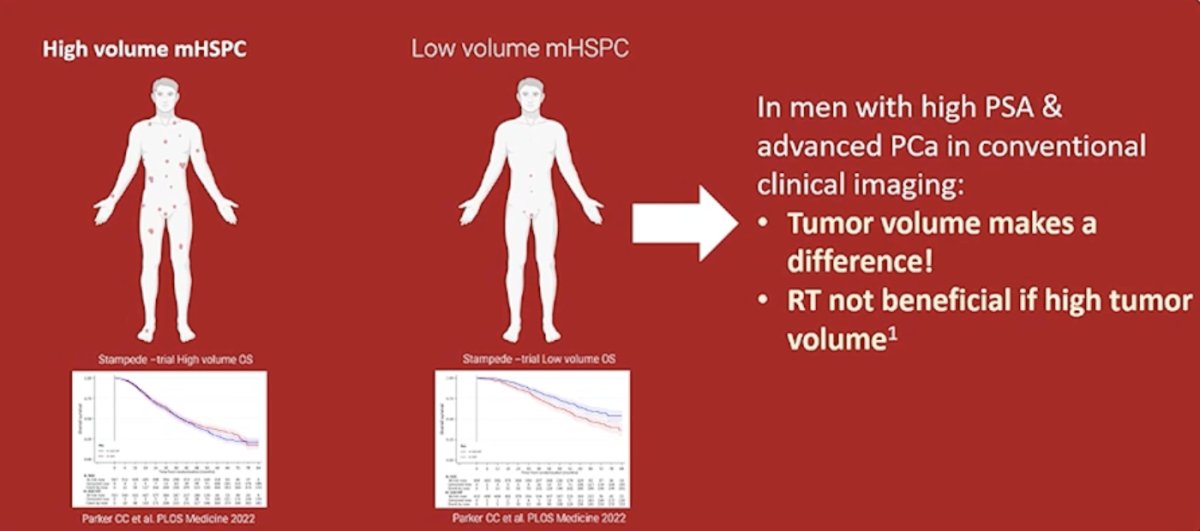
However, in men with low PSA and negative conventional imaging but positive PSMA PET/CT, it is unclear if tumor volume impacts outcomes. In these cases, PSA can serve as a surrogate for tumor burden.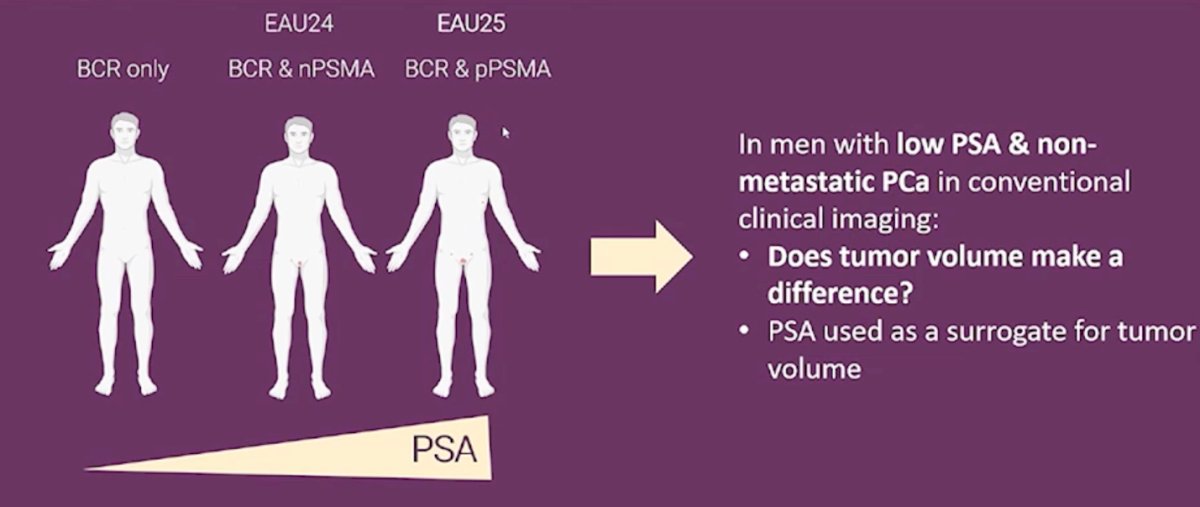
Dr. Tilki et al. conducted a study evaluating PSA levels at the time of salvage RT after RP, showing that administering salvage RT at PSA levels above 0.25 ng/ml was associated with increased all-cause mortality.1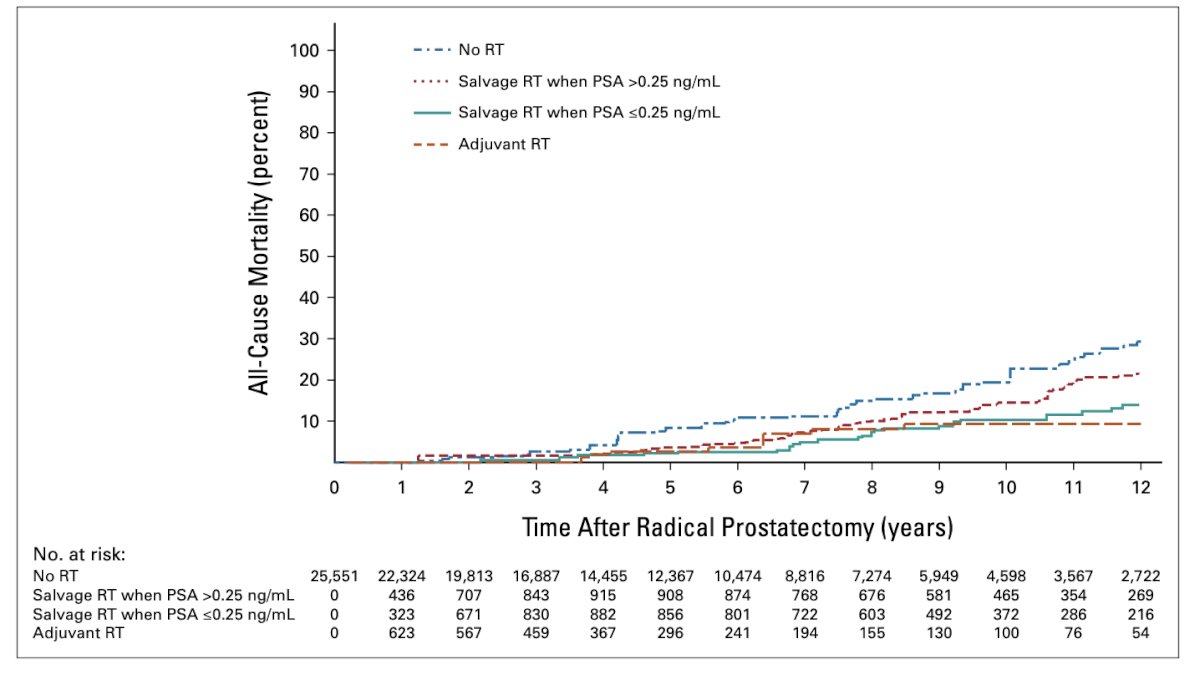
Dr. Rannikko posed the question: If salvage RT alone is not enough, should we add systemic therapy? The answer is yes. In the RTOG 9601 study, adding systemic therapy (bicalutamide 150 mg for 24 months) to salvage RT improved metastasis-free survival, particularly in patients with pre-salvage RT PSA > 0.61 ng/ml.2 The key question remains: does a longer duration of ADT further improve MFS?
