(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th 2025, was host to an EAU lab abstract session. Dr. Alexander Wyatt delivered a state-of-the-art lecture on the use of ctDNA testing for guiding treatment decision-making in genitourinary cancers.
He began by noting that currently available ctDNA tests are different in nature, which reflects differences in the clinical questions that ctDNA tests have been designed to address:
The ctDNA test choice must match the clinical question:
There are two broad categories of ctDNA: tumor-informed and tumor-naïve, as outlined below:
What do we already know about ctDNA in urologic malignancies? Correlative studies suggest that ctDNA positivity is associated with urothelial carcinoma recurrences, progression, and prognoses. The use of ctDNA offers opportunities for intervention:
- ctDNA negative de-escalation of treatment; bladder sparing
- ctDNA positive earlier treatment or treatment change
What are the current limitations of ctDNA in urologic malignancies?
- Prospective evaluation of its utility remains limited
- There are few comparisons of ctDNA test sensitivity
- It is unclear how we can operationalize ctDNA in the real world
Dr. Wyatt presented the key takeaways from three abstracts presented during this session. Starting off with ‘ctDNA positivity predicts shorter disease-specific survival for G3pT1 urothelial bladder carcinoma patients’, he noted that this study evaluated a new paradigm: urine-informed plasma ctDNA detection. This may be particularly significant for upper tract tumors given the challenges with obtaining adequate tissue in a number of such patients. The