(UroToday.com) The 2025 EAU annual meeting featured a game changer session and a discussant presentation by Dr. Paolo Gontero. Dr. Gontero discussed Dr. Psutka’s presentation “Perioperative outcomes of neoadjuvant TAR-200 + cetrelimab or cetrelimab alone in patients with muscle invasive bladder cancer ineligible for or refusing neoadjuvant cisplatin-based chemotherapy.” When assessing the tolerability of neoadjuvant therapy, Dr. Gontero notes that there are certain safety expectations, including (i) not delaying radical cystectomy, (ii) minimizing toxicity to the patient, and (iii) not worsening the morbidity of surgery.
A potential comparator to the SunRISe-4 trial is the NIAGARA trial of systemic gemcitabine + cisplatin + durvalumab,1 however he notes that this is a different population (cisplatin fit) compared to SunRISe-4 (cisplatin unfit and cisplatin refused). Comparing these two trials, Dr. Gontero emphasized that there was a reduction in treatment related adverse events (grade 3+) for SunRISe-4 (11% versus 37% in NIAGARA) and a reduction in adverse events leading to treatment discontinuation (7.6% versus 15% in NIAGARA), which is welcomed in a cisplatin unfit population: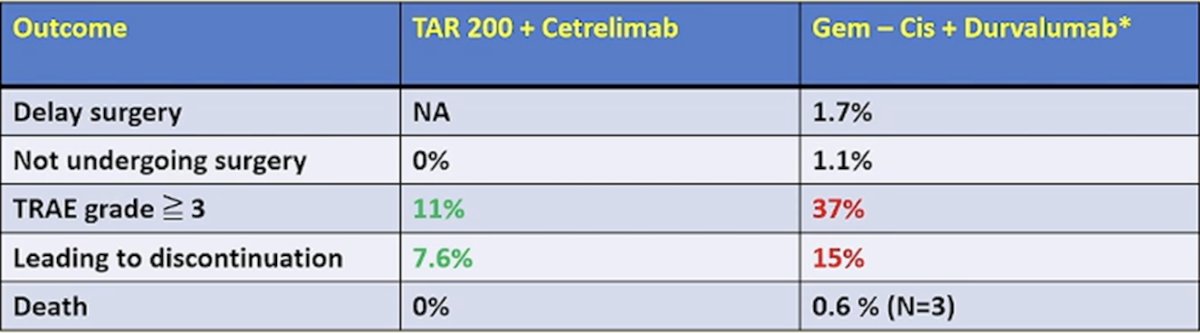
A second consideration for neoadjuvant therapy is the efficacy of therapy. Our expectations are to improve cancer specific survival (primary endpoint), with a surrogate endpoint being improved pathological complete response. The ideal mechanism of action is to eradicate micrometastatic disease. In SunRISe-4, the combination of TAR-200 + cetrelimab had a pathological complete response rate of 42% (which is almost double cetrelimab alone). However, does complete response achieved with local therapy translate into a systemic benefit? The hypothesis here is that local disease control driven by TAR-200 is more suited for bladder sparing approaches.
Dr. Gontero concluded his discussant presentation of SunRISe-4 with the following take home points regarding the combination of TAR-200 + cetrelimab:
- The combination halves the G3+ toxicity and treatment discontinuation rates compared with a combination of systemic chemotherapy and immune checkpoint inhibitor
- There was no negative effect on surgery
- There is a higher pathological complete response rate driven by TAR 200 (versus cetrelimab alone)
- A survival advantage is yet to be demonstrated
- This is clearly an option worthy of further exploration in the cisplatin unfit muscle invasive bladder cancer population.
Presented by: Paolo Gontero, MD, Torino School of Medicine, Torino, Italy
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References: