(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain was host to a plenary session on organ-sparing paradigms in kidney and bladder cancer. Drs. Marek Babjuk, Antoni Vilaseca Cabo, and Ashish Kamat discussed various strategies for the management of low-risk, recurrent non-muscle invasive bladder cancer (NMIBC) in elderly patients:
- Fulguration as day care protocol
- Chemoablation in mutated tumors (.e.g, FGFR altered [FGFRalt])
- Active surveillance strategies
The session began with a case presentation of an 84-year-old, fit female patient with the following bladder cancer history:
- August 2020: 2 cm bladder tumor TURBT: TaG1 urothelial carcinoma
- February 2022: 0.8 cm recurrence TURBT: TaG1
- March 2024: A likely TaG1 2cm recurrence, with a negative urinary cytology
What are the next steps in management?
Arguing in favor of in-office fulguration, Dr. Babjuk noted that the relevant clinical questions in this scenario are as follows:
- Can we discern low- from high-grade tumors at cystoscopy?
- What is the prognosis of such a patient?
- What are the available methods and are they safe/feasible?
- What are the oncological outcomes in such a scenario?
With regards to predicting low-grade disease at cystoscopy, Marlappan et al. have previously demonstrated that the overall positive predictive value for low-grade tumors at cystoscopy is 86% (88% for tumors <3 cm).1 In other words, if a lesion appears to be low-grade on cystoscopy and then a TURBT is performed, the lesion is pathologically confirmed low-grade ~90% of the time. Thus, Dr. Babjuk argued that, in general, we may presume a low risk of high-grade recurrence in such patients with a history of recurrent low-grade tumors who have a low-grade appearing lesion on surveillance.
What is the prognosis of this patient? Based on the current EAU risk stratification model of 2021, this patient meets the criteria for intermediate-risk disease given that she has recurrent LG Ta lesions <3 cm with no CIS component. Her risk of disease progression at 5 years is ~5%, per the EAU risk classification model. However, when we apply the IBCG risk stratification to sub-stratify these intermediate-risk patients, we note that this patient has 0 high-risk factors (multiple lesions, tumor size >3 cm, early recurrence <1-year, frequent recurrences >1/year), and is thus in intermediate risk ‘low’ subgroup.

Based on the current evidence, she has a ‘negligible’ risk of progression with a ~30% risk of disease recurrence and should be treated similarly to low risk patients.1

What do the current guidelines say about in-office fulgurations?
- EAU: Patients with small recurrent low-grade Ta tumors can be effectively and safely offered office fulguration (strong recommendation)
- AUA/SUO: In a patient with a history of low-grade Ta disease and a noted subcentimeter papillary tumor(s), a clinician may consider in-office fulguration as an alternative to resection under anesthesia (Expert opinion)
- NICE: Consider fulguration without a biopsy for people with recurrent NMIBC if they have all of the following:
- No previous intermediate- or high-risk bladder cancer
- A disease-free interval of at least 6 months
- Solitary papillary recurrence
- A tumor diameter of 3 mm or less
Available methods for ablation include:
- Fulguration (e.g., monopolar ‘bugbee’ electrode’)
- Laser ablation
- Ho:YAG, 980 nm diode laser, Nd:YAG
- Thullium fiber laser
Importantly, it appears that currently available fulguration/laser ablation techniques are safe, with the following pooled results from a 2022 systematic review by Malde et al. published in European Urology Oncology:3

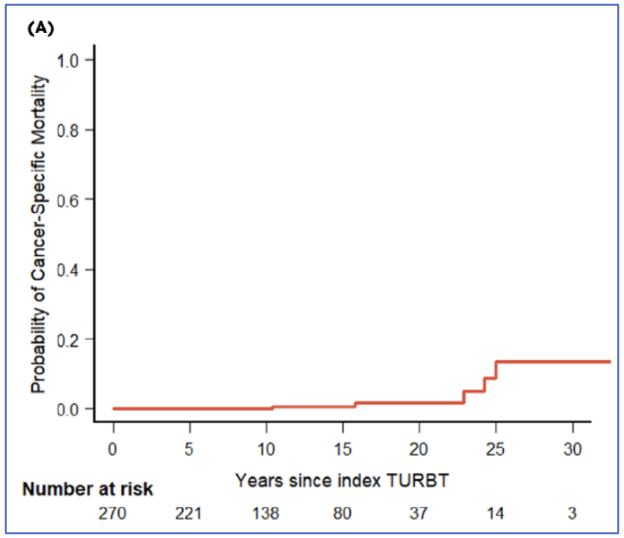
In addition to being safe, long-term follow-up of a cohort of 270 patients with recurrent low-grade Ta tumors treated with in office fulguration (mean follow-up: 11.7 years) demonstrated that the 10-year progression rate was only 3.1%.
