(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain was host to the Biomarkers to guide peri-operative management in Uro-oncology Plenary Session. Dr. John Sfakianos discussed the role of ctDNA in treatment de-escalation
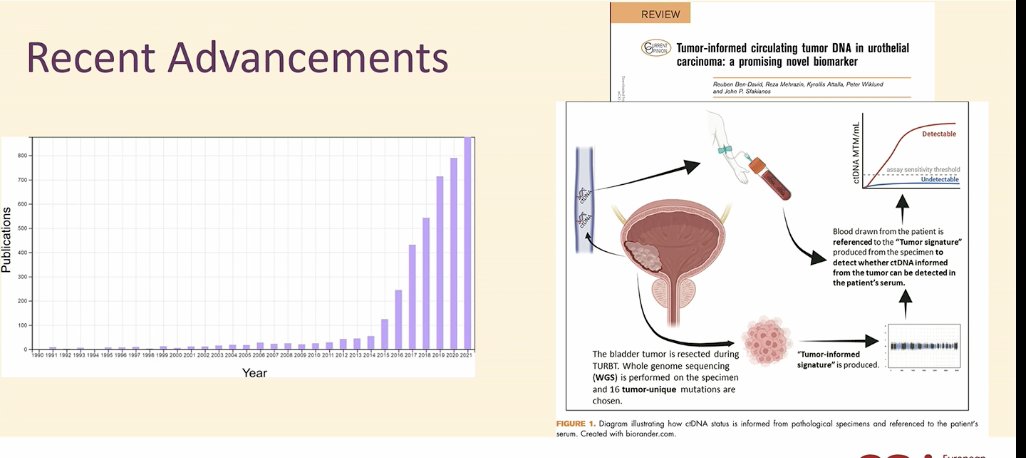
ctDNA is one of the most exciting topics in oncology, with growing momentum over the past five years and a skyrocketing publication record. In bladder cancer, its application is particularly promising, as TURBT specimens provide a valuable source of tumor DNA to guide analysis and decision-making.
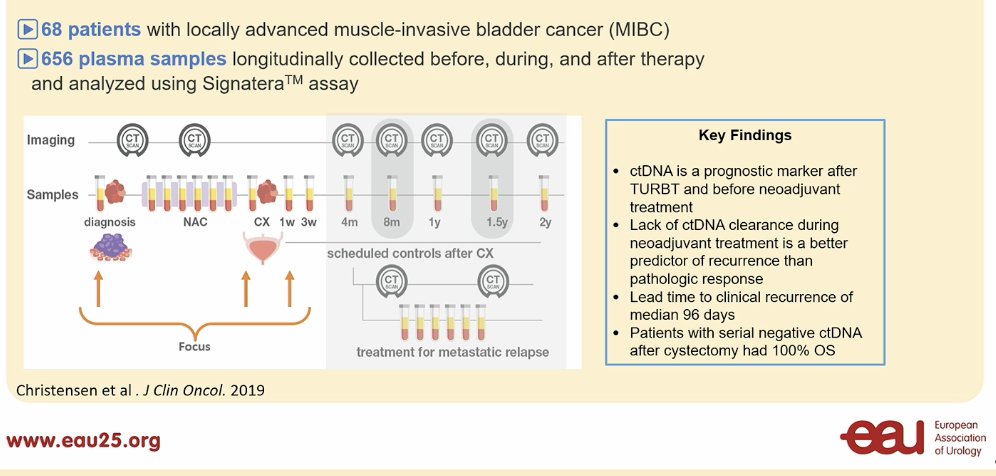
In work by Dr. Lars Drysjokt, 68 patients with locally advanced MIBC were analyzed using 656 plasma samples, demonstrating that ctDNA is a prognostic marker both after TURBT and before neoadjuvant treatment. Notably, a lack of ctDNA clearance during neoadjuvant therapy was a stronger predictor of recurrence than pathological response. The median lead time to clinical recurrence was 96 days, and patients with consistently negative ctDNA had significantly better outcomes.1