The patient presented at the beginning of this session had EAU high-risk biochemical recurrence (PSA doubling time <1 year and grade group 5 disease). Despite negative conventional imaging, he likely has microscopic oligometastatic disease. However, PSMA PET/CT identified a single lesion, placing him in a transitional stage between micrometastatic and oligometastatic disease.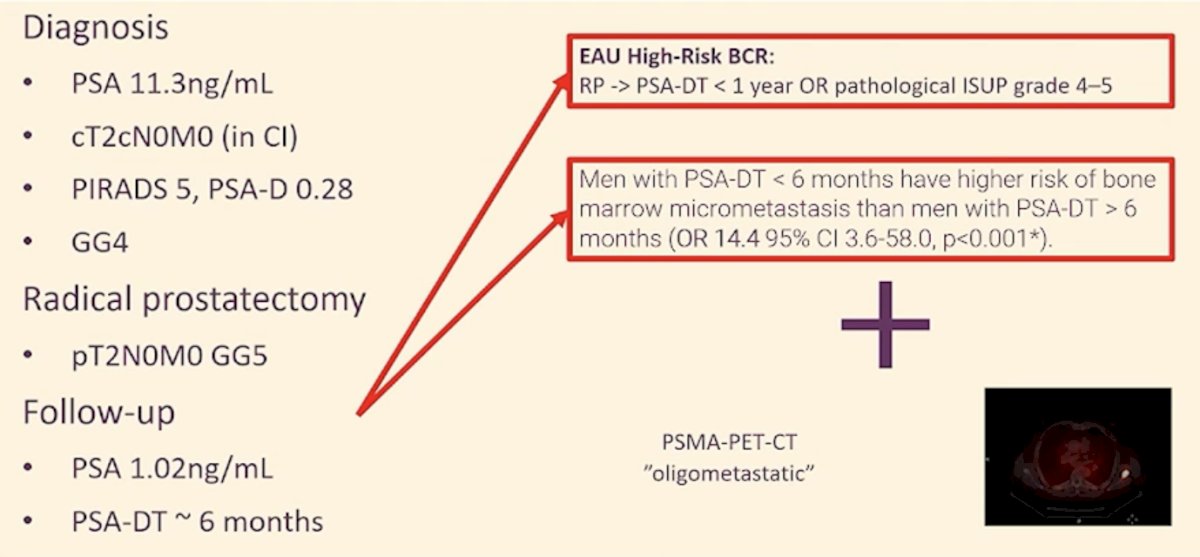
Studies comparing metastasis-directed therapy (MDT) to observation in these patients are limited to small phase 2 trials, with endpoints such as ADT-free survival and progression on conventional imaging. This raises the question of whether these endpoints are truly clinically meaningful in guiding treatment decisions.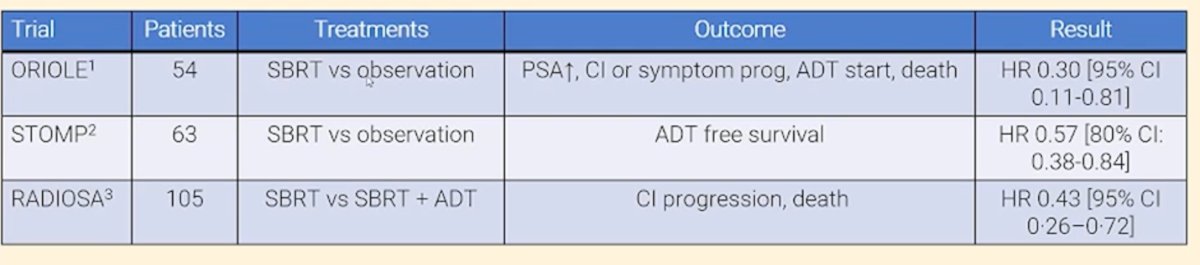
On the other hand, two phase 3 trials have investigated treatment intensification with an ARPI in this setting. The PRESTO trial (NCT03009981) randomized patients with biochemically relapsed prostate cancer (PSA doubling time ≤ 9 months) and no distant metastases on conventional imaging to ADT alone, ADT + apalutamide, or ADT + apalutamide + abiraterone