What about the efficacy of in-office laser ablation? In 2023, Pedersen et al. published the results of a trial of 206 patients with tumors ≤1.5 cm randomized to either laser photocoagulation with a 980 nm diode laser or TURBT. After 4 months, the recurrence-free survival rate was 57% in the laser arm versus 49% in the TURBT arm. Complications were noted in 2% and 10% of patients in the ablation and TURBT arms, respectively.4
Dr. Babjuk concluded his argument by noting that in well-selected patients, in-office fulguration or laser ablation is feasible, safe, and effective.
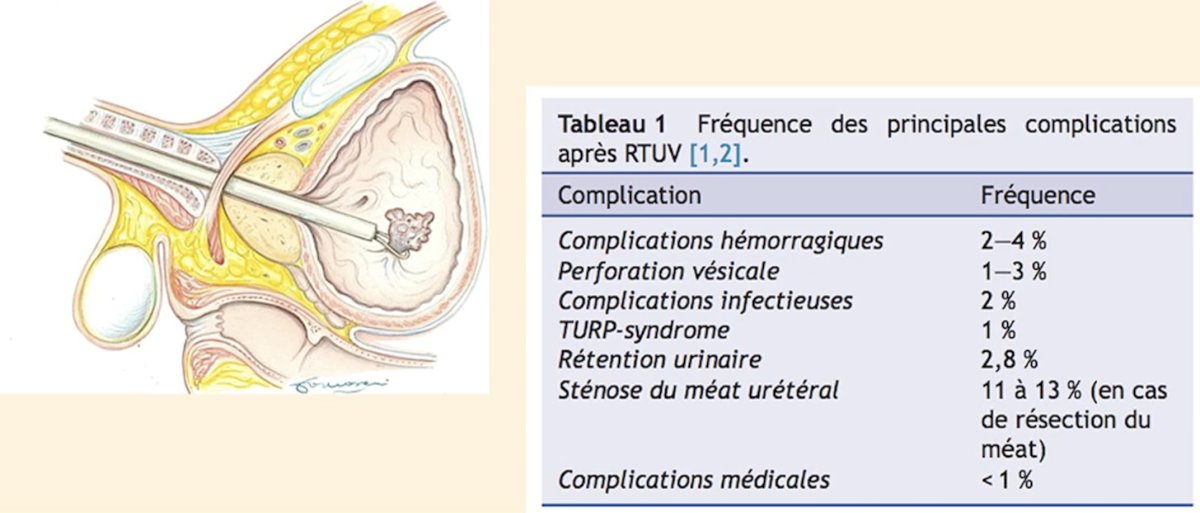
Next, Dr. Vilaseca argued in favor of chemoablation in such a setting, specifically for mutated tumors (e.g., FGFRalt). He noted that TURBT, although not a major urologic procedure, is associated with significant, often underappreciated complication rates:
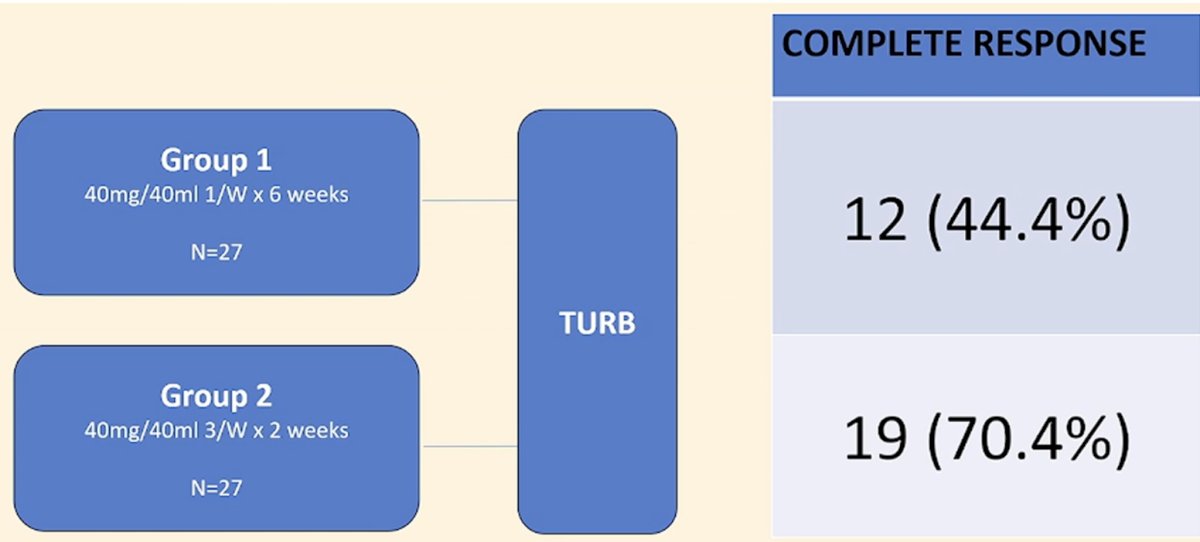
What is the evidence for chemoablation for low-grade tumors? In 2012, Colombo et al. published the results of a phase II trial of neoadjuvant short-term intensive intravesical mitomycin C (3 instillations/week for 2 weeks prior to TURBT) versus a neoadjuvant weekly schedule (1/week x 6 weeks prior to TURBT) for low-grade, recurrent NMIBC. They demonstrated that the complete response rates were superior in the ‘intense’ neoadjuvant strategy arm (70% versus 44%).5
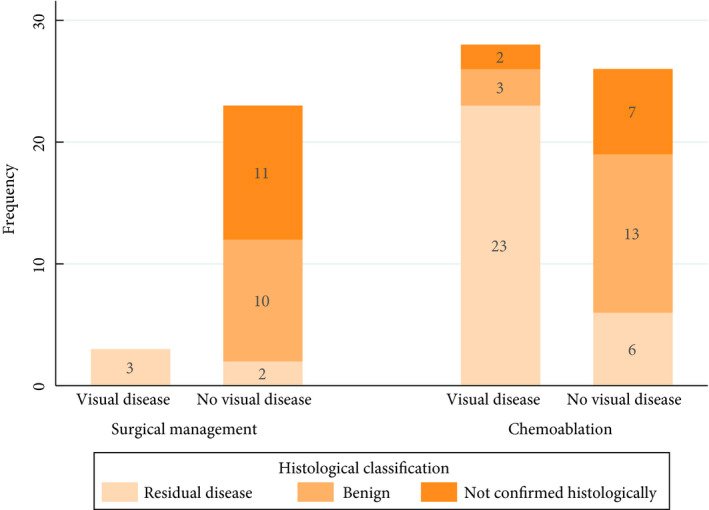
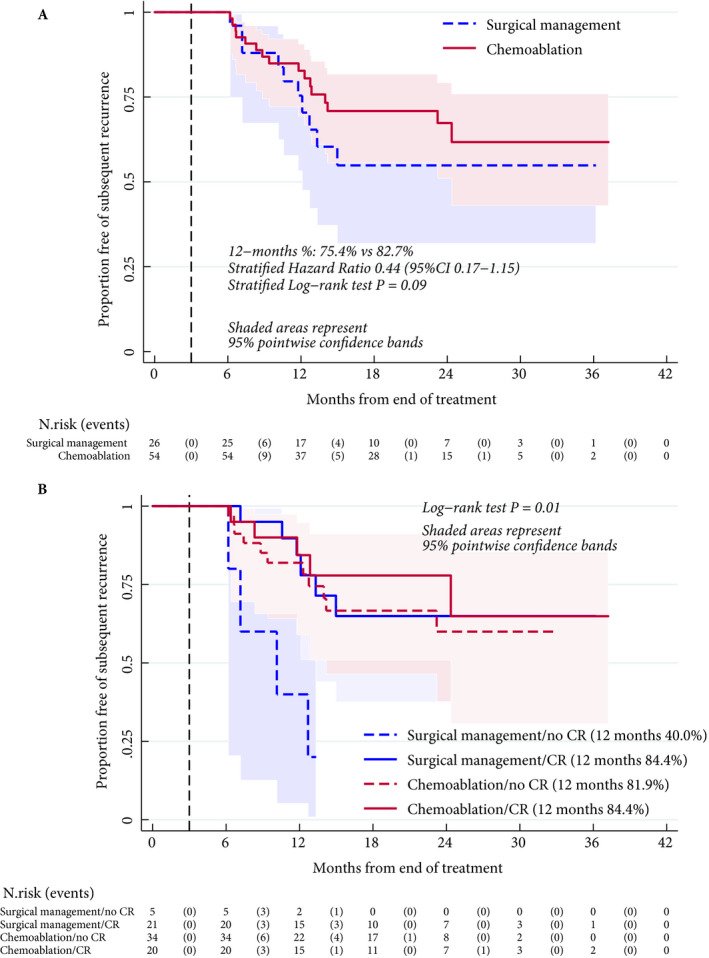
CALIBER, published in 2020,6 was a phase II feasibility trial whereby patients with low-risk NMIBC were randomized 2:1 to treatment with four once-weekly mitomycin-C 40-mg intravesical instillations (chemoablation arm) or to surgical management. Between February 2015 and August 2017, 82 patients with a visual