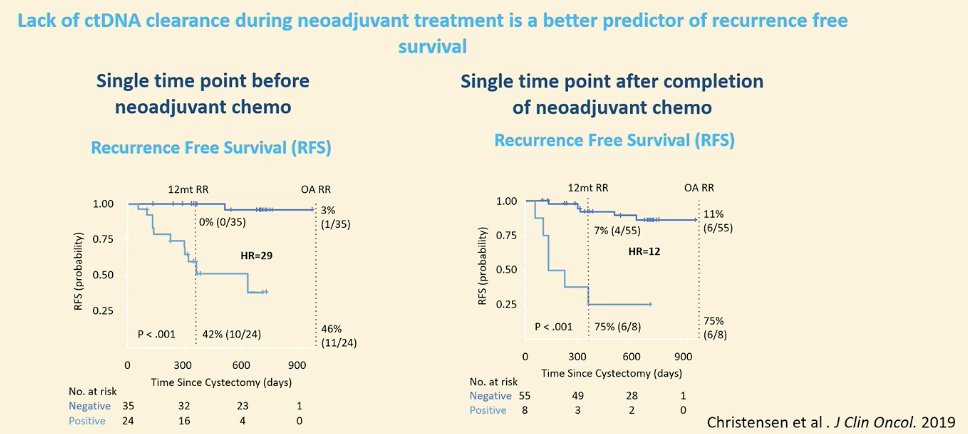
Similarly, this same study found, that even at a single time point before and after chemotherapy, we can risk-stratify patients and identify those with the best recurrence-free survival (RFS), as shown below. Notably, lack of ctDNA clearance during neoadjuvant treatment is a stronger predictor of RFS than pathological response.1
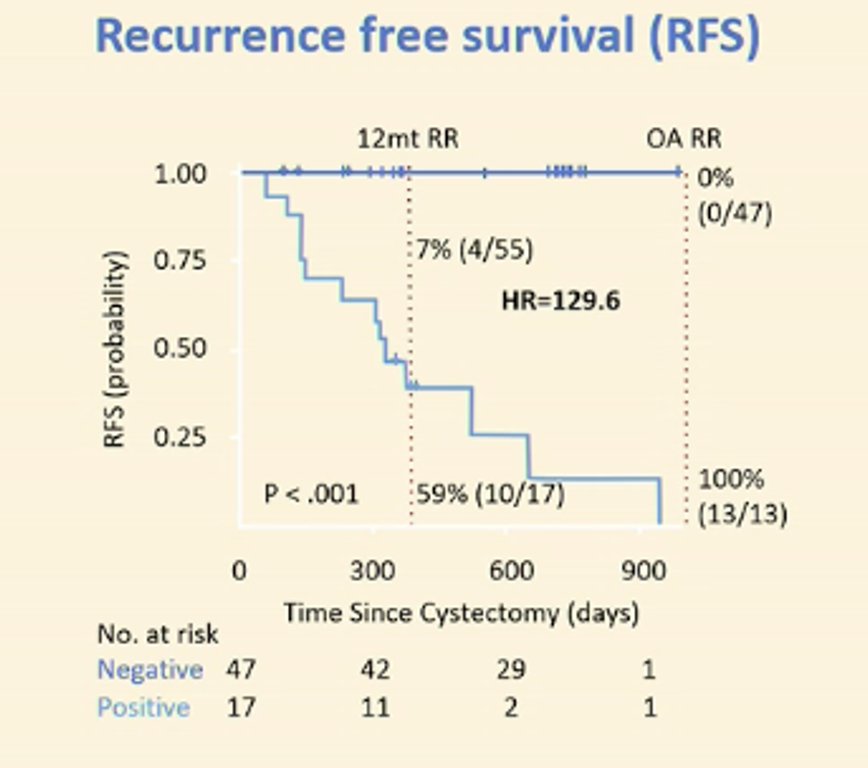
Most importantly, when patients are followed longitudinally, those who remain ctDNA-negative after cystectomy achieve 100% overall survival (OS). ctDNA has proven to be a more reliable predictive factor than lymph node status or pathologic staging. Dr. Sfakianos highlighted the remarkable prognostic value of ctDNA for recurrence-free survival (RFS), with a hazard ratio of 129.6—an impressive finding that is shaping the future direction of research and clinical practice.
