(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain was host to the session Progress and Controversies in oncological urology from the EAU Section of Oncological Urology. Dr. Jeremy Teoh debated why there is a plea for local therapy in oligoprogression after first-line systemic therapy in RCC.
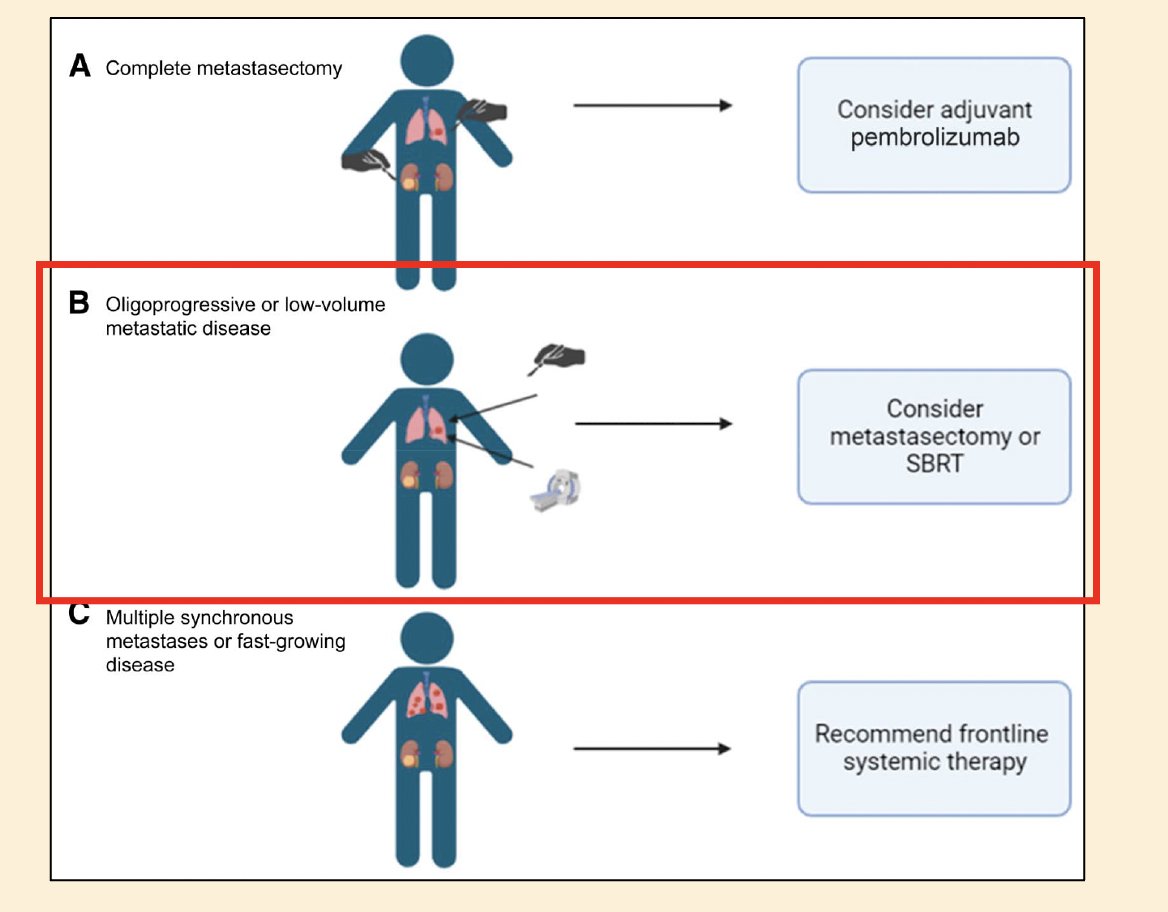
Dr. Teoh began his presentation by emphasizing the importance of differentiating between oligometastatic and oligoprogressive disease in renal cell carcinoma (RCC). Oligometastatic disease is defined as having fewer than five metastatic sites, whereas oligoprogressive disease is characterized by progression in a maximum of three to five sites while all other tumor sites remain controlled by systemic therapy. Notably, patients with oligoprogressive or oligometastatic disease are often considered for metastasectomy or SBRT.
The KEYNOTE-564 study included assessed adjuvant pembrolizumab in patients with intermediate or high-risk of recurrence after surgical treatment. Inclusion criteria for this study were:
- RCC with clear cell component
- Intermediate/high or high risk of recurrence
- pT2 with grade 4 / sarcomatoid
- pT3/4 with any grade
- Nodal positive (N1)
- M1 with No Evidence of Disease (NED) after complete resection of oligometastases synchronously or within 1 year of nephrectomy
The KEYNOTE-564 trial demonstrated a significant improvement in disease-free survival and overall survival in patients who received adjuvant treatment as shown below. There was a signal of improved benefit in patients with M1, NED.