diagnosis of recurrent low-risk NMIBC were enrolled from 24 UK hospitals (chemoablation, n = 54; surgical management, n =28), and followed for a median of 24 months. The 3 months complete response rate was 81% with surgical management versus 37% with mitomycin-C ablation. Amongst patients with a complete response at 3 months, the 12-months recurrence-free rates were identical in both groups (84%). Notably, amongst those with residual disease at 3 months, the 12-month recurrence-free proportion was lower in the surgical management group (40%), compared to the chemoablation group (84%). Ultimately, recruitment was suspended early as chemoablation did not meet the prespecified threshold of 45% complete responses at 3 months.
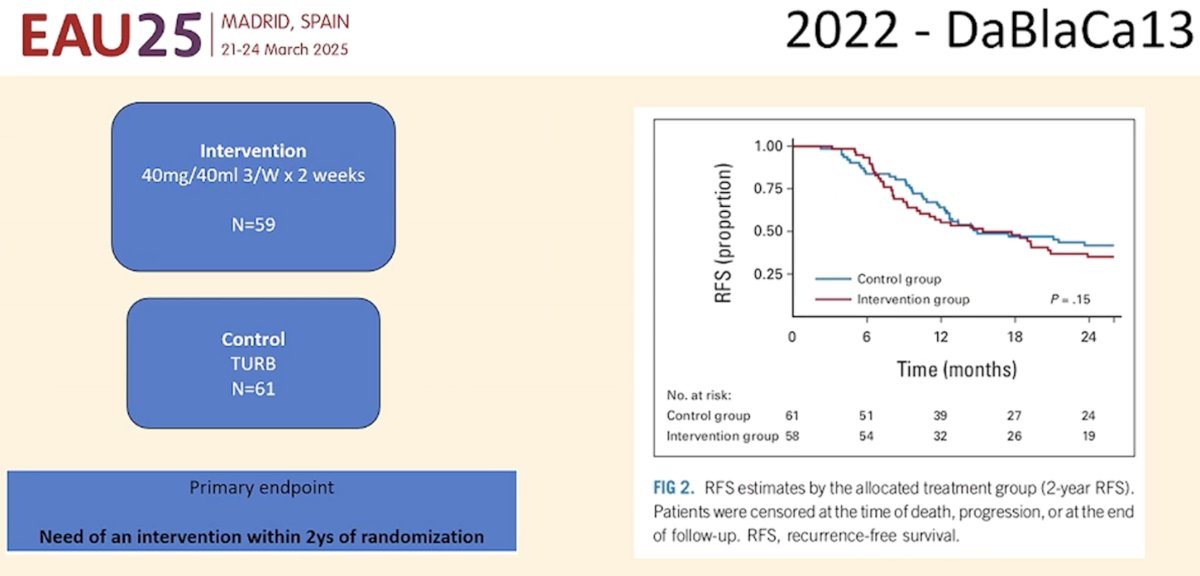
In 2023, the DaBlaCa13 trial was published in The Journal of Clinical Oncology.7 This was a Danish randomized clinical trial of 120 patients with a history of Ta low- or high-grade NMIBC who were included upon recurrence and randomized to:
- Intervention: Intravesical mitomycin-C (40 mg/40 mL) three times a week for 2 weeks and TURBT or office biopsy only if the response was incomplete
- TURBT or office biopsy and 6 weekly adjuvant instillations
This trial demonstrated that fewer patients in the intervention group required a procedure (71% versus 100%). There were no differences in the 12-months recurrence-free survival rates (36% versus 43%, p=0.5).
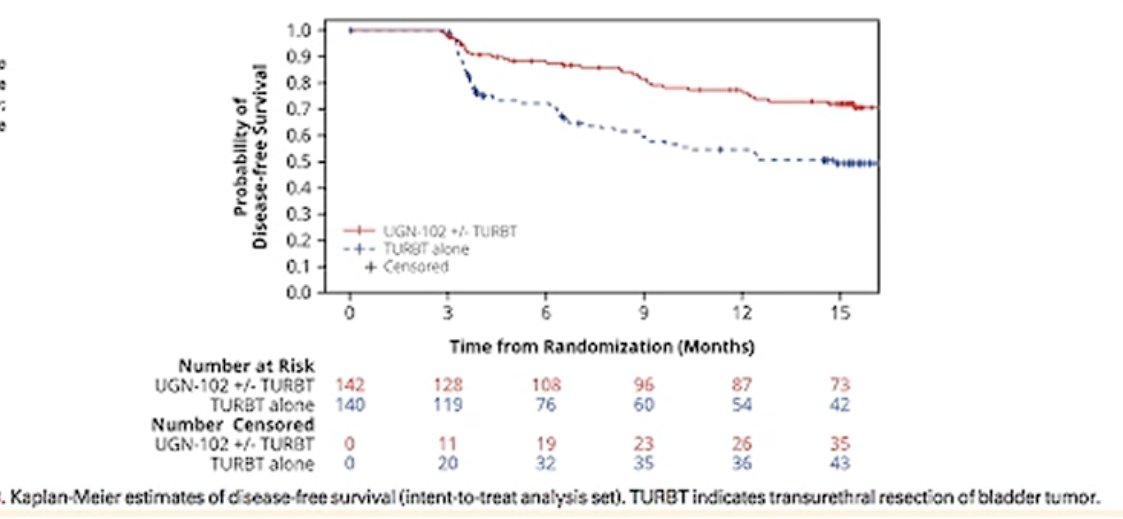
Novel bladder chemoablative treatment options are emerging. Dr. Vilaseca highlighted UGN-102, a reverse thermal gel containing mitomycin, that was evaluated in ATLAS a randomized phase III trial of UGN-102 once weekly for 6 weeks versus TURBT in patients with new or recurrent low-grade, intermediate-risk NMIBC.
