(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025, was host to the clinically relevant questions in the management of advanced, hormone-sensitive prostate cancer: Thematic session. Dr. Brian Chapin discussed the management of locally advanced prostate cancer and delved into what is the standard of care in 2025, including intensified approaches with surgery.
Dr. Chapin began by presenting a clinical scenario of a patient with cT3N0M0 on conventional imaging. He highlighted the common confusion between locally advanced and high-risk prostate cancer, emphasizing that while all locally advanced cases are high-risk, not all high-risk cases are locally advanced—and they should not be treated the same way.
One key insight we gained from the surgical approach is the significant rate of pathologic reclassification. Gleason 4+4 is downgraded in 46-62% of cases, while clinical T3 is downstaged to pT2 in 26-29% of patients. Additionally, occult node-positive disease is identified in 25-39% of cN0 cases, including 20-25% of patients with negative PSMA PET/CT scans (miN0). Notably, PSMA PET staging in high-risk prostate cancer detects M1 disease in 15-27% of patients initially classified as N1.
According to EAU guidelines, treatment options for locally advanced prostate cancer include radiotherapy with 2 years of ADT (strong recommendation) and radical prostatectomy (weak recommendation) with extended pelvic LND (strong recommendation) as part of a multimodal approach.1
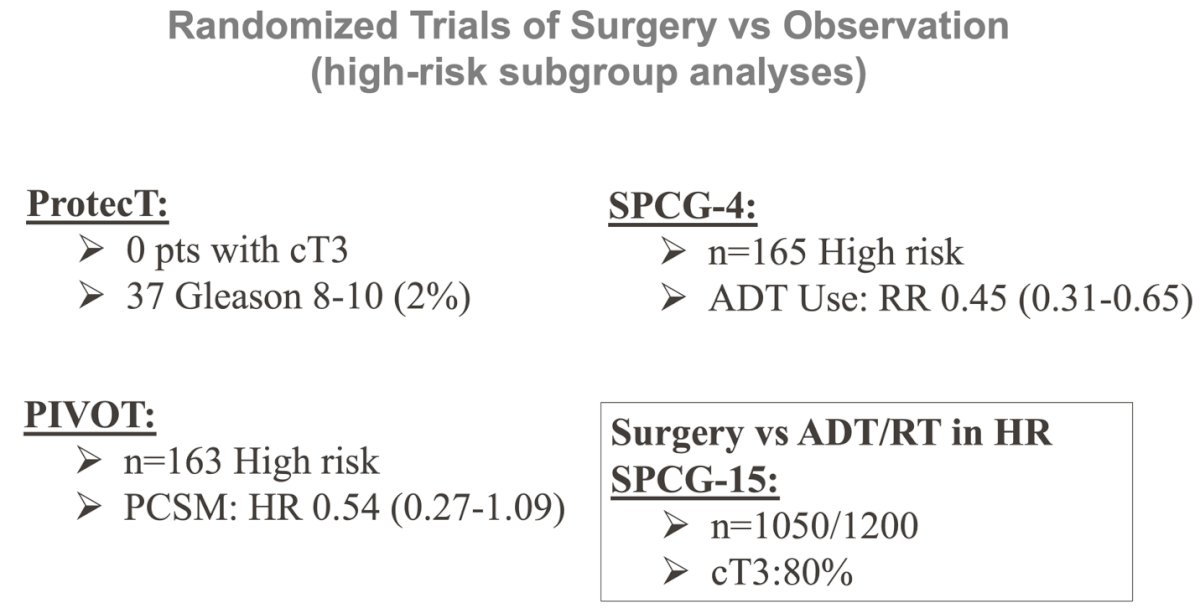
There are few RCTs directly comparing surgery to RT or observation in high-risk prostate cancer. The available trials, which included relatively small numbers of high-risk patients, compared surgery and radiation therapy to observation. In the PIVOT study, the HR for prostate cancer-specific mortality (0.54, 95% CI 0.27-1.09) was not statistically significant, though the trial was underpowered for this outcome in this subgroup of patients.2 In SPCG-4, there was increased use of ADT in patients with high-risk disease (n=165). The results of SPCG-15, which is comparing surgery vs. RT + ADT in high-risk patients, are eagerly awaited, and the trial is nearly fully accrued.
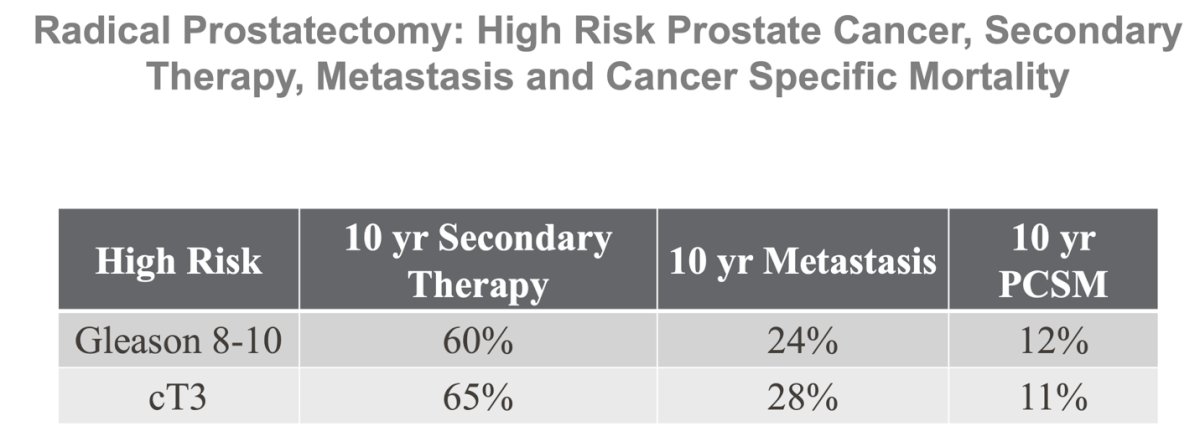
Retrospective data on patients undergoing surgery for locally advanced prostate cancer show a 10-year metastasis rate of 24-28% in those with Gleason GG4-5 or cT3 disease, with over 60% requiring secondary therapy. The majority will eventually receive additional treatments.
Adjuvant Therapies: Intensifying therapy
Dr. Chapin reviewed data on various adjuvant strategies, highlighting that adjuvant radiation after RP improves survival outcomes, immediate ADT in N1 disease enhances survival, and adjuvant RT with or without ADT in N1 patients is effective.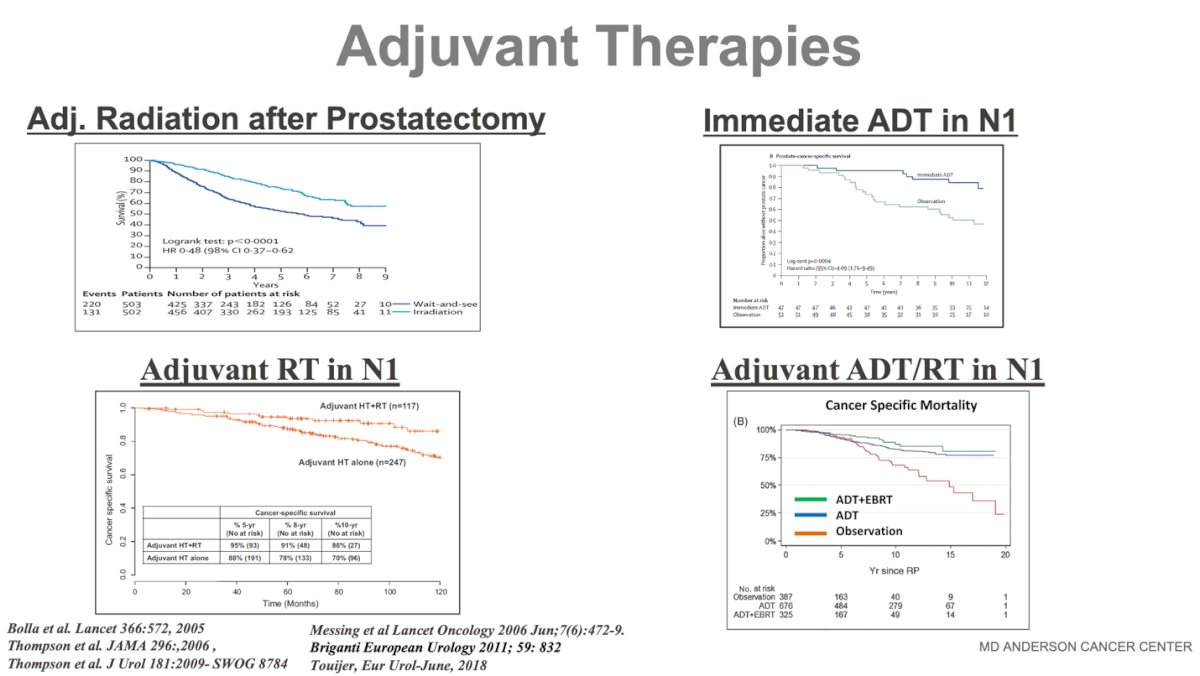
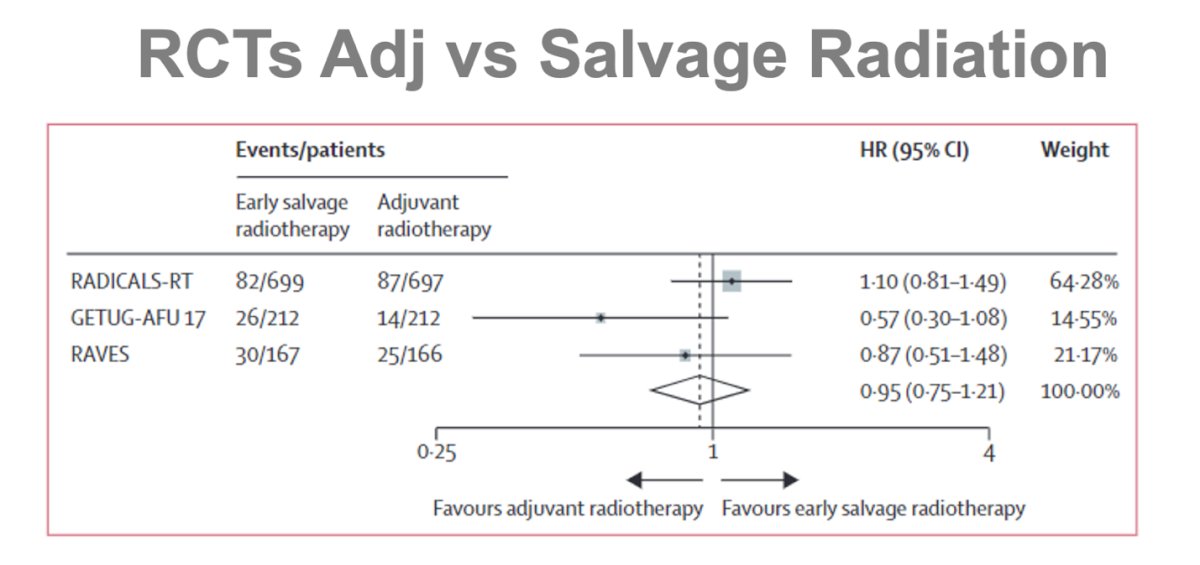
The ARTISTIC meta-analysis, comparing adjuvant vs. salvage RT across three RCTs, demonstrated noninferiority for salvage RT. However, most patients had more favorable disease features—primarily Gleason 7, with <20% having Gleason 8-10 or pT3b, and <5% with pN1. Dr. Chapin questioned the generalizability of these findings to locally advanced disease and emphasized that shared decision-making remains crucial in adjuvant therapy decision making.3
Neoadjuvant therapy