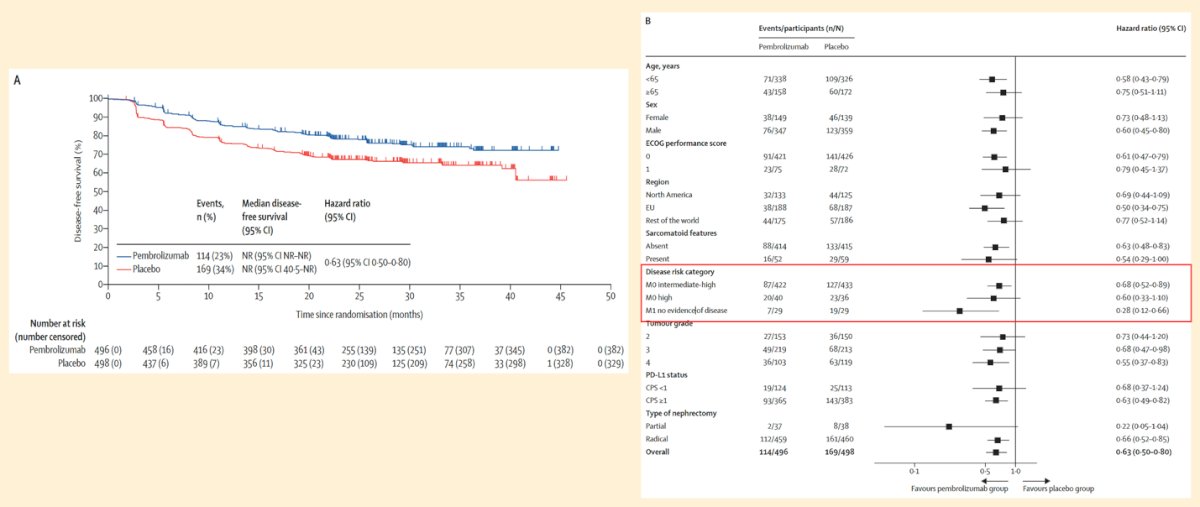
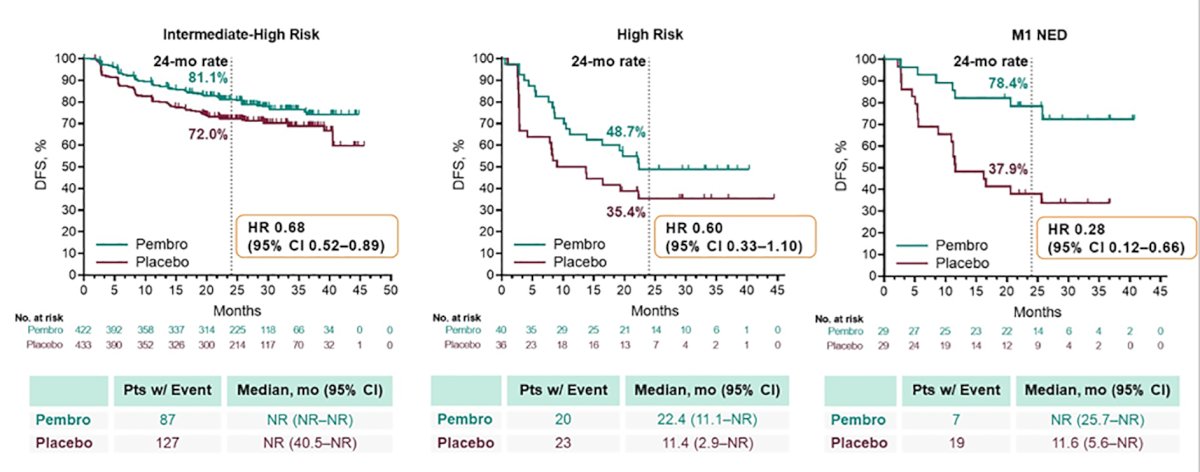
Notably, patients with M1 NED derived the greatest benefit from adjuvant pembrolizumab, as in the Kaplan-Meier graphics below, with a 72% reduction in the risk of disease recurrence (HR 0.28, 95% CI 0.12-0.66).1
A systematic review evaluating the role of complete surgical metastasectomy showed that incomplete metastasectomy was associated with worse overall survival, all studies included favoring complete resection. This finding was also confirmed in multivariate analysis and two rounds of sensitivity analyses, as illustrated below.2

Several studies have evaluated the role of metastasectomy and radiotherapy in RCC patients with bone metastases. Zelefsky et al. found that image-guided IMRT and hypofractionated regimens achieved a 3-year local PFS of 44%, with single-dose IGRT >24 Gy associated with better outcomes.3 Fuchs et al. reported higher survival rates in patients undergoing metastasectomy or curettage for solitary RCC bone metastases (3-year: 60% vs. 27%; 5-year: 36% vs. 8%).4 Hunter et al. compared SBRT vs. CRT for spine metastases, showing similar overall pain response rates (62% vs. 68%) and no significant differences in time-to-pain relief or its duration.5
The role of local therapy for brain metastasisDr. Teoh highlighted two studies evaluating metastasectomy and radiotherapy in RCC patients with brain metastases. Fokas et al. compared stereotactic radiosurgery (SRS), whole-brain