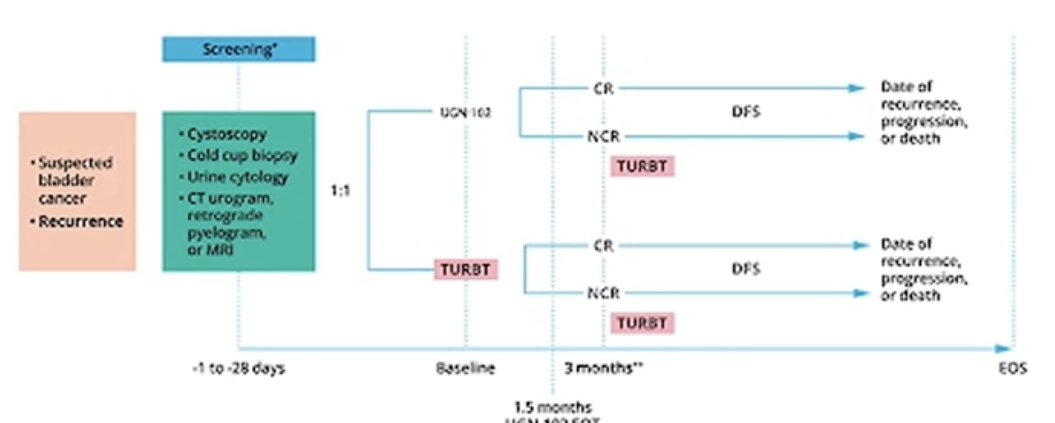
Tumor-free complete response 3 months after initial treatment was achieved by 65% of UGN-102-treated patients and 64% of TURBT patients. The estimated probability of disease-free survival 15 months after randomization was 72% for UGN-102 ± TURBT and 50% for TURBT patients.8
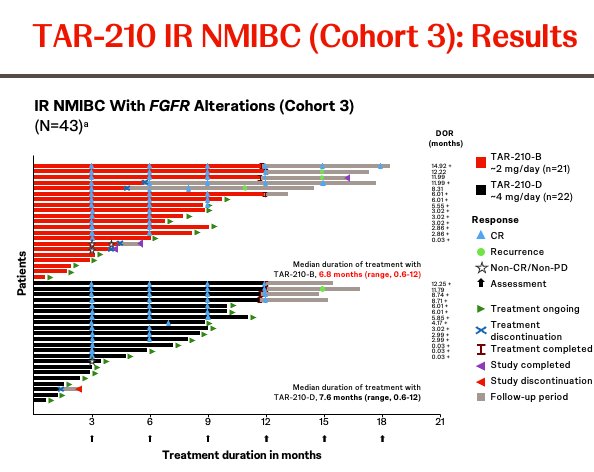
Another promising, emerging option in this space is TAR-210, which is designed to release sustained local erdafitinib, a pan-FGFR inhibitor, intravesically for 3 months. At AUA 2024, Dr. Vilaseca presented the first safety and efficacy results of an open-label, multicenter phase I study (NCT05316155) that evaluated TAR-210 in patients with NMIBC whose tumors harbor select FGFRalt.
This study included two cohorts:
- Cohort 1; High-risk NMIBC (HG Ta/T1, no CIS, papillary only), BCG-experienced/unresponsive and not undergoing radical cystectomy. All patients in this cohort had a TURBT with complete resection of all visible disease prior to treatment.
- Cohort 3: Intermediate-risk NMIBC (LG Ta/T1 disease) and visible target lesions prior to treatment (chemoablation design)

The baseline characteristics were as follows:
In cohort 3 (chemoablation cohort), 90% achieved a complete response, with 28/31 achieving this response by week 12.