acetate plus prednisone for 52 weeks. The study demonstrated that adding apalutamide to ADT improved PSA progression-free survival. However, the clinical significance of this outcome remains uncertain, and the role of PSMA PET/CT imaging in guiding treatment decisions is still unclear.3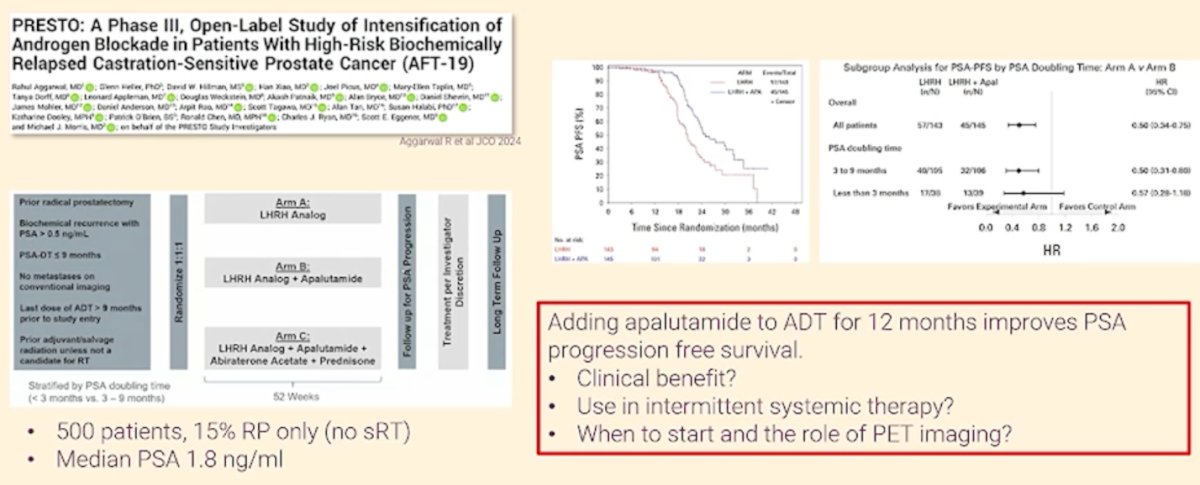
The EMBARK trial enrolled 1,068 patients with high-risk BCR (PSA doubling time ≤9 months and PSA ≥1 ng/ml after radical prostatectomy or ≥2 ng/ml above nadir following primary EBRT) in a three-arm, randomized phase 3 trial. Patients with no evidence of metastasis on conventional imaging were assigned (1:1:1) to ADT, ADT + enzalutamide, or enzalutamide monotherapy, demonstrating a clear MFS benefit with treatment intensification.4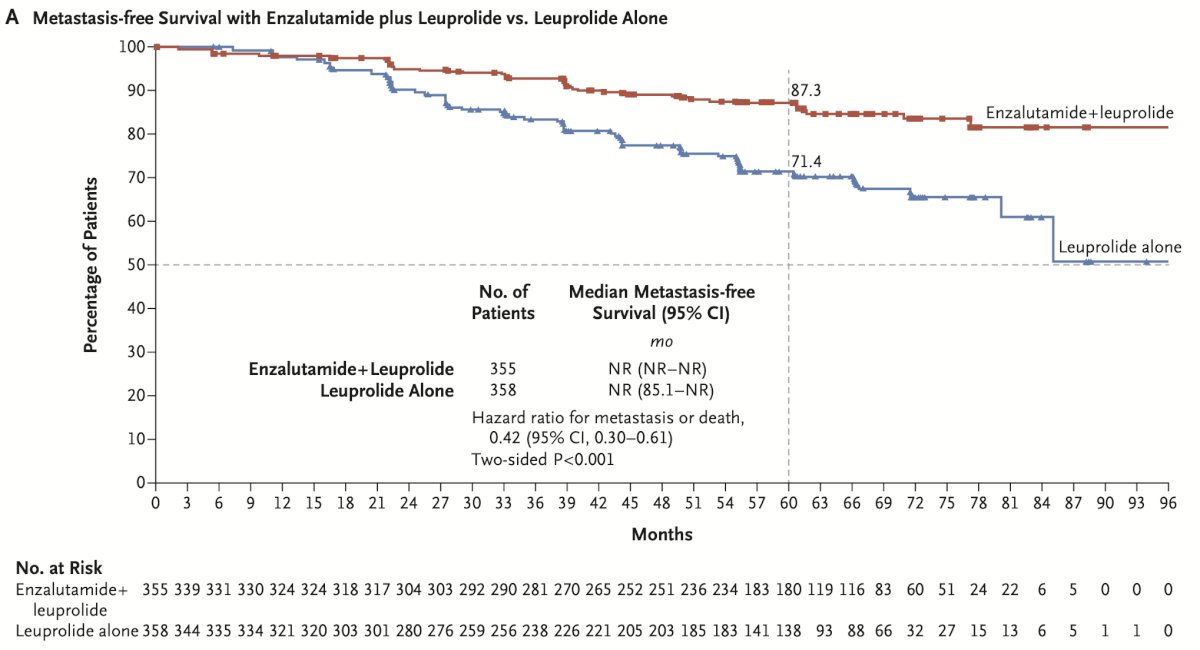
When selecting treatment, comorbidities must be considered. For example, this patient had four cardiovascular risk factors—myocardial infarction (2 years ago), hypertension, hypercholesterolemia, and diabetes—placing him in a high-CVD risk group. A cardiology/internal medicine consultation should be obtained before initiating therapy.
