(UroToday.com) The 2025 EAU annual meeting featured a game changer session and a presentation by Dr. James Catto discussing surgical outcomes and neoadjuvant safety with perioperative durvalumab for muscle-invasive bladder cancer in the NIAGARA trial. NIAGARA was the first global phase 3 study to evaluate perioperative immunotherapy, durvalumab, combined with neoadjuvant chemotherapy in cisplatin eligible patients with muscle invasive bladder cancer:1

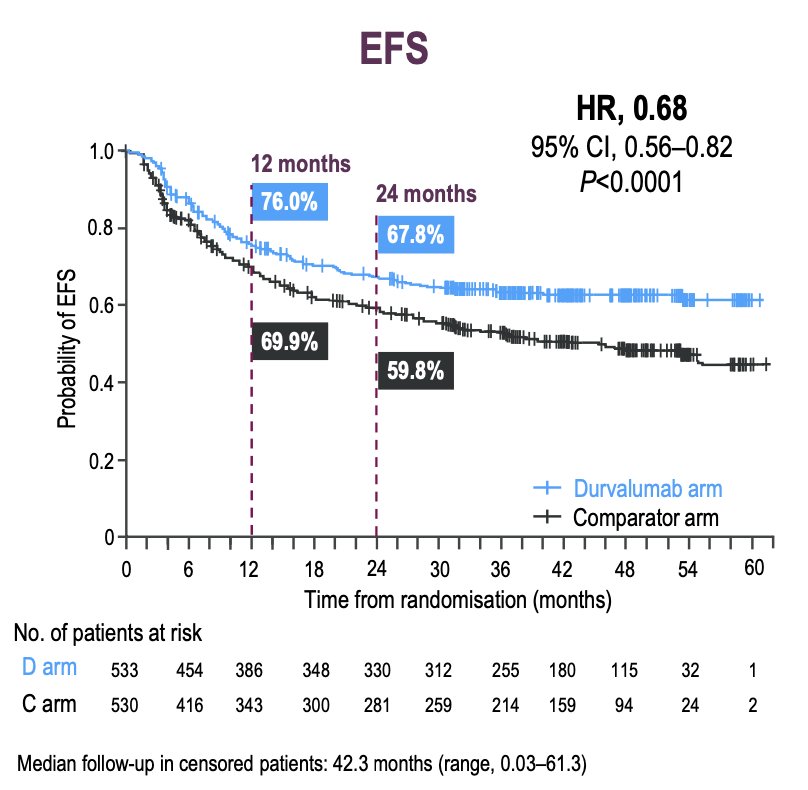
The first line results were initially presented at ESMO 2024, noting that event free survival, as assessed by blinded independent central review in the intention to treat population, showed an event free survival at 2 years of 67.8% in