Significantly, TAR-210 provided sustained erdafitinib release in the urine over 90 days with very low plasma concentrations:
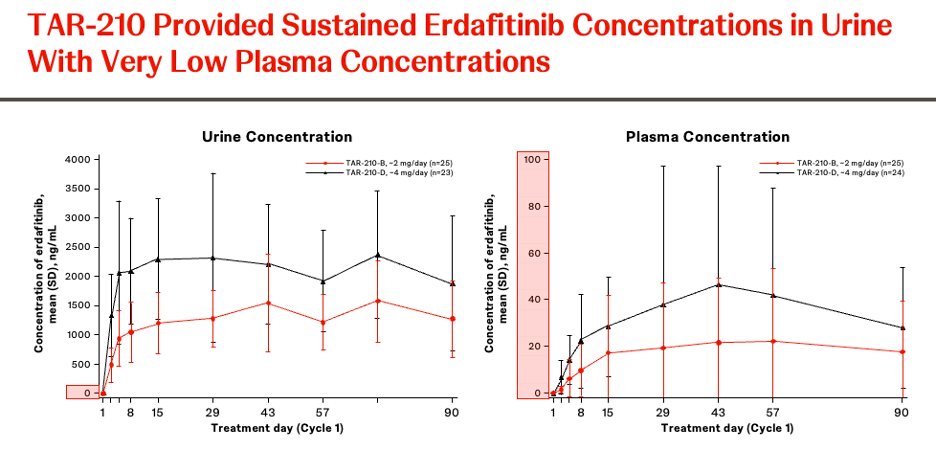
The adverse event profile was favorable, and there were no dose-limiting toxicities.

Dr. Vilaseca concluded his argument in favor of ablation as follows:
- TURBT is associated with some adverse events, and NMIBC is associated with high recurrence rates
- Chemoablation for low- to intermediate-risk NMIBC is feasible
- In a pooled meta-analysis of mitomycin-C, BCG, epirubicin, and gemcitabine, the complete response rate was 51%9
- Thermogels for mitomycin-C can improve complete response rates up to 65% in ATLAS and up to 80% in ENVISION10
- FGFR-directed chemoablation can achieve complete response rates in 90% of cases
Finally, Dr. Kamat argued in favor of surveillance in this scenario. While the patient in question has, by definition, EAU intermediate-risk disease, this group includes a heterogenous population of candidate patients:
- Recurrent low-grade disease (case example presented)
- Primary, large (>3 cm) LG Ta
- High-grade Ta with, at most, one high-risk clinical feature

Dr. Kamat noted that the updated 2022 IBCG guidelines provide further nuance and guidance for the management of intermediate-risk patients. The IBCG risk classification stratifies patients based on the number of risk factors present, as follows, with the 5-year risks of recurrence and progression with sequential intravesical gemcitabine + docetaxel summarized below:11

Importantly, this scoring system can be used to predict the subsequent time of surveillance. In an analysis of 163 patients with low-grade Ta/T1 NMIBC followed for a median of 33 months, patients with 0 risk factors, such as the patient in the case example, were over 2-fold more likely to continue active surveillance compared to patients with ≥3 risk factors (59% vs 24%). Multivariable analysis adjusted for age, T stage, and sex demonstrated that the IBCG intermediate-risk NMIBC scoring system was associated with subsequent rates of surveillance discontinuation and performance of a TURBT (1-2 risk factors: HR=1.66, p=0.072; ≥3 risk factors: HR=3.21, p<0.001).12

Furthermore, when the IBCG intermediate-risk NMIBC scoring system is applied, we note that low-grade, intermediate-risk NMIBC patients with 0 risk factors have 3-year recurrence-free survival rates of 86%, including 92% for high-grade recurrences.13

Based on the current evidence, the following algorithm for the management of primary low-grade Ta disease, which incorporates active surveillance as an option for IBCG intermediate-risk NMIBC with ≤2 risk factors, has been proposed:

- Marek Babjuk, MD, PhD, Professor, Department of Urology, 2nd Faculty of Medicine, Hospital Motol, Prague, Czech Republic
- Antoni Vilaseca Cabo, MD, Hospital Clínic de Barcelona, Barcelona, Spain
- Ashish Kamat, MD, MBBS, Professor of Urology, and Wayne B. Duddleston Professor of Cancer Research, University of Texas, MD Anderson Cancer Center, Houston, TX
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:
- Mariappan P, Lavin V, Phua CQ, et al. Predicting Grade and Stage at Cystoscopy in Newly Presenting Bladder Cancers-a Prospective Double-Blind Clinical Study. Urology. 2017; 109:134-9.