Maybe not every patient with MIBC needs neoadjuvant chemotherapy (NAC). Instead, we should focus on escalating treatment only for select patients. Surgery has consistently demonstrated its benefit and remains the standard of care (SOC). While systemic therapy is important, it carries its own risks.
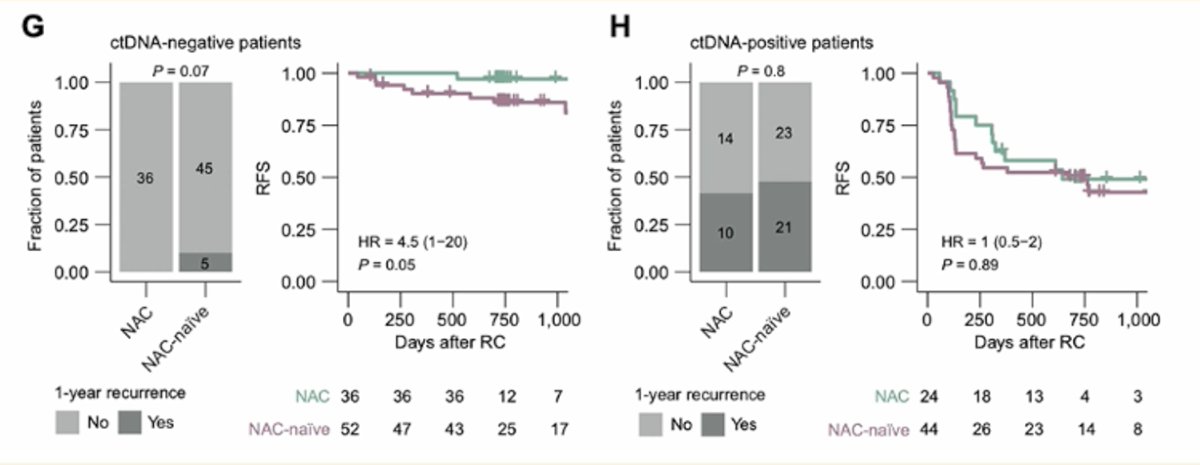
In a study analyzing ctDNA in advanced urothelial carcinoma, patients who were ctDNA-negative after surgery had similar outcomes to those who received NAC, with a 1-year recurrence rate of 5% in NAC-naïve patients versus 0% in the NAC group. This raises the question of whether ctDNA could help refine treatment decisions, potentially sparing some patients from unnecessary systemic therapy.2
In a study by Dr. Sfakianos' group, only 20% of patients with MIBC had undetectable ctDNA before radical cystectomy. Notably, among those with pN1/2 disease, just 10% had undetectable ctDNA, highlighting its potential as a prognostic marker for nodal involvement and disease burden. Which raises again the question if we can treat these patients in a different manner.3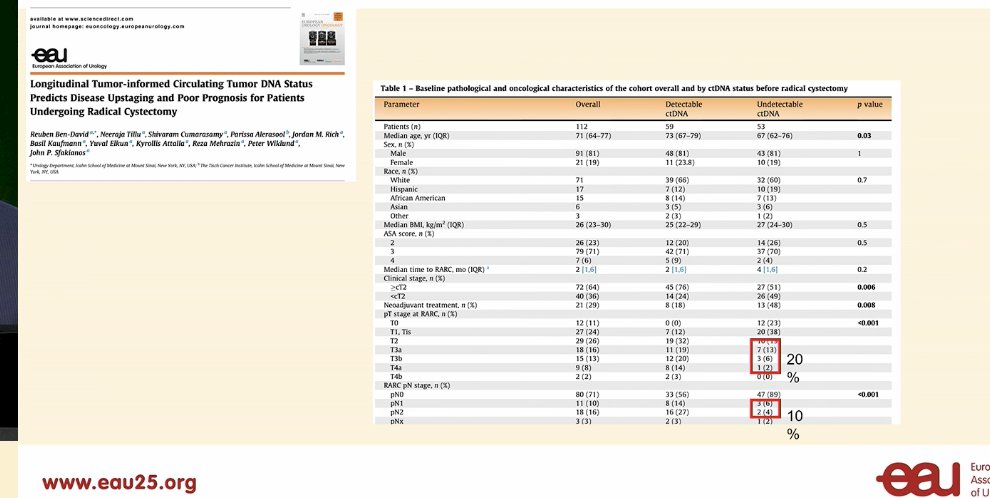