Dr. Rannikko concluded his presentation with the following key points:
- Asymptomatic men may develop symptoms with ADT ± ARSI.
- There is evidence supporting the addition of ADT to enzalutamide (or enzalutamide monotherapy) for improving MFS.
- ADT + enzalutamide has shown no clear OS benefit, only a signal.
- Many patients may do well with close follow-up alone.
- It remains unknown whether early treatment is superior to delayed intervention.
- Cardiovascular risks must be considered when selecting treatment options.
- Intermittent therapy could be a potential strategy.
Presented by: Professor Antti Sakari Rannikko, MD, Associate Professor, Urology, University of Helsinki and the Helsinki University Central Hospital, Helsinki (HUCH).
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:
- Tilki D, Chen MH, Wu J, Huland H, Graefen M, Mohamad O, Cowan JE, Feng FY, Carroll PR, D'Amico AV. Prostate-Specific Antigen Level at the Time of Salvage Therapy After Radical Prostatectomy for Prostate Cancer and the Risk of Death. J Clin Oncol. 2023 May 1;41(13):2428-2435. doi: 10.1200/JCO.22.02489. Epub 2023 Mar 1. PMID: 36857638; PMCID: PMC10150889.
- Shipley WU, Seiferheld W, Lukka HR, Major PP, Heney NM, Grignon DJ, Sartor O, Patel MP, Bahary JP, Zietman AL, Pisansky TM, Zeitzer KL, Lawton CA, Feng FY, Lovett RD, Balogh AG, Souhami L, Rosenthal SA, Kerlin KJ, Dignam JJ, Pugh SL, Sandler HM; NRG Oncology RTOG. Radiation with or without Antiandrogen Therapy in Recurrent Prostate Cancer. N Engl J Med. 2017 Feb 2;376(5):417-428. doi: 10.1056/NEJMoa1607529. PMID: 28146658; PMCID: PMC5444881.
- Aggarwal R, Heller G, Hillman DW, Xiao H, Picus J, Taplin ME, Dorff T, Appleman L, Weckstein D, Patnaik A, Bryce A, Shevrin D, Mohler J, Anderson D, Rao A, Tagawa S, Tan A, Halabi S, Dooley K, O'Brien P, Chen R, Ryan CJ, Eggener SE, Morris MJ; EORTC-55994 Study Group. PRESTO: A Phase III, Open-Label Study of Intensification of Androgen Blockade in Patients With High-Risk Biochemically Relapsed Castration-Sensitive Prostate Cancer (AFT-19). J Clin Oncol. 2024 Apr 1;42(10):1114-1123. doi: 10.1200/JCO.23.01157. Epub 2024 Jan 23. PMID: 38261983; PMCID: PMC11637124.
- Freedland SJ, de Almeida Luz M, De Giorgi U, Gleave M, Gotto GT, Pieczonka CM, Haas GP, Kim CS, Ramirez-Backhaus M, Rannikko A, Tarazi J, Sridharan S, Sugg J, Tang Y, Tutrone RF Jr, Venugopal B, Villers A, Woo HH, Zohren F, Shore ND; EMBARK Study. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med. 2023 Oct 19;389(16):1453-1465. doi: 10.1056/NEJMoa2303974. PMID: 37851874.