study investigators applied this test to 95 patients with T1G3 bladder cancer. Notably, serum ctDNA-negative patients had superior disease-specific and progression-free survivals. Dr. Wyatt noted that this creates a novel class of NMIBC patients, ctDNA+ T1G3 patients with poor outcomes, who may benefit from early treatment escalation.
Next, Dr. Wyatt summarized the results of the TOMOBOLA trial, presented by Dr. Dyrskjøt. TOMBOLA was a national, non-randomized ctDNA-based intervention study conducted at 5 centers in Denmark. Eligible patients were those with cT2-4aN0-1M0, cisplatin, and immunotherapy-eligible MIBC who received neoadjuvant chemotherapy followed by radical cystectomy. Patients underwent serial ctDNA testing post-operatively. Upon ctDNA detection, patients were recommended for one year of atezolizumab therapy.
The patient characteristics are summarized below, with 39% and 61% of patients having clinical high- and low-risk disease, respectively. Notably, among the clinical high-risk patients, 65% had a positive ctDNA status post-radical cystectomy. Conversely, almost half (49%) of the ‘low risk’ patients were also ctDNA+ post operatively. 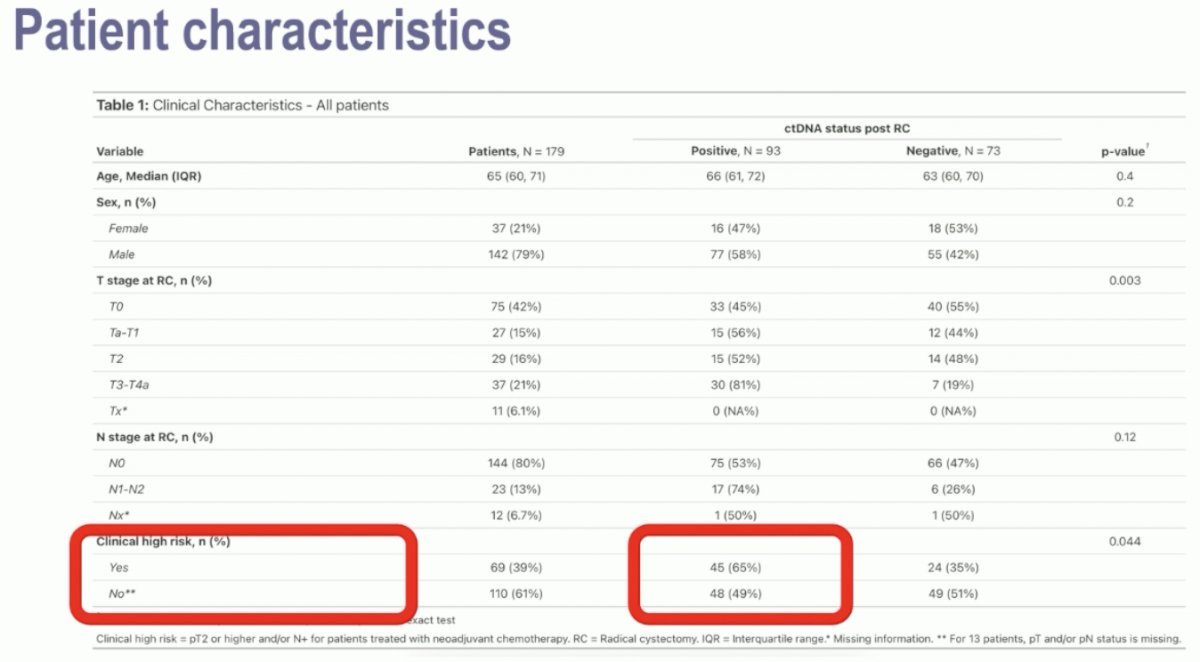
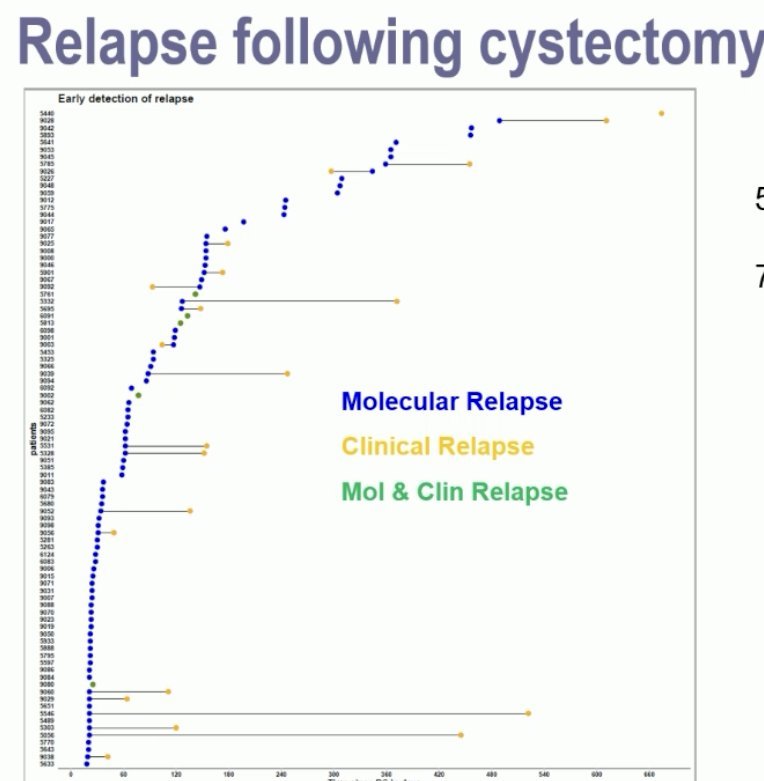
56% of patients were ctDNA+ post-radical cystectomy. 75% were detected <4 months post-cystectomy. Of the ctDNA- patients, only 2 (3%) developed metastases on CT scan during follow-up.
In the ctDNA- patients, both recurrence-free and overall survivals were excellent, as demonstrated in the Kaplan-Meier curves below: 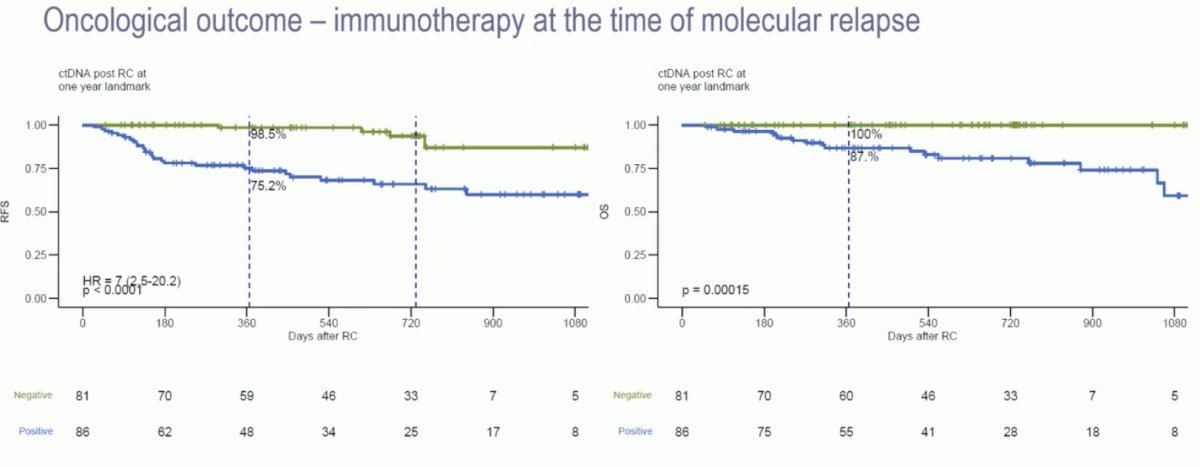
