(UroToday.com) The 2025 EAU annual meeting featured a non muscle invasive bladder cancer session and a presentation by Dr. Trinity Bivalacqua discussing updated clinical and translational results from BOND-003 cohort C, a phase 3, single-arm study of intravesical cretostimogene grenadenorepvec for high-risk BCG-unresponsive non muscle invasive bladder cancer with CIS. There is a significant unmet need for clinically effective and well-tolerated bladder-sparing treatments in these high risk patients. Cretostimogene grenadenorepvec is an oncolytic immunotherapy with a dual mechanism of action. It selectively replicates in and lyses cancer cells with Rb-E2F pathway alterations, which releases virus- and tumor-specific antigens, triggering antitumor immune activation, potentiated by the GM-CSF transgene:

Cretostimogene previously received US FDA Fast Track and Breakthrough Therapy Designations. BOND-003 (NCT044552591) is a phase-3 study that evaluates the efficacy and safety of cretostimogene in patients with high-risk BCG-unresponsive non muscle invasive bladder cancer. At the EAU 2025 annual meeting, Dr. Bivalacqua presented updated results from BOND-003 cohort C.
A total of 112 adults with histologically confirmed high-risk BCG-unresponsive non muscle invasive bladder cancer with CIS were enrolled in cohort C. Patients received prior adequate BCG and were considered BCG-unresponsive per US FDA guidance. Cretostimogene was administered in 6 weekly doses during the induction phase, followed by maintenance therapy. Patients with persistent HG Ta or CIS at month 3 were eligible for re-induction. Response assessments included serial cystoscopy, urine cytology, axial imaging, and mandatory biopsy at month 12, with centralized pathology review. The primary outcome measure was complete response at any time, and secondary endpoints included duration of response, recurrence-free survival, progression-free survival, cystectomy-free survival, safety, and tolerability:

Among the 112 patients enrolled in BOND-003 cohort C, 74.1% were male, the median age was 74.0 (range: 43-90) years, the median number of prior BCG instillations was 12 (range: 7-66), and the majority of patients (80.4%) had CIS only disease:

As of the January 20, 2025 data cutoff, the complete response rate at any time in BOND-003 cohort C was 75.5% (83/110) (95% CI 66.3-83.2%). The 12 month landmark complete response rate was 46% (95% CI 36.9 – 56.1), with 30 patients having confirmed complete responses that have reached the 24 month time point and beyond:
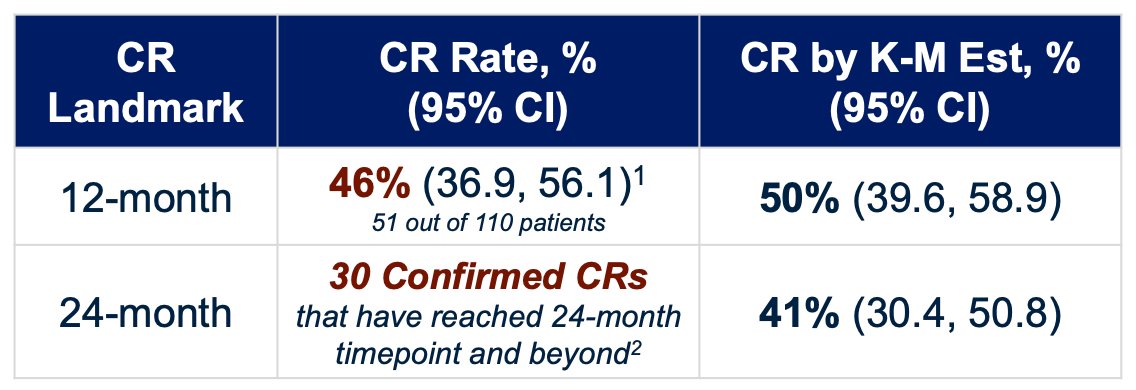
Furthermore, the freedom from progression to muscle invasive bladder cancer at 12 months was 97.3% and the cystectomy free survival rate at 12 months was 90.0%. The complete response rate was consistent across patient subgroups and all complete responses were centrally confirmed. Cretostimogene demonstrated sustained and ongoing duration of response in this disease space: over a median follow-up of 22.3 months, the 12 month estimated duration of response probability was 63.7% (95% CI 51.8-73.3) and was 58.7% at 24 months. The median duration of response exceeds 28 months, suggesting innate to adaptive switching with immunogenic memory and a long IO tail:

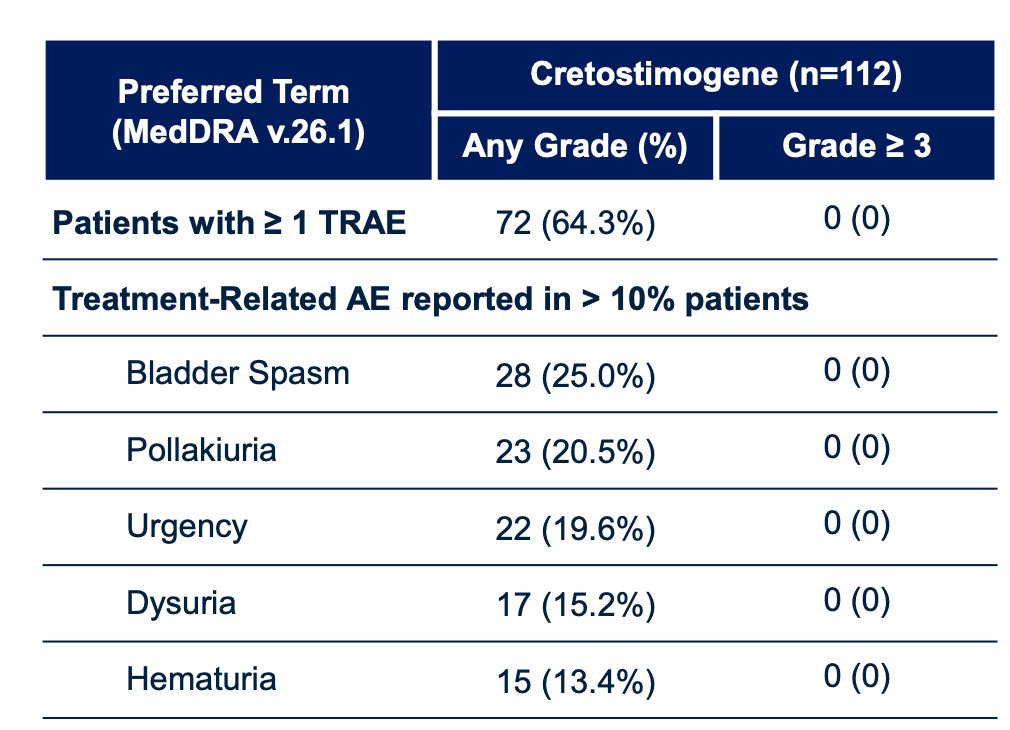
Cretostimogene was associated with a favorable and well tolerated safety profile, with most adverse events being grade 1-2 and no grade 3+ adverse events or death. Additionally, the median time to treatment related adverse event resolution was 1 day, there were no treatment related discontinuations, and 97.3% of patients completed all protocol defined treatments. Only 2 patients (1.8%) had serious treatment related adverse events (grade 2):
From a translational standpoint, at induction, cretostimogene replication and GM-CSF expression are linked, and levels peak immediate after instillation, and are sustained locally for 4-5 days, offering an effective payload delivery. This reinforces observations from V-0046/phase 1 data:
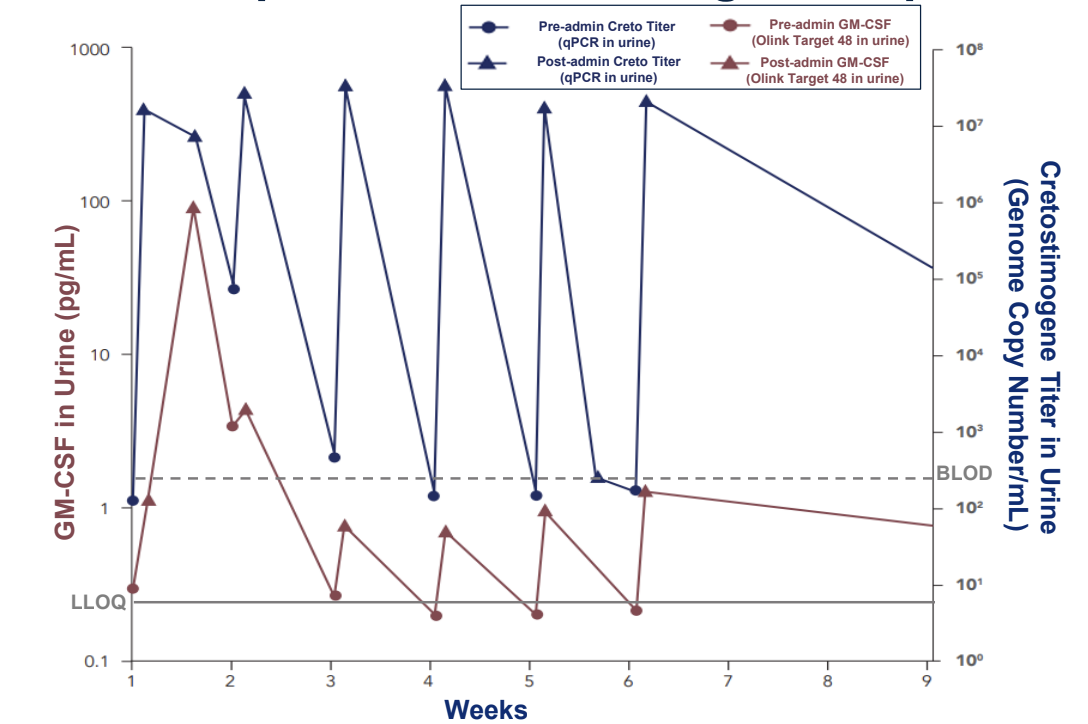
