(UroToday.com) The 2025 EAU annual meeting featured a session on intravesical therapy for bladder cancer and a presentation by Dr. Yohann Loriot discussing that combination systemic and intravesical therapy is the ideal duo for treatment of high risk non muscle invasive bladder cancer. Dr. Loriot started his presentation by emphasizing that BCG-induced innate and adaptive immune responses can be modulated by systemic therapies. With regards to mechanisms of resistance to BCG, PDL1 expression is associated with BCG resistance in 25% of patients, and CD8 and PDL1 co-localize resulting in adaptive immune resistance.
Why not give immune checkpoint inhibitors intravesically? This was first reported in 2022 by Meghani et al.1 who assessed the first-in-human intravesical delivery of pembrolizumab, identifying immune activation in BCG unresponsive non muscle invasive bladder cancer. Specifically, they showed progressive remodeling of local immune contents over the course of treatment by urine analysis of immune cells and cytokines. Grade 3-4 toxicity of intravesical pembrolizumab was lower than that of intravenous pembrolizumab, but one patient died from pembrolizumab adverse events. All patients recurred, with a recurrence free survival rate at 3, 6, and 12 months of 100%, 67%, and 22%, respectively. Notably, progression to locally advanced cancer occurred in 4/9 patients, with recurrence in 6/9 patients outside of the treated bladder to upper tract urothelial carcinoma (n = 2), lung (n = 1), prostate (n = 2), and pelvis (n = 1).