There are many reasons to consider neoadjuvant therapy in high-risk or locally advanced PCa. In the short term, it can downstage tumors and decrease positive surgical margins, while in the long term, it may eliminate delays in therapy initiation, target extraprostatic disease systemically, and potentially improve PFS, MFS, and OS. Additionally, neoadjuvant trials provide a window of opportunity for personalized sequential therapy and long-term treatment optimization.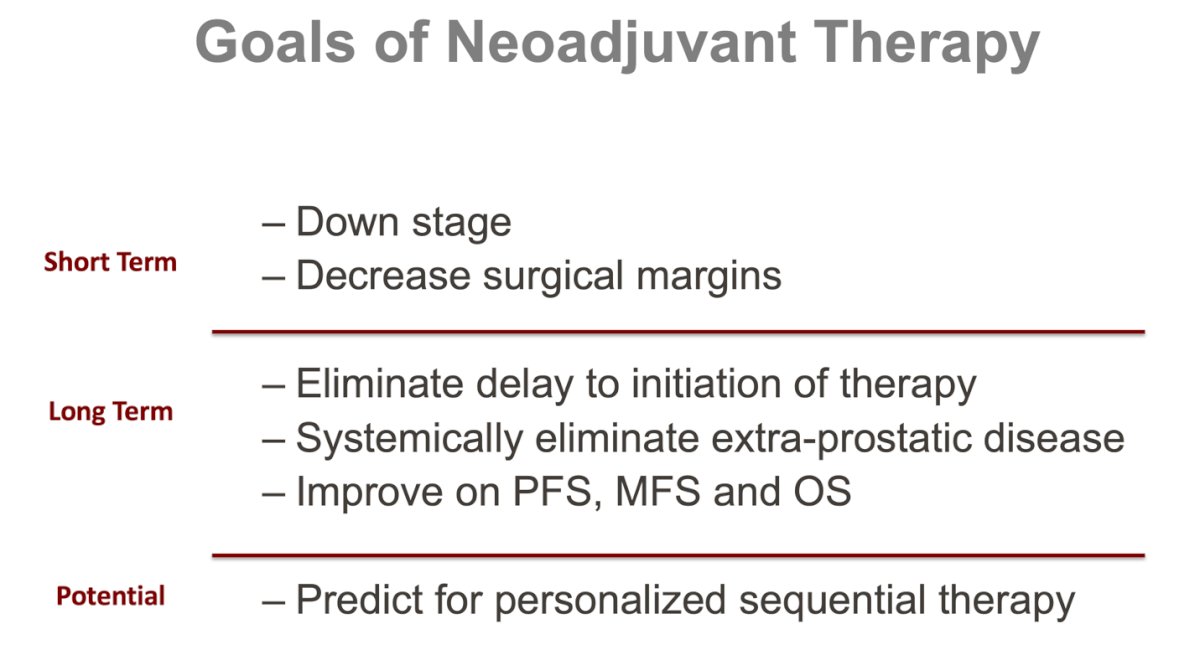
One of the largest RCTs, CALGB 90203 (Alliance), evaluated neoadjuvant chemohormonal therapy before RP in high-risk prostate cancer. While the primary endpoint of 3-year biochemical progression-free survival (B-PFS) was not met, the study showed improved B-PFS at 8 years, as well as improved MFS and OS. However, the risk of Grade 3-4 AEs was 26% and 19%, respectively, leading most experts to conclude that the toxicity is too high to consider it standard of care.4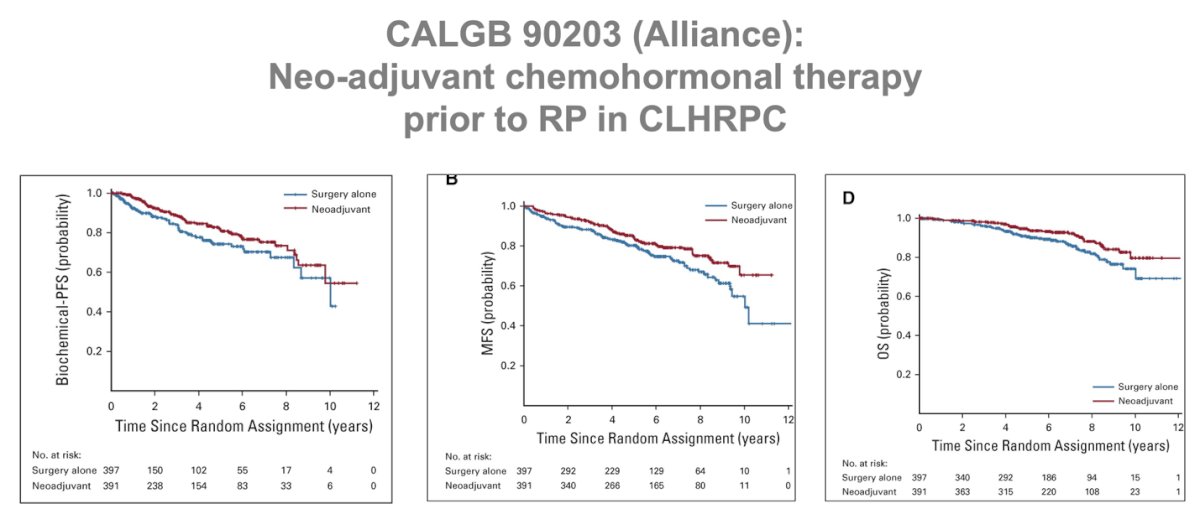
The phase 3 PROTEUS trial (NCT03767244) is evaluating perioperative apalutamide plus ADT and RP vs perioperative ADT in patients with high-risk, localized, or locally advanced prostate cancer. This study is expected to provide important insights, with data anticipated for release later this year. The study design is shown below:
Active trials for biomarker compartmentalization
The GUNS trial (NCT04812366) is a multicenter, adaptive phase II umbrella study evaluating ARPI combination therapies in high-risk, localized prostate cancer (high-volume pattern 4, 5). Its goal is to define the impact of biomarker-selected targeted therapies on pathological response, including complete response (pCR) or minimal residual disease (MRD) <5 mm. Sub-protocols combine ARPI doublets with agents targeting specific genomic biomarkers, such as docetaxel for RB1, PTEN, and/or TP53 loss, niraparib for DNA damage repair (DDR) deficiency, and anti-PD-L1 for mismatch repair (MMR) deficiency.

The NAUTILUS trial (NCT06066437) is a phase 1/2 study evaluating Lu-177 with or without ADT, followed by robot-assisted radical prostatectomy and extended pelvic lymph node dissection in patients with high-risk or very high-risk prostate cancer. Its design is similar to the LuTectomy study conducted in Australia.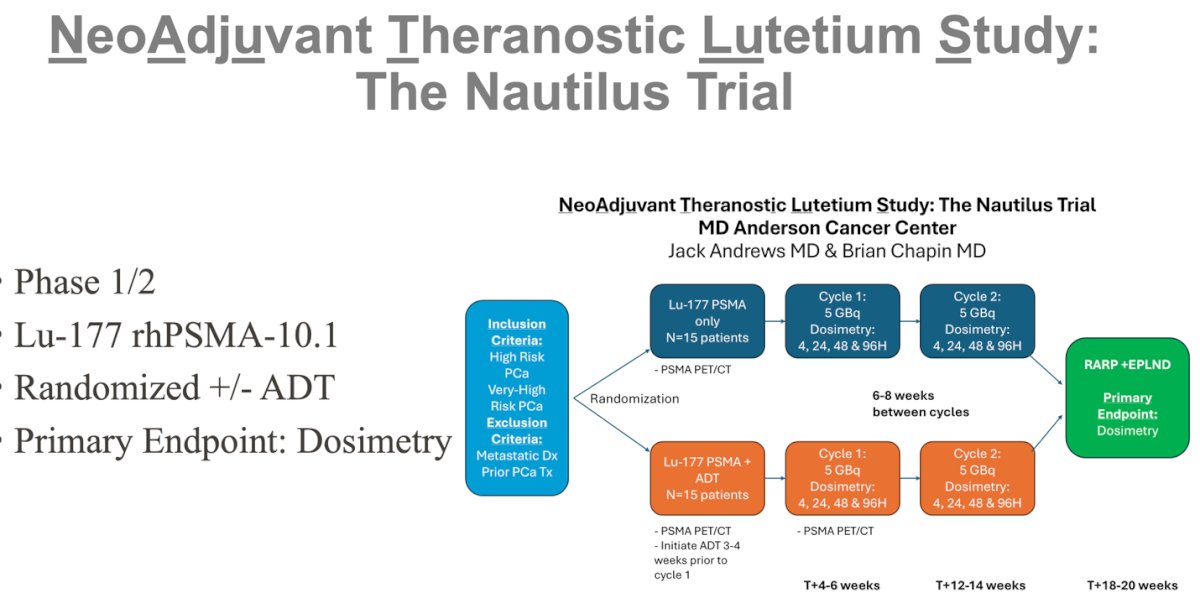
Dr. Chapin concluded his presentations with the following key messages:
- Locally advanced prostate cancer we know has lethal potential
- High level data supporting surgery is lacking
- Surgery as the initial step in multimodality therapy may provide informed application of subsequent adjuvant or salvage treatments
- Intensified therapies with surgery are promising with trials underway
Presented by: Brian F. Chapin, MD, Associate Professor in the Department of Urology at The University of Texas MD Anderson Cancer Center. Houston, TX.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:- EAU Guidelines. Edn. Presented at the EAU Annual Congress Paris April 2024. ISBN 978-94-92671-23-3
- Wilt TJ, Vo TN, Langsetmo L, Dahm P, Wheeler T, Aronson WJ, Cooperberg MR, Taylor BC, Brawer MK. Radical Prostatectomy or Observation for Clinically Localized Prostate Cancer: Extended Follow-up of the Prostate Cancer Intervention Versus Observation Trial (PIVOT). Eur Urol. 2020 Jun;77(6):713-724. doi: 10.1016/j.eururo.2020.02.009. Epub 2020 Feb 21. Erratum in: Eur Urol. 2022 Feb;81(2):e52. doi: 10.1016/j.eururo.2021.11.009. PMID: 32089359.
- Vale CL, Fisher D, Kneebone A, Parker C, Pearse M, Richaud P, Sargos P, Sydes MR, Brawley C, Brihoum M, Brown C, Chabaud S, Cook A, Forcat S, Fraser-Browne C, Latorzeff I, Parmar MKB, Tierney JF; ARTISTIC Meta-analysis Group. Adjuvant or early salvage radiotherapy for the treatment of localised and locally advanced prostate cancer: a prospectively planned systematic review and meta-analysis of aggregate data. Lancet. 2020 Oct 31;396(10260):1422-1431. doi: 10.1016/S0140-6736(20)31952-8. Epub 2020 Sep 28. PMID: 33002431; PMCID: PMC7611137.
- Eastham JA, Heller G, Halabi S, Monk JP 3rd, Beltran H, Gleave M, Evans CP, Clinton SK, Szmulewitz RZ, Coleman J, Hillman DW, Watt CR, George S, Sanda MG, Hahn OM, Taplin ME, Parsons JK, Mohler JL, Small EJ, Morris MJ. Cancer and Leukemia Group B 90203 (Alliance): Radical Prostatectomy With or Without Neoadjuvant Chemohormonal Therapy in Localized, High-Risk Prostate Cancer. J Clin Oncol. 2020 Sep 10;38(26):3042-3050. doi: 10.1200/JCO.20.00315. Epub 2020 Jul 24. PMID: 32706639; PMCID: PMC7479762.