The 12-month RFS is very similar, suggesting that identifying a subgroup of patients with undetectable ctDNA could allow for de-escalation to RC alone. For patients who remain ctDNA-positive, prognosis remains poor regardless of treatment. However, a subset of patients can convert to ctDNA-negative with surgery alone—these patients warrant close attention.3

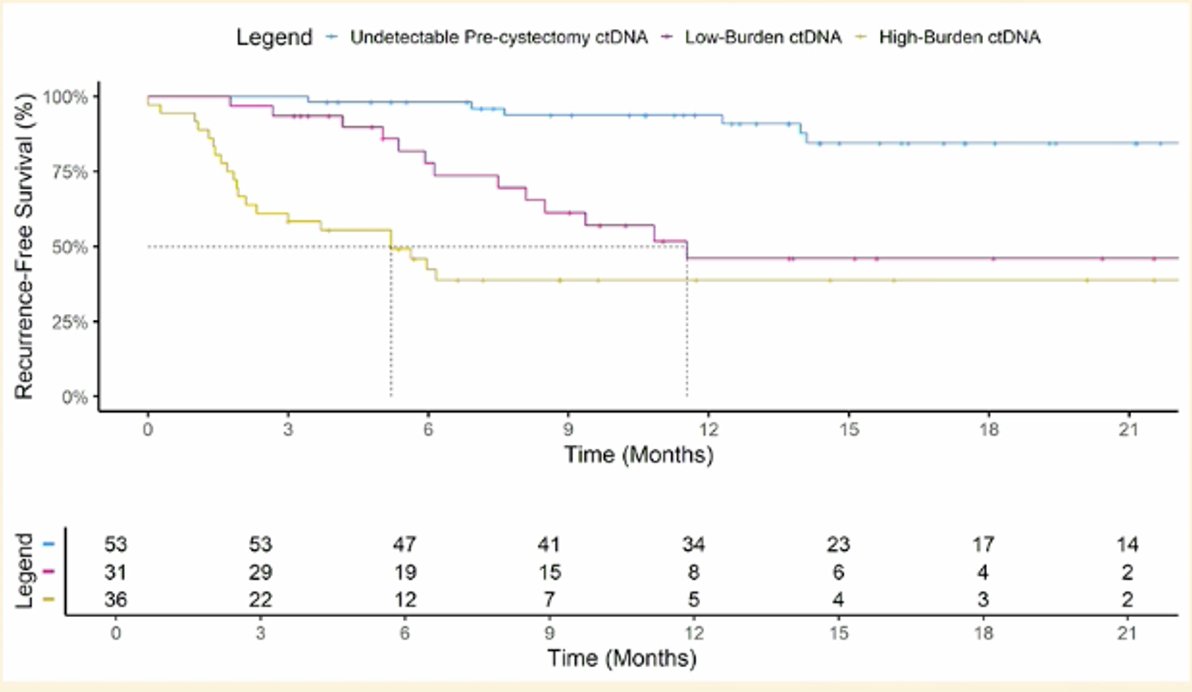
We can start stratifying patients based on absolute ctDNA levels. In a similar study, pre-cystectomy ctDNA burden, measured quantitatively, was predictive of recurrence-free survival (RFS), allowing for a cutoff of 2.5 molecules per mL (MTM/mL).
- High-burden pre-cystectomy ctDNA: 3- and 6-month RFS of 58.3% and 42.4%, respectively, with a median time to recurrence of 5.2 months.
- Low-burden pre-cystectomy ctDNA: 3- and 6-month RFS of 93.6% and 77.7%, respectively.
This cut-off highlights how ctDNA levels can help identify patients with the best prognosis.