The clinical rationale for this combination approach is that progression to muscle invasive bladder cancer or occurrence of metastases are rare at the time of relapses treated with BCG, however the natural history of BCG-refractory disease is often progression to muscle invasive bladder cancer, metastases or death. Dr. Loriot then discussed the KEYNOTE-057 trial,2 which is an open-label, single-arm, multicenter, phase II trial consisting of two adult patient cohorts:
- Cohort A: BCG-unresponsive CIS +/- papillary tumors
- Cohort B: BCG-unresponsive high-grade Ta or any grade T1 papillary tumors (no CIS)
The trial design for KEYNOTE-057 is as follows: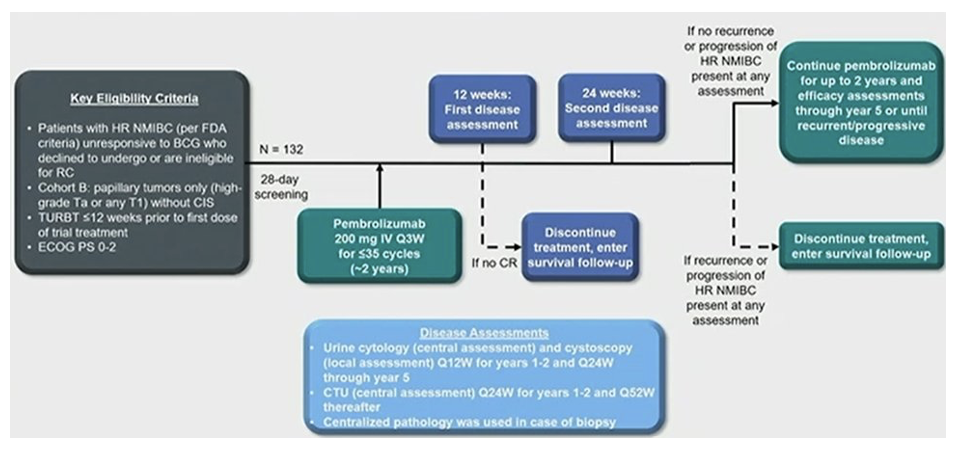
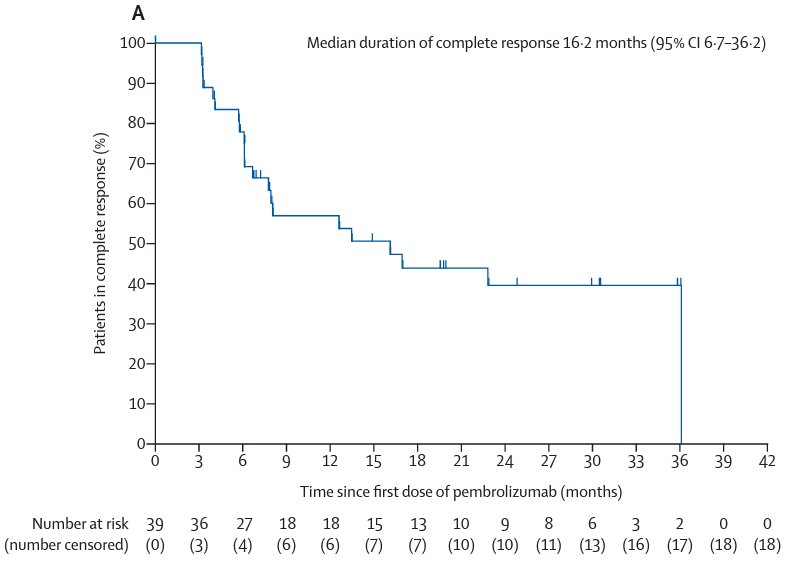
Patients in this trial received intravenous pembrolizumab, an anti-PD-1 agent, at 200 mg every 3 weeks for up to 24 months or until patients had evidence of centrally-confirmed disease persistence, recurrence, or progression or unacceptable drug-related toxicity. The 36-month follow-up outcomes of the 101 patients in Cohort A showed that the 3-month complete response rate, defined as absence of high-risk non muscle invasive bladder cancer or progressive disease, was 41%:
Systemic immunotherapy has some local activity in BCG-refractory papillary tumors. The SWOG S1605 trial [3] showed that among 74 patients with CIS +/- Ta/T1, atezolizumab lead to a complete response rate of 42% at 3 months, 24% at 12 months, and a grade 3+ adverse event rate of 13%. Presented at ASCO GU 2024, BladderGATE assessed atezolizumab + intravesical BCG combination in patients with high risk non muscle invasive bladder cancer. In this phase 1b/2 open label clinical trial, patients were scheduled to receive atezolizumab 1,200 mg IV on day 1 of each 21-day cycle (maximum of 52 weeks) plus BCG weekly x 6 weeks induction followed by maintenance at weeks 12, 24, and 48:

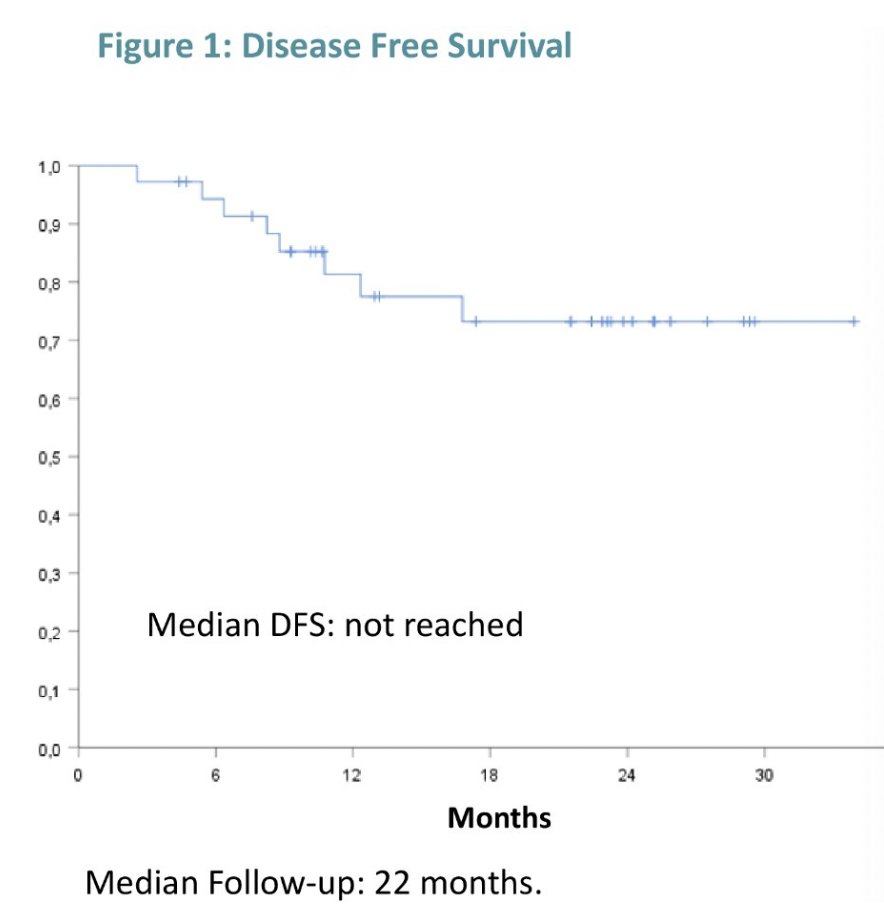
In this trial, 56% of patients completed all BCG instillation, with 89% overall considered to have received ‘adequate’ BCG per the FDA guidance. Atezolizumab treatment was completed by 61% of patients, with a median of 14.5 doses. The main reason for atezolizumab non-compliance was immune-related adverse events, with grade ≥3 such events occurring in 19.4% of patients: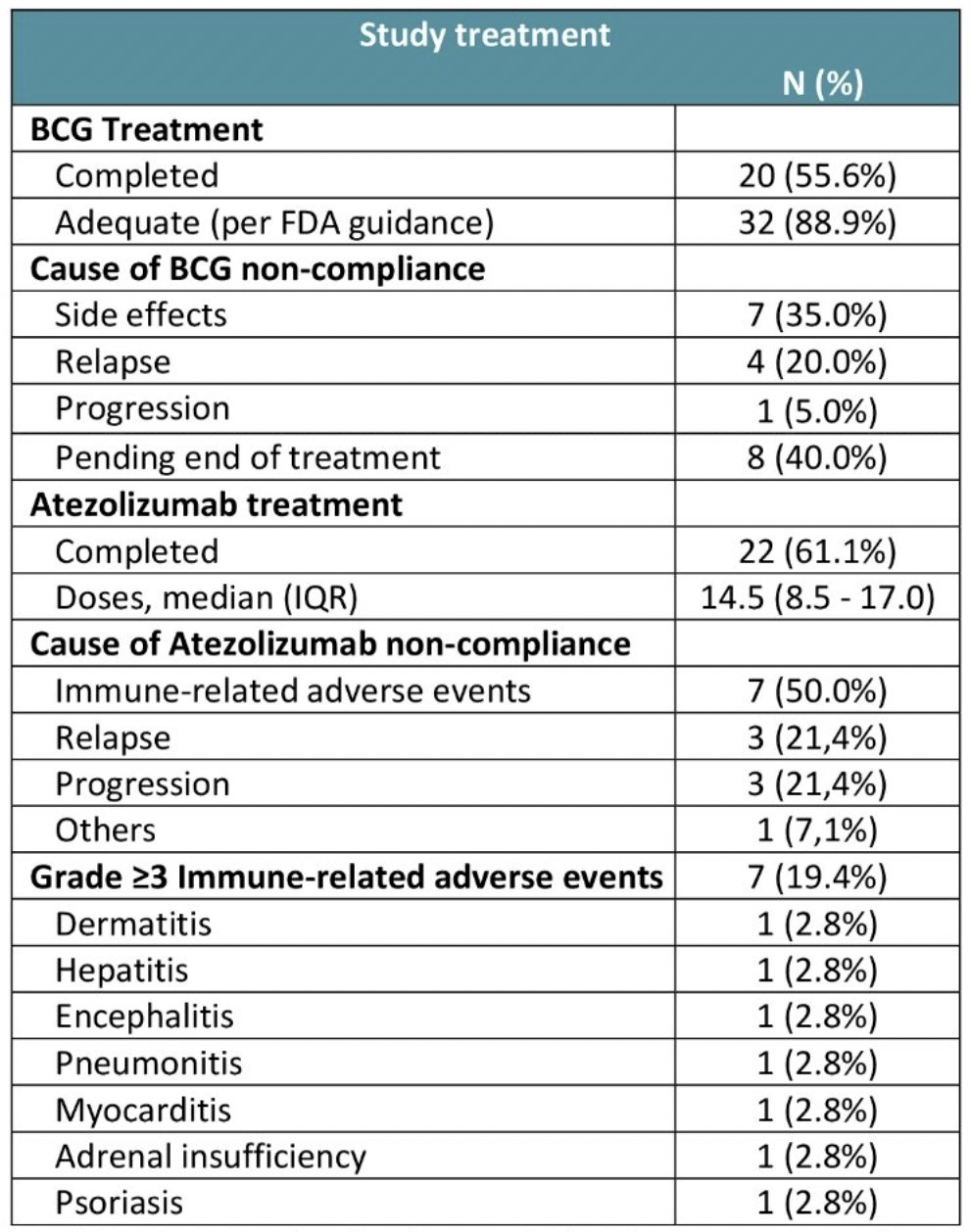
With regards to efficacy outcomes, local recurrence occurred in 17% of patients (13.9% high grade), with a 2-year high-grade disease-free survival of 73%. Three (8%) patients progressed to muscle invasiveness: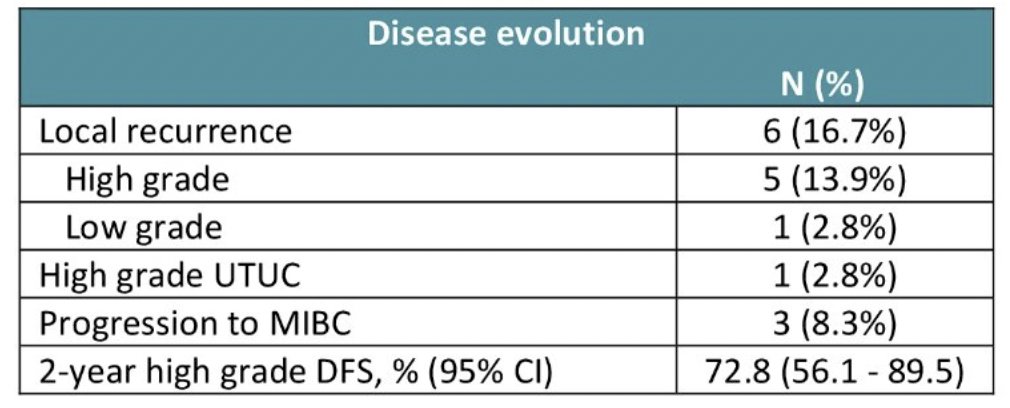
The duos currently being investigated include:
- IV PD(L)1 + BCG
- CREST phase 3 trial
- ALBAN phase 3 trial
- POTOMAC phase 3 trial
- KEYNOTE-676 phase 3 trial
- IV PD(L)1 + TAR-200
- SunRISe-1 phase 2b trial
- SunRISe-3 phase 3 trial
Dr. Loriot notes that the SunRISe-1 trial taught us that not all duos are additive or synergistic and that TAR-200 is enough. In the TAR-200 monotherapy arm of this trial, the anytime complete response rate was 83.5%. The ongoing SunRISe-3 trial is assessing TAR-200 + cetrelimab versus TAR-200 monotherapy versus BCG: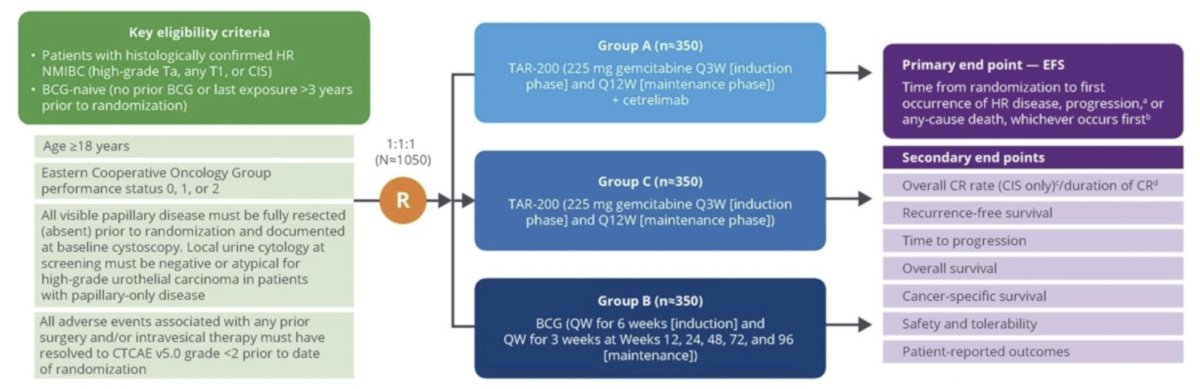
Determining the mechanisms of action is critical. For example, FGFR mutations allow specific FGFR inhibitors in early stage bladder cancer, which is being assessed in the MoonRISE program. This is an open label, multicenter, phase 1 trial that aims to evaluate the safety, pharmacokinetics, and efficacy of TAR-210. This study included 2 cohorts:
- Cohort 1: High-risk non muscle invasive bladder cancer (HG Ta/T1, no CIS, papillary only), BCG-experienced/unresponsive, and not undergoing radical cystectomy. All patients in this cohort had a TURBT with complete resection of all visible disease prior to treatment
- Cohort 3: Intermediate-risk non muscle invasive bladder cancer (LG Ta/T1 disease) and visible target lesions prior to treatment (chemoablation design)
Part 1 was a dose escalation phase with two different erdafitinib release rates being evaluated. Part 2 was the dose expansion phase for patients in Cohorts 1 and 3. Response was assessed every 3 months with continued treatment for up to 1 year if recurrence-free (Cohort 1) or until complete response (Cohort 3). Of note, the first response assessment was at 3 months:

For patients in Cohort 1 (n=16), the median age was 73.5 years, 75% were male, 75% and 25% had tumor stage Ta and T1, respectively, 44% had multiple tumors, and 100% had prior BCG. In 11 patients with an available response assessment, 9 (82%) were recurrence-free. The median recurrence-free survival has not been reached yet (95% CI: 2.96 months – not reached). The median duration of treatment exposure was 3.7 – 4.3 months: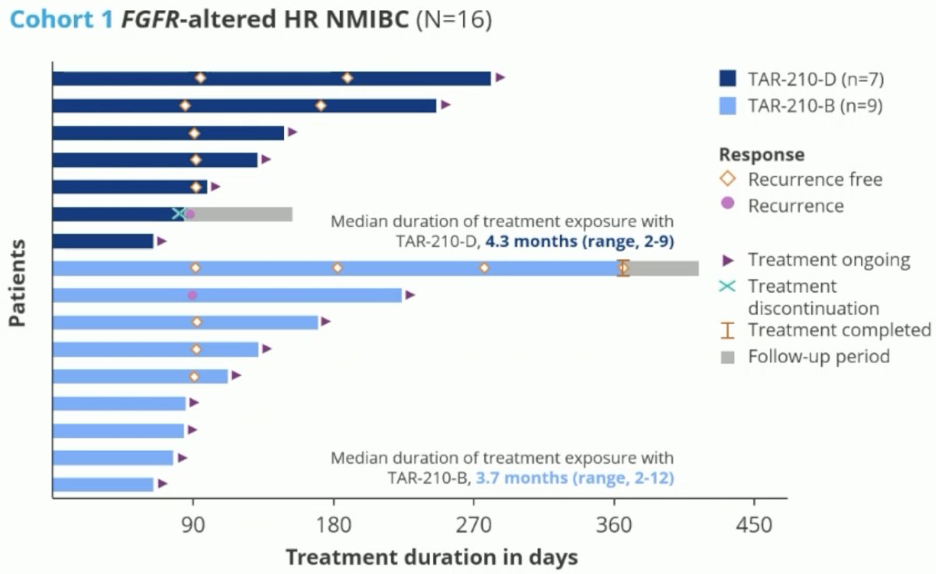 In the chemoablative Cohort 3 (n=27), the median age was 67 years, 85% were male, 100% had tumor stage Ta, 41% had multiple tumors, 59% had prior intravesical therapy, and 22% had prior BCG. In 15 patients with available response assessment, 13 (87%) achieved a complete response. All complete responses were ongoing as of data collection cut-off (median duration of response not reached yet). The median duration of treatment exposure was 3.3 – 4.2 months:
In the chemoablative Cohort 3 (n=27), the median age was 67 years, 85% were male, 100% had tumor stage Ta, 41% had multiple tumors, 59% had prior intravesical therapy, and 22% had prior BCG. In 15 patients with available response assessment, 13 (87%) achieved a complete response. All complete responses were ongoing as of data collection cut-off (median duration of response not reached yet). The median duration of treatment exposure was 3.3 – 4.2 months:
Regarding other duos currently being investigated, for those receiving IV PD(L)1 + an antibody drug conjugate or IV PD(L)1 + virus/gene therapy, there are the following combinations:
- Enfortumab vedotin (anti-nectin 4) in EV-104
- Sac-TMT (anti-Trop 2) in Trofuse-027
- Disitamab vedotin (anti-HER2) in RC48-C029
- Cretostimogene grenadenorepvec + pembrolizumab in CORE-001
- Nadofaragene firadenovec + pembrolizumab in ABLE-22
Presented initially at ASCO 2023, EV-104 trial is an ongoing phase 1, open-label, multicenter, dose-escalation and expansion study of intravesical enfortumab vedotin evaluating the safety, tolerability, pharmacokinetic, and antitumor activity of intravesical enfortumab vedotin in patients with high-risk BCG-unresponsive non muscle invasive bladder cancer with CIS with or without papillary disease who are ineligible for or refuse radical cystectomy. The trial design for EV-104 is as follows: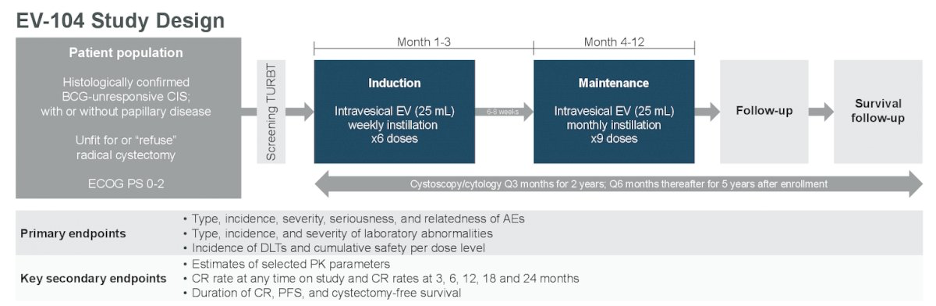
