(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain was host to plenary session on organ-sparing paradigms in kidney and bladder cancer. Dr. Martina Pecoraro discussed the use of bladder MRI for the radiologic evaluation and local staging of muscle-invasive bladder cancer (MIBC).
The EAU guidelines note that one of the roles of imaging in treatment planning of bladder cancer patients is to differentiate T1 from T2 tumors, and MRI using the Vesical Imaging Reporting and Data System (VI-RADS) score can be used in this setting:

Local staging using the MRI VI-RADS score can be used to evaluate for:
- Muscle invasiveness (cT1 versus T2)
- Peri-vesical fat invasion (i.e., cT3)
- Adjacent structure involvement (i.e., cT4)
- Presence/absence of pathologic lymph nodes

The ‘historical timeline’ for the MRI VI-RADS system is as follows:
- 2015: MRI shown to be potentially superior to standard of care for the clinical staging of clinical ≤T1 versus ≥T2 disease, ≥T3, and <T4b versus pT4b disease.
- 2017: Pooled sensitivity and specificity of 0.92 and 0.87, respectively, for differentiating cT1 versus ≥cT2 disease
- 2018: Pooled sensitivity and specificity of 0.90 and 0.88, respectively, for differentiating cT1 versus ≥T2


The American College of Radiology (ACR) has adopted this scoring system which relies on numerous MRI phases (T2-weighted [T2W], diffusion-weighted imaging [DWI], dynamic contrast-enhanced [DCE]) for high-contrast resolution imaging that allows for the optimal evaluation of bladder wall layers.

The ACR VI-RADS scoring system employs a 5-point scale as follows:

Examples are illustrated below, starting with a case of an MRI VIRADS-2 lesion:

VI-RADS 3:

VI-RADS 4:

VI-RADS 5:

As of presentation, there are currently 183 papers on the use of the VI-RADS score and bladder MRI, with 9 published meta-analyses and 1 clinical trial (Bladder Path).
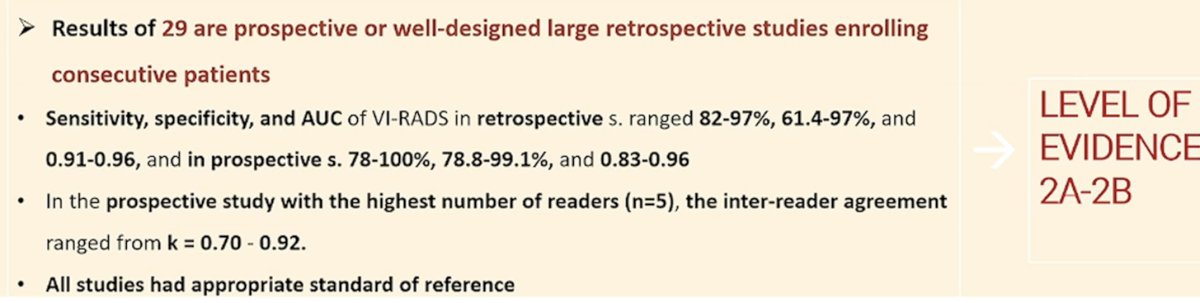
Dr. Percoraro highlighted that this scoring system is associated with a significantly higher inter-reader agreement (Kappa score for 5 readers: 0.7-0.92), compared to the prostate PI-RADS scoring system, which is critical for wide-spread adoption.

In 2020, Del Giudice et al. published the results of two studies evaluating the VI-RADS scoring system for:1,2
- Discriminating between non-muscle and muscle-invasive bladder cancer at TURBT
- Predicting locally advanced bladder cancer in neoadjuvant chemotherapy refusing/ineligible patients who underwent mpMRI of the bladder prior to staging TURBT followed by radical cystectomy for MIBC
At initial TURBT, mpMRI demonstrated a sensitivity of 92% and specificity of 91% for distinguishing NMIBC from MIB at initial TURBT.
For differentiating those with muscle-confined from extravesical MIBC, the performance characteristics were as follows:
- Extravesical bladder cancer: Sensitivity of 90% and specificity of 98%
- Muscle-confined bladder cancer: Sensitivity of 95%, specificity of 96%
- Based on these results, the study investigators concluded that VI-RADS is valid and reliable in differentiating patients with extravesical disease from those with muscle-confined bladder cancer prior to TURBT. Moving forward, higher VI-RADS scores could potentially avoid the morbidity of extensive primary resections in favour of sampling-TUR for histology.

Additionally, the MRI VI-RADS score has been incorporated into clinical trials to evaluate whether definitive treatment can be expedited for MIBC. BladderPath is a prospective open-label, randomized study conducted within 17 UK hospitals. Participants with suspected new bladder cancer were randomly assigned 1:1 to TURBT-staged or mpMRI-staged care.

Between May 2018 and December 2021, 143 participants were randomly assigned to TURBT (n=72; 15 MIBCs) or initial mpMRI (n=71; 14 MIBCs). The median time to correct treatment for participants with MIBC was significantly shorter with initial mpMRI (53 versus 98 days, p=0.02).3 Thus, the mpMRI-directed pathway led to a 45-day reduction in time to correct treatment for patients with MIBC.
Dr. Pecoraro concluded her presentation by providing guidance into how the MRI VI-RADS scoring system can be incorporated into a contemporary bladder cancer management paradigm:

Presented by: Martina Pecoraro, MD, Department of Radiological Sciences, Oncology and Pathology, Sapienza University/Policlinico Umberto I, Viale del Policlinico 155, 00161, Rome, Italy
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:
- Del Giudice F, Leonardo C, Simone G, et al. Preoperative detection of Vesical Imaging-Reporting and Data System (VI-RADS) score 5 reliably identifies extravesical extension of urothelial carcinoma of the urinary bladder and predicts significant delayed time to cystectomy: time to reconsider the need for primary deep transurethral resection of bladder tumour in cases of locally advanced disease? BJU Int. 2020; 126(5): 610-9.
- Del Giudice F, Barchetti G, De Berardinis E, et al. Prospective Assessment of Vesical Imaging Reporting and Data System (VI-RADS) and Its Clinical Impact on the Management of High-risk Non-muscle-invasive Bladder Cancer Patients Candidate for Repeated Transurethral Resection. Eur Urol. 2020; 77(1): 101-9.
- Bryan RT, Liu W Pirrie SJ, et al. Randomized Comparison of Magnetic Resonance Imaging Versus Transurethral Resection for Staging New Bladder Cancers: Results From the Prospective BladderPath Trial. J Clin Oncol. 2025: JCO2302398.