the durvalumab arm compared to 59.8% in the comparator arm. The hazard ratio for event free survival was 0.68 (95% CI 0.56–0.82, p < 0.0001):
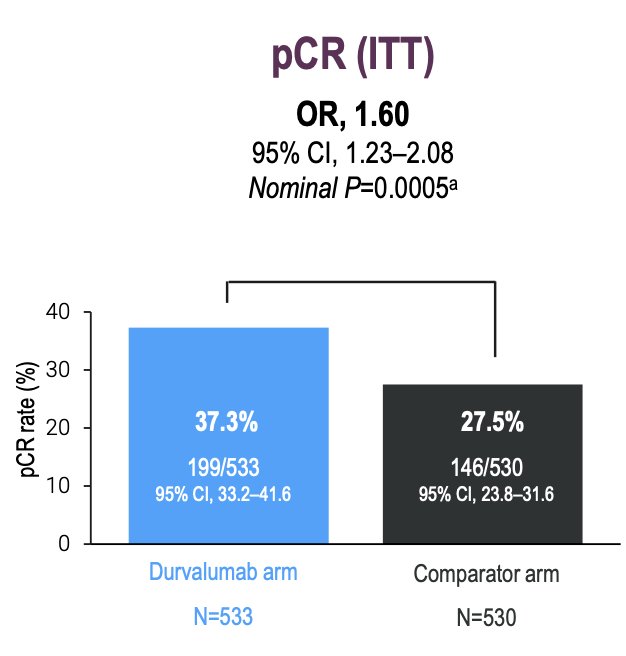
In the intention to treat population, pathological complete response was 37.3% in the durvalumab arm versus 27.5% in the comparator arm (OR 1.60, 95% CI 1.23-2.08):
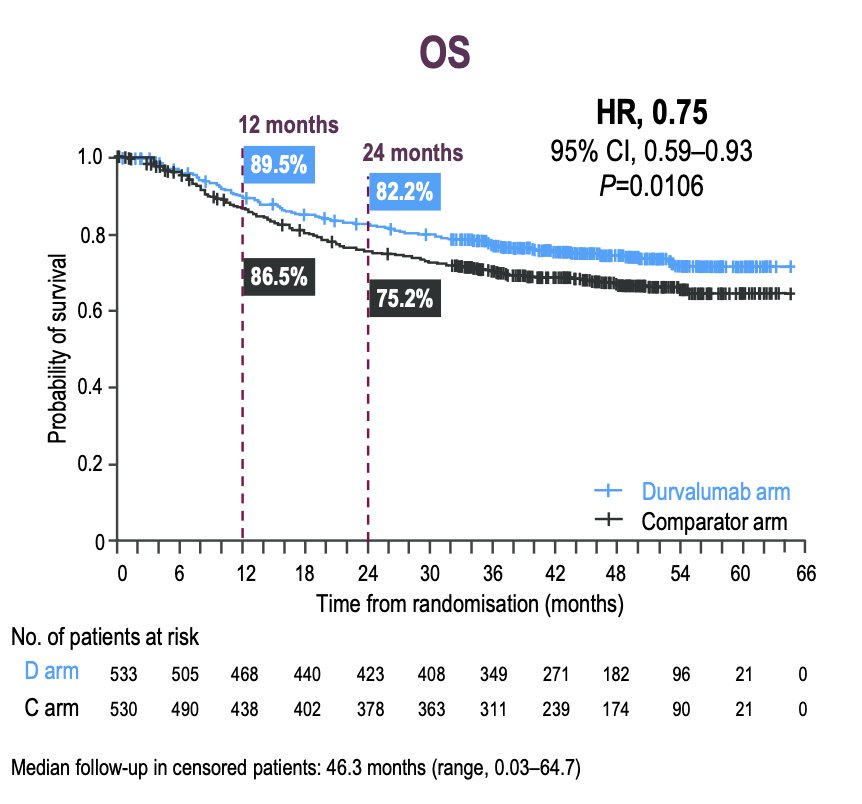
The median follow-up for the overall survival analysis in censored patients was 46.3 months (range 0.03–64.7). At 24 months, 82.2% of patients in the durvalumab arm were alive, compared to 75.2% in the comparator arm. The hazard ratio for overall survival was 0.75 (95% CI 0.59–0.93, p = 0.016):
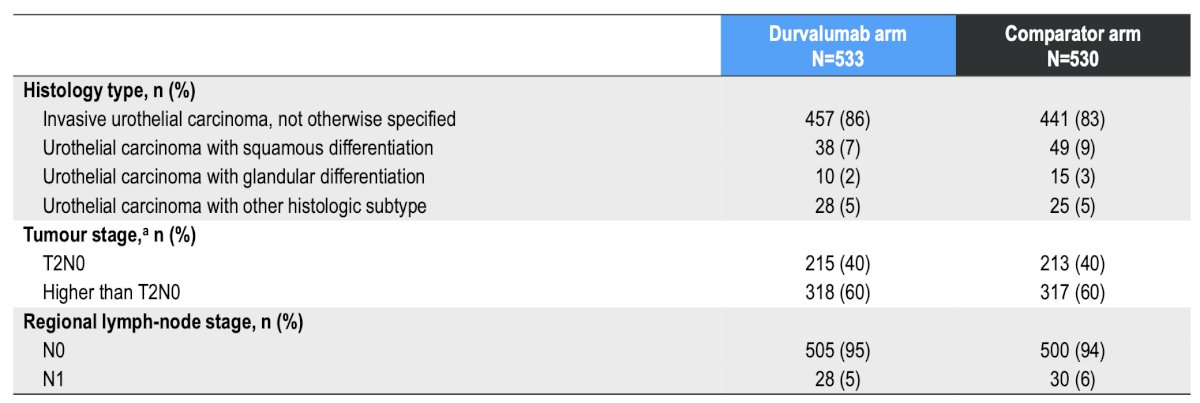