With regards to the primary endpoint, 55% of the 44 patients with a ctDNA+ status converted to ctDNA- with no evidence of disease on CT scanning. 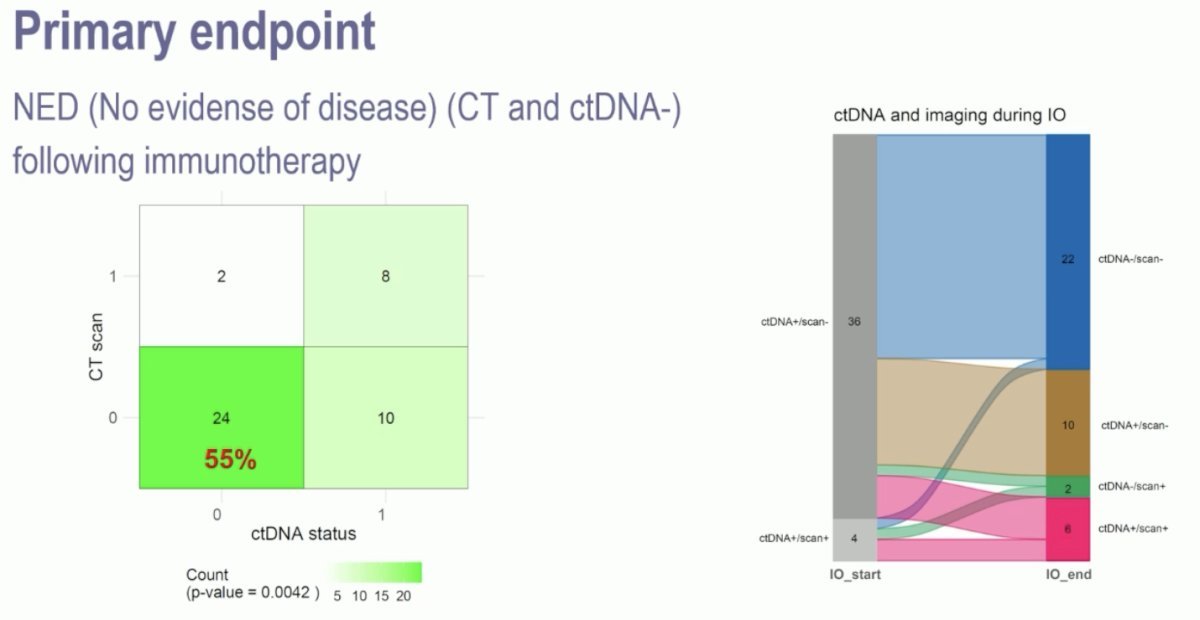
Finally, Dr. Wyatt addressed the abstract presentation by Dr. Nordentoft: “Comparison of ctDNA detection methods for monitoring minimal residual disease in patients with bladder cancer: Insights from the TOMBOLA trial”. This study directly compared two different tumour-informed methods:
- Labour-heavy (droplet digital PCR [ddPCR]) versus computer-heavy (whole genome sequencing [WGS])
- Speed and cost were higher with WGS
The WGS-based method had reduced sensitivity for low tumour fractions. Dr. Wyatt hypothesized whether the sensitivity could be improved with higher input (i.e., more cell-free DNA)? Conversely, the WGS-based method had higher specificity for predicting recurrences. Will longer follow-up clarify ddPCR specificity?
Dr. Wyatt concluded as follows:
- Plasma ctDNA positive versus negative status is poised to influence patient management in NMIBC & MIBC
- Is de-escalation in ctDNA negative patients the easiest path forward?
- Several types of tumour-informed tests are applicable:
- What tumour analyte do we use (urine vs. tissue)?
- Where do we personalize (wet-lab design vs. bioinformatics)?
- What are the resource implications (labor vs. compute, cost)?
- We must consider who will operate the tests (e.g. hospital pathology labs)
Presented by: Alexander Wyatt, B.SC., D.Phil., Associate Professor, Department of Urologic Sciences, Vancouver Prostate Centre, University of British Columbia, Vancouver, BC, Canada
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th, 2025