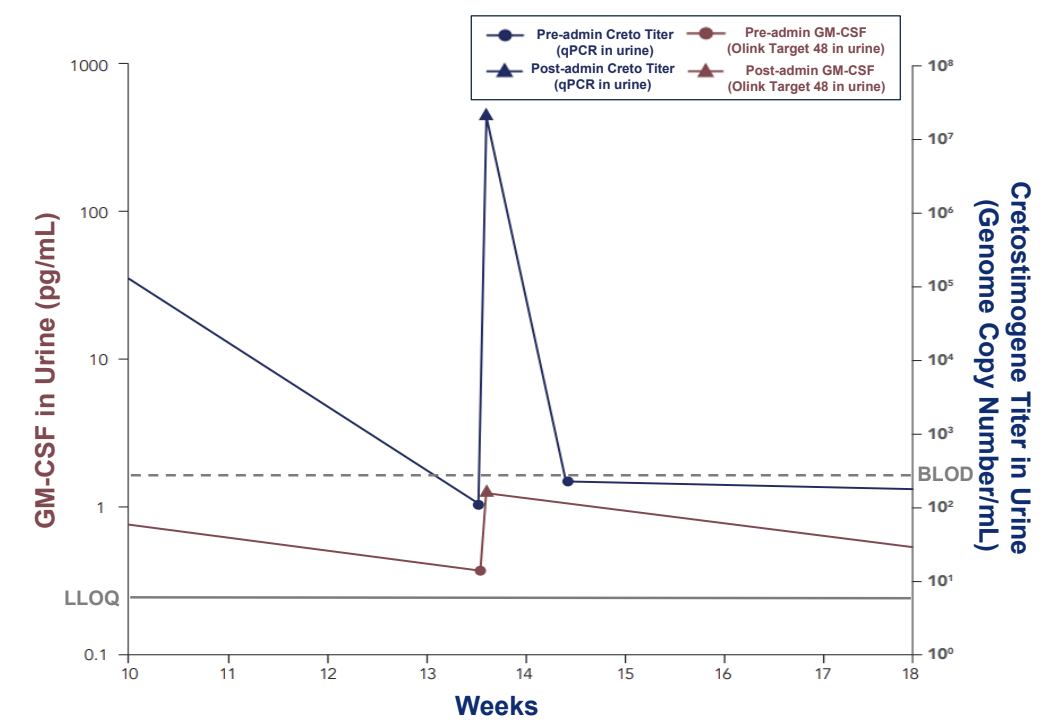
During the maintenance phase, there is a similar pharmacokinetic peak and trough pattern that mirrors replication kinetics, with titers present throughout the maintenance phase. This supports an oncolytic mechanism of action:
Additionally, cretostimogene shows robust and stable immune activity, with pre-existing Ad5 antibodies, allowing immune priming, and stable antibody and anti-tumor response over time. Antibody response also correlates with clinical outcomes and intravesical delivery reduces ADA neutralization, preserving therapeutic efficacy:

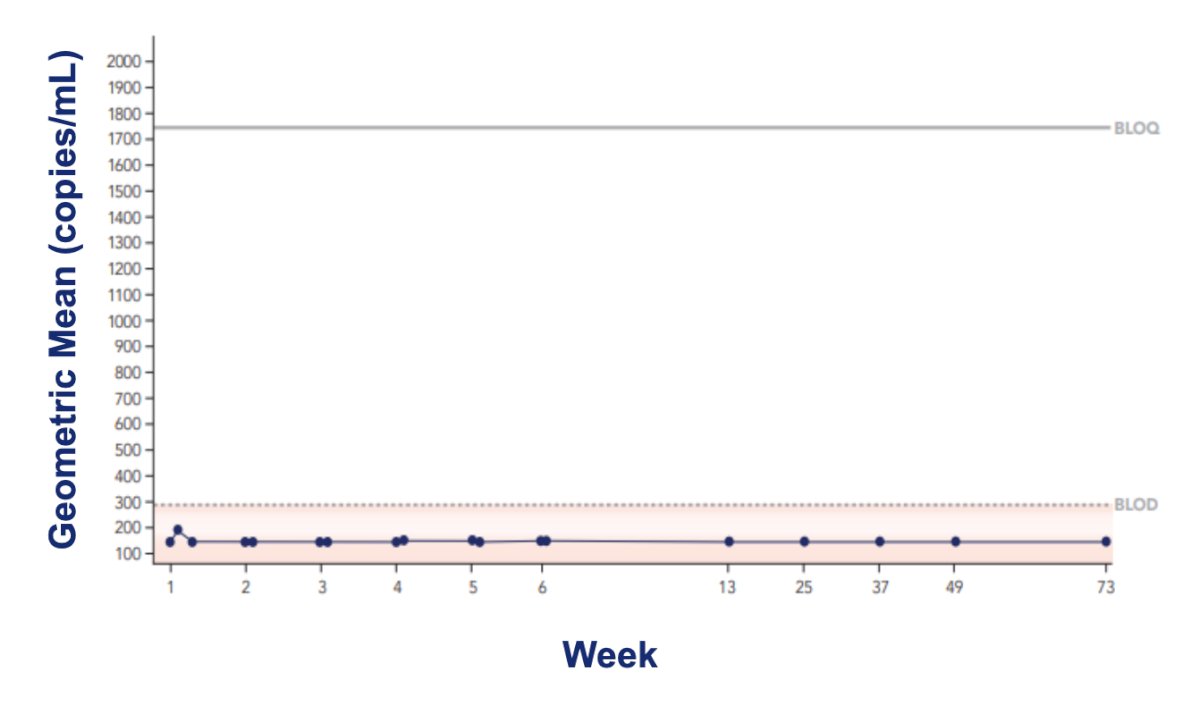
Finally, there was no systemic exposure, and cretostimogene levels remained below the limit of detection, concentrated in the bladder, even with repeat dosing:
Dr. Bivalacqua concluded his presentation by discussing updated clinical and translational results from BOND-003 cohort C with the following take home points:
- Cretostimogene is an oncolytic immunotherapy with a dual mechanism of action
- It is highly effective and a very well tolerated regimen
- Translational analyses validate sustained local activity, dose, treatment schedule, and legacy data
- There are no post-cretostimogene close contact precautions
- The final BOND-003 cohort C results will be presented at AUA 2025
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025