As of data cutoff, no dose limiting toxicities were observed for either 125 mg or 250mg. All blood PK analyses (ADC and unconjugated MMAE) for patients at 125mg were undetectable; no PK data was available for 250 mg. Of 4 patients receiving 125 mg of intravesical enfortumab vedotin, 3 achieved complete response and continue in response. The fourth patient discontinued treatment due to persistent disease but remains on study:
Dr. Loriot concluded his presentation discussing that combination systemic and intravesical therapy is the ideal duo for treatment of high risk non muscle invasive bladder cancer with the following take home points:
- There is strong rationale for the combination of systemic and intravesical therapy
- Not all IV and intravesical combinations will work, thus determining the mechanism of action is key
- The safety profile is critical in this population of patients
- BCG + PD(L)1 may be the first available duo in the coming months/years
- Strong collaboration between medical oncologists and urologists will be critical, especially for managing the toxicities
Presented by: Yohann Loriot, MD, PhD Institut Gustave Roussy, Universite Paris-Saclay, Villejuif, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:
- Meghani K, Cooley LF, Choy B, et al. First-in-human intravesical delivery of pembrolizumab identifies immune activation in bladder cancer unresponsive to Bacillus Calmette-Guerin. Eur Urol. 2022 Dec;82(6):602-610.
- Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): An open-label, single-arm, multicenter, phase 2 study. Lancet Oncol. 2021 Jul;22(7):919-930.
- Black PC, Tangen CM, Singh P, et al. Phase 2 trial of Atezolizumab in Bacillus Calmette-Guerin-unresponsive high risk non-muscle-invasive bladder cancer: SWOG S1605. Eur Urol. 2023 Dec;84(6):536-544.