Moreover, a study of 94 patients post-RARC demonstrated that ctDNA analysis closely correlated with imaging studies for detecting recurrence, with a diagnostic performance of 100% sensitivity, 92% specificity (95% CI: 87-100%), and 100% negative predictive value (NPV). Notably, patients with undetectable ctDNA at any time point had no recurrence. These findings suggest that if ctDNA remains undetectable, it could serve as a highly reliable marker, potentially allowing for de-escalation of follow-up strategies based on ctDNA results rather than relying solely on pathological findings.
Dr. Sfakianos briefly discussed the DECIDE trial, an MRD-driven decision-making neoadjuvant therapy study in patients undergoing radical cystectomy. Based on ctDNA status, patients are randomized to either immediate cystectomy or neoadjuvant chemotherapy followed by cystectomy. In the adjuvant setting, only those who convert to detectable ctDNA receive additional treatment. The trial aims to refine treatment strategies by identifying patients who may safely avoid unnecessary therapy while ensuring appropriate escalation for those at higher risk. Efforts are underway to launch the trial soon, with the goal of optimizing treatment de-escalation.

Dr. Sfakianos concluded his presentation with the following key points:
- ctDNA is a promising predictive and prognostic biomarker.
- Pre-cystectomy ctDNA, informed by the TURBT specimen, predicts both final pathological outcomes and long-term prognosis, regardless of clinical staging.
- ctDNA can be used in the neoadjuvant setting to guide treatment de-escalation, both for neoadjuvant chemotherapy and surgery.
- ctDNA should be incorporated into all clinical trials to refine treatment strategies.
- Potential role in bladder-sparing approaches, possibly incorporating urine ctDNA.
- ctDNA can enhance surveillance protocols, reducing reliance on imaging.
Presented by: John Sfakianos, MD, is an Associate Professor of Urology and Urologic Oncology at the Icahn School of Medicine at Mount Sinai, New York, NY.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:- Christensen E, Birkenkamp-Demtröder K, Sethi H, Shchegrova S, Salari R, Nordentoft I, Wu HT, Knudsen M, Lamy P, Lindskrog SV, Taber A, Balcioglu M, Vang S, Assaf Z, Sharma S, Tin AS, Srinivasan R, Hafez D, Reinert T, Navarro S, Olson A, Ram R, Dashner S, Rabinowitz M, Billings P, Sigurjonsson S, Andersen CL, Swenerton R, Aleshin A, Zimmermann B, Agerbæk M, Lin CJ, Jensen JB, Dyrskjøt L. Early Detection of Metastatic Relapse and Monitoring of Therapeutic Efficacy by Ultra-Deep Sequencing of Plasma Cell-Free DNA in Patients With Urothelial Bladder Carcinoma. J Clin Oncol. 2019 Jun 20;37(18):1547-1557. doi: 10.1200/JCO.18.02052. Epub 2019 May 6. PMID: 31059311.
- Lindskrog SV, Birkenkamp-Demtröder K, Nordentoft I, Laliotis G, Lamy P, Christensen E, Renner D, Andreasen TG, Lange N, Sharma S, ElNaggar AC, Liu MC, Sethi H, Aleshin A, Agerbæk M, Jensen JB, Dyrskjøt L. Circulating Tumor DNA Analysis in Advanced Urothelial Carcinoma: Insights from Biological Analysis and Extended Clinical Follow-up. Clin Cancer Res. 2023 Dec 1;29(23):4797-4807. doi: 10.1158/1078-0432.CCR-23-1860. PMID: 37782315; PMCID: PMC10690087.
- Ben-David R, Tillu N, Cumarasamy S, Alerasool P, Rich JM, Kaufmann B, Elkun Y, Attalla K, Mehrazin R, Wiklund P, Sfakianos JP. Longitudinal Tumor-informed Circulating Tumor DNA Status Predicts Disease Upstaging and Poor Prognosis for Patients Undergoing Radical Cystectomy. Eur Urol Oncol. 2024 Oct;7(5):1105-1112. doi: 10.1016/j.euo.2024.03.002. Epub 2024 Mar 22. PMID: 38521660.