(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain was host to the Biomarkers to guide peri-operative management in Uro-oncology Plenary Session. Dr. Kent Mouw discussed Bladder-sparing strategies: DNA damage response (DDR) genes and liquid biopsies
Currently, two curative-intent treatment strategies are supported by available data: radical cystectomy (RC) and trimodal therapy (TMT). However, these approaches have never been successfully compared in a randomized trial. Validated predictive biomarkers could help guide therapy selection, determining whether RC, TMT, or other bladder-sparing approaches are the most appropriate for individual patients.

DDR gene alterations have been identified in certain cohorts of muscle-invasive bladder cancer (MIBC), with studies showing promising responses, particularly in ERCC2-mutated cases and broader gene panels. The data from these studies are summarized below. A key question remains: can DDR gene alteration status be used to identify select MIBC patients who may safely avoid definitive local therapy, such as radical cystectomy (RC) or trimodal therapy (TMT)?1

The first trial to address this question is the RETAIN-1 trial. Patients underwent an initial TURBT followed by next-generation sequencing and received three cycles of AMVAC. A re-TURBT was then performed, and based on residual tumor status, patients were assigned to one of several treatment pathways: active surveillance, intravesical therapy, chemoradiotherapy, or radical cystectomy. Notably, among the 25 patients who underwent active surveillance, 32% had no recurrence, and 47% of those who retained their bladder remained metastasis-free. Additionally, 16% ultimately underwent radical cystectomy with no evidence of disease, while 4% developed metastatic disease as their first recurrence event. Meanwhile, 32% experienced local recurrence that later progressed to metastasis.
The RETAIN-2 trial is currently underway to further evaluate this approach and refine selection criteria for bladder preservation strategies in MIBC.

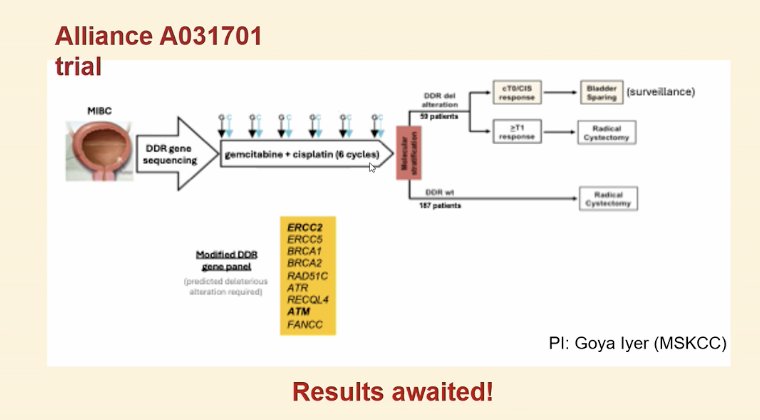
A second trial, run by the Alliance group (A031701), is currently evaluating DDR gene sequencing in MIBC. It is actively accruing patients, and results are expected in the coming years. The study is randomizing patients based on DDR gene status to either surveillance or cystectomy.
The HCRN 16-257 trial is similar to RETAIN-1 and the ALLIANCE trial but did not use DDR gene status for inclusion—any patient was eligible for surveillance. Among 76 participants, eight required cystectomy, and only two developed metastatic disease, unlike RETAIN-1, with one case occurring after cystectomy. Incorporating DDR gene alterations did not provide additional benefits.

Plasma circulating tumor DNA (ctDNA) dynamics have been associated with clinical outcomes in patients treated with TMT. Among those who remained ctDNA-positive post-TMT, 100% developed metastatic disease. In contrast, patients who converted to ctDNA-negative fared significantly better, with 17 out of 18 showing no evidence of metastatic or locally invasive disease. Notably, one patient who initially tested ctDNA-negative later converted post-TMT and subsequently developed metastatic disease.

Dr. Mouw concluded his presentation with the following take-home messages:
- DNA damage repair gene alterations are associated with high pCR rates and improved outcomes in some neoadjuvant chemotherapy followed by + cystectomy cohorts.
- The questions that remain to be answered are:
- Which genes? Which mutations?
- The role of DDR gene alteration status in guiding bladder preservation remains uncertain.
- DDR gene alterations alone are neither necessary nor sufficient to ensure good clinical outcomes.
- ctDNA dynamics appear to correlate with metastatic disease in TMT cohorts, raising the potential role of urine tumor DNA (utDNA) in assessing bladder disease status.
- The future direction is toward multimodal biomarker integration, combining ctDNA/utDNA, mpMRI, genomics (DNA/RNA), AI, and other advanced approaches
Presented by: Kent William Mouw, MD, PhD, Associate Professor of Radiation Oncology; Institution. Dana-Farber Cancer Institute, Boston, MA. United States.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:- Liu D, Plimack ER, Hoffman-Censits J, Garraway LA, Bellmunt J, Van Allen E, Rosenberg JE. Clinical Validation of Chemotherapy Response Biomarker ERCC2 in Muscle-Invasive Urothelial Bladder Carcinoma. JAMA Oncol. 2016 Aug 1;2(8):1094-6. doi: 10.1001/jamaoncol.2016.1056. PMID: 27310333; PMCID: PMC5515075.