- Soria F, Rosazza M, Livoti, S, et al. Clinical Validation of the Intermediate-risk Non-muscle-invasive Bladder Cancer Scoring System and Substratification Model Proposed by the International Bladder Cancer Group: A Multicenter Young Academic Urologists Urothelial Working Group Collaboration. Eur Urol Oncol. 2024; 7(6): 1497-503.
- Malde S, Grover S, Raj S, et al. A Systematic Review of the Efficacy and Safety of Outpatient Bladder Tumour Ablation. Eur Urol Focus. 2022; 8(1): 141-51.
- Pedersen GL, Erikson MS, Mogensen K, et al. Outpatient Photodynamic Diagnosis-guided Laser Destruction of Bladder Tumors Is as Good as Conventional Inpatient Photodynamic Diagnosis-guided Transurethral Tumor Resection in Patients with Recurrent Intermediate-risk Low-grade Ta Bladder Tumors. A Prospective Randomized Noninferiority Clinical Trial. Eur Urol. 2023; 83(2): 125-30.
- Colombo R, Rocchini L, Suardi N, et al. Neoadjuvant short-term intensive intravesical mitomycin C regimen compared with weekly schedule for low-grade recurrent non-muscle-invasive bladder cancer: preliminary results of a randomised phase 2 study. Eur Urol. 2012; 62(5): 797-802.
- Mostafid AH, Porta N, Cresswell J, et al. CALIBER: a phase II randomized feasibility trial of chemoablation with mitomycin-C vs surgical management in low-risk non-muscle-invasive bladder cancer. BJU Int. 2020l 125(6): 817-26.
- Lindgren MS, Hansen E, Azawi N, et al. DaBlaCa-13 Study: Oncological Outcome of Short-Term, Intensive Chemoresection With Mitomycin in Nonmuscle Invasive Bladder Cancer: Primary Outcome of a Randomized Controlled Trial. J Clin Oncol. 2023; 41(2): 206-11.
- Prasad SM, Huang WC, Shore ND, et al. Treatment of Low-grade Intermediate-risk Nonmuscle-invasive Bladder Cancer With UGN-102 ± Transurethral Resection of Bladder Tumor Compared to Transurethral Resection of Bladder Tumor Monotherapy: A Randomized, Controlled, Phase 3 Trial (ATLAS). J Urol. 2023; 210(4):619-29.
- Yanagisawa T, Quhal F, Kawada T, et al. A Systematic Review and Meta-analysis of Chemoablation for Non-muscle-invasive Bladder Cancer. Eur Urol Focus. 2023; 9(3): 463-79.
- Prasad SM, Shishkov D, Mihaylov NV, et al. Primary Chemoablation of Recurrent Low-Grade Intermediate-Risk Nonmuscle-Invasive Bladder Cancer With UGN-102: A Single-Arm, Open-Label, Phase 3 Trial (ENVISION). J Urol. 2025; 213(2): 205-16.
- Tan WS, McElree IM, Davaro F, et al. Sequential Intravesical Gemcitabine and Docetaxel is an Alternative to Bacillus Calmette-Guérin for the Treatment of Intermediate-risk Non-muscle-invasive Bladder Cancer. Eur Urol Oncol. 2023; 6(5): 531-4.
- Tan WS, Contieri R, Buffi NM, et al. International Bladder Cancer Group Intermediate-risk Nonmuscle-invasive Bladder Cancer Scoring System Predicts Outcomes of Patients on Active Surveillance. J Urol. 2023; 210(5): 763-70.
- Zaurito P, Scilipoti P, Longoni M, et al. Identifying optimal candidates for active surveillance in low-grade intermediate-risk non-muscle invasive bladder cancer. W J Urol. 2025; 43(1):113.