The focus of Dr. Catto’s EAU 2025 presentation was assessing the ability and safety to undergo radical cystectomy. In NIAGARA, 88% of patients in the durvalumab arm versus 83% in the comparator arm underwent radical cystectomy. Baseline tumor characteristics between the two arms were well balanced:
Similarly, the surgical characteristics between the two arms were comparable:
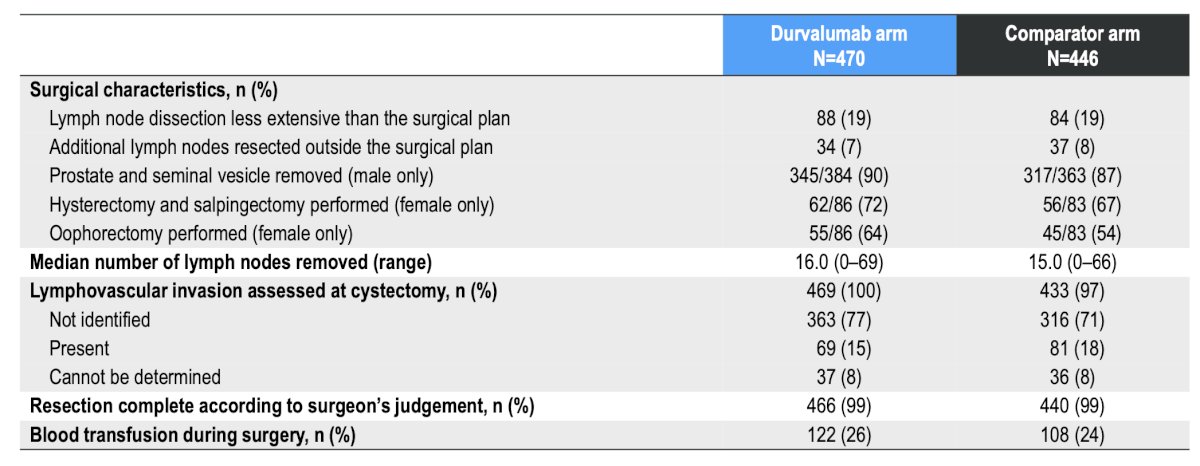
There was no difference in time to cystectomy between the study arms:
- The median time from last dose of neoadjuvant therapy to cystectomy was 5.6 weeks (range: 1.1-16.9) for the durvalumab arm versus 5.4 weeks (range: 1.7-47.6) for the comparator arm
- The median time from randomization to radical cystectomy was 16.3 weeks (IQR 14.7-18.4) for the durvalumab arm versus 16.1 weeks (IQR 14.3-18.3) for the comparator arm
- Patients undergoing cystectomy within 56 days after the last dose of neoadjuvant therapy included 90% in the durvalumab arm and 90% in the comparator arm
- Patients undergoing cystectomy within 70 days after the last dose of neoadjuvant therapy included 96% in the durvalumab arm and 95% in the comparator arm
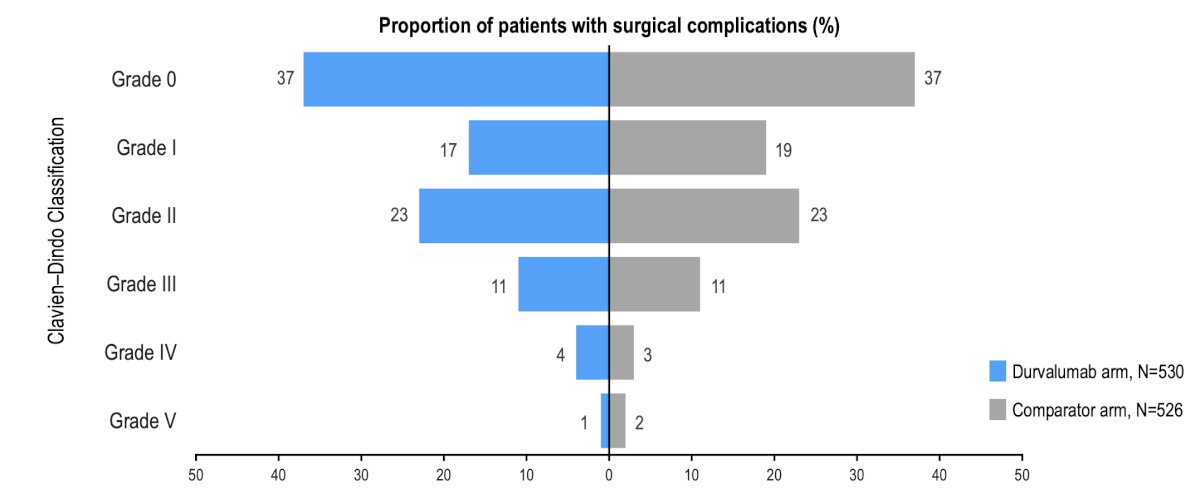
Rates of surgical complications by Clavien-Dindo classification were similar between the study arms:
Additionally, perioperative durvalumab + neoadjuvant chemotherapy was tolerable and manageable, with no new safety signals identified:
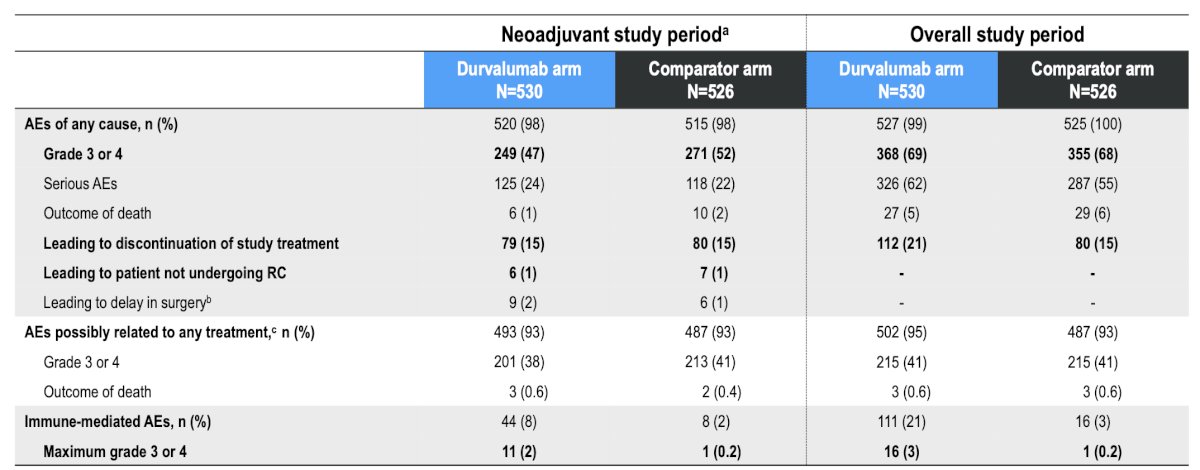