radiotherapy (WBRT), and their combination, reporting median overall survival (OS) of 12, 2, and 16 months, respectively, with WBRT improving intracerebral control but not OS. Similarly, Ikushima et al. evaluated fractionated stereotactic radiotherapy (FSRT), surgery followed by conventional radiotherapy (S-CRT), and CRT alone, finding that FSRT provided superior tumor control and prolonged survival (median OS: 25.6, 18.7, and 4.3 months, respectively).6
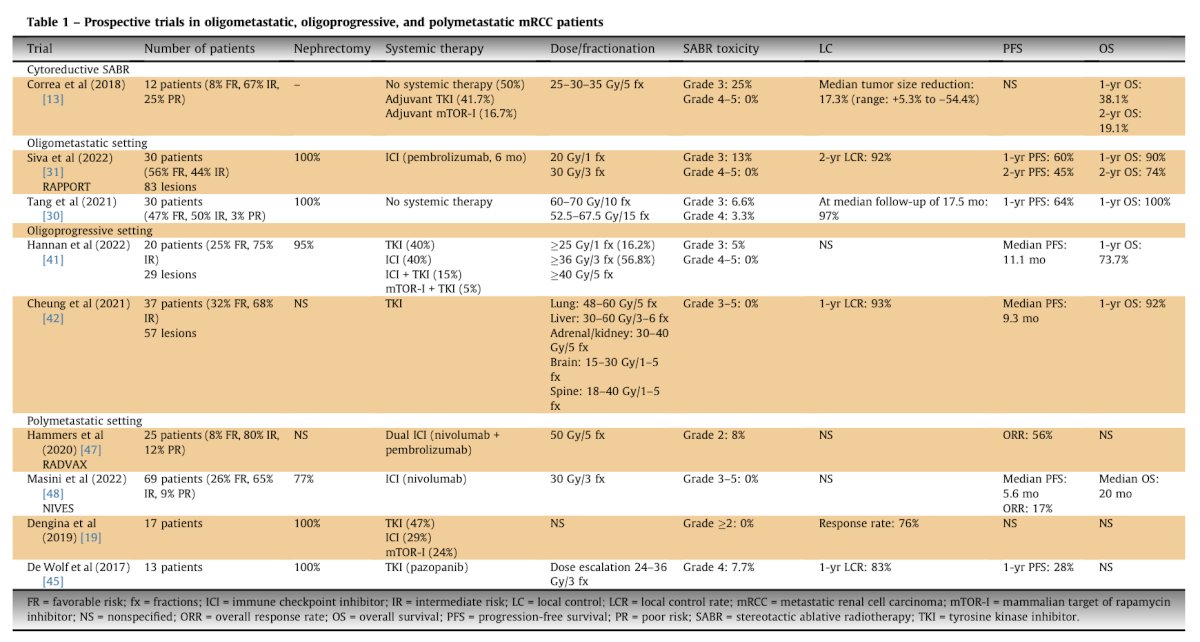
The emerging role of cytoreductive stereotactic body radiotherapy (SABR)A systematic review of nine prospective studies evaluated the role of extracranial stereotactic ablative radiotherapy (SABR) in metastatic RCC. The findings indicated that SABR effectively eradicated the entire metastatic burden in both synchronous and metachronous oligometastatic patients, achieving a long-term local control rate of over 90%. Additionally, treating oligoprogressive lesions with SABR extended the duration of systemic therapy by approximately nine months.7
Dr. Teoh concluded by presenting an algorithm illustrating the role of SABR in the oligoprogressive setting, emphasizing the existing knowledge gap in this area. He noted that SABR to all oligoprogressive sites aims to enhance local control, prolong progression-free survival (PFS) and overall survival (OS), and delay the transition from first- to second-line systemic therapy. While further research is needed, SABR should be considered for select patients.

Dr. Teoh concluded his presentation with the following key takeaways:
- Achieving an ‘NED status’ appears to be beneficial in patients with oligometastatic RCC
- There is some evidence showing the benefit of metastasis-directed therapy in patients with oligoprogression after first-line systemic therapy
- Switching to another systemic therapy does not necessarily mean a better outcome
- Metastasis-directed therapy should be offered in highly selected patients
- We must balance between the potential benefits and risks of local therapy in oligometastatic/oligoprogressive RCC
Presented by: Jeremy Yuen-Chun Teoh, MD, Urology Centre, Department of Surgery, Faculty of Medicine, Chinese University of Hong Kong, Hong Kong, China
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:- Choueiri TK, Tomczak P, Park SH, Venugopal B, Ferguson T, Symeonides SN, Hajek J, Chang YH, Lee JL, Sarwar N, Haas NB, Gurney H, Sawrycki P, Mahave M, Gross-Goupil M, Zhang T, Burke JM, Doshi G, Melichar B, Kopyltsov E, Alva A, Oudard S, Topart D, Hammers H, Kitamura H, McDermott DF, Silva A, Winquist E, Cornell J, Elfiky A, Burgents JE, Perini RF, Powles T; KEYNOTE-564 Investigators. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med. 2024 Apr 18;390(15):1359-1371. doi: 10.1056/NEJMoa2312695. PMID: 38631003.
- Zaid HB, Parker WP, Safdar NS, Gershman B, Erwin PJ, Murad MH, Boorjian SA, Costello BA, Thompson RH, Leibovich BC. Outcomes Following Complete Surgical Metastasectomy for Patients with Metastatic Renal Cell Carcinoma: A Systematic Review and Meta-Analysis. J Urol. 2017 Jan;197(1):44-49. doi: 10.1016/j.juro.2016.07.079. Epub 2016 Jul 26. PMID: 27473875.
- Zelefsky MJ, Greco C, Motzer R, Magsanoc JM, Pei X, Lovelock M, Mechalakos J, Zatcky J, Fuks Z, Yamada Y. Tumor control outcomes after hypofractionated and single-dose stereotactic image-guided intensity-modulated radiotherapy for extracranial metastases from renal cell carcinoma. Int J Radiat Oncol Biol Phys. 2012 Apr 1;82(5):1744-8. doi: 10.1016/j.ijrobp.2011.02.040. Epub 2011 May 17. PMID: 21596489; PMCID: PMC4034682.
- Fuchs B, Trousdale RT, Rock MG. Solitary bony metastasis from renal cell carcinoma: significance of surgical treatment. Clin Orthop Relat Res. 2005 Feb;(431):187-92. doi: 10.1097/01.blo.0000149820.65137.b4. PMID: 15685074.
- Hunter GK, Balagamwala EH, Koyfman SA, Bledsoe T, Sheplan LJ, Reddy CA, Chao ST, Djemil T, Angelov L, Videtic GMM. The efficacy of external beam radiotherapy and stereotactic body radiotherapy for painful spinal metastases from renal cell carcinoma. Pract Radiat Oncol. 2012 Oct-Dec;2(4):e95-e100. doi: 10.1016/j.prro.2012.01.005. Epub 2012 Feb 15. PMID: 24674192.
- Ikushima H, Tokuuye K, Sumi M, Kagami Y, Murayama S, Ikeda H, Tanaka M, Oyama H, Shibui S, Nomura K. Fractionated stereotactic radiotherapy of brain metastases from renal cell carcinoma. Int J Radiat Oncol Biol Phys. 2000 Dec 1;48(5):1389-93. doi: 10.1016/s0360-3016(00)00804-x. PMID: 11121638.
- Le Guevelou J, Sargos P, Siva S, Ploussard G, Ost P, Gillessen S, Zilli T. The Emerging Role of Extracranial Stereotactic Ablative Radiotherapy for Metastatic Renal Cell Carcinoma: A Systematic Review. Eur Urol Focus. 2023 Jan;9(1):114-124. doi: 10.1016/j.euf.2022.08.016. Epub 2022 Sep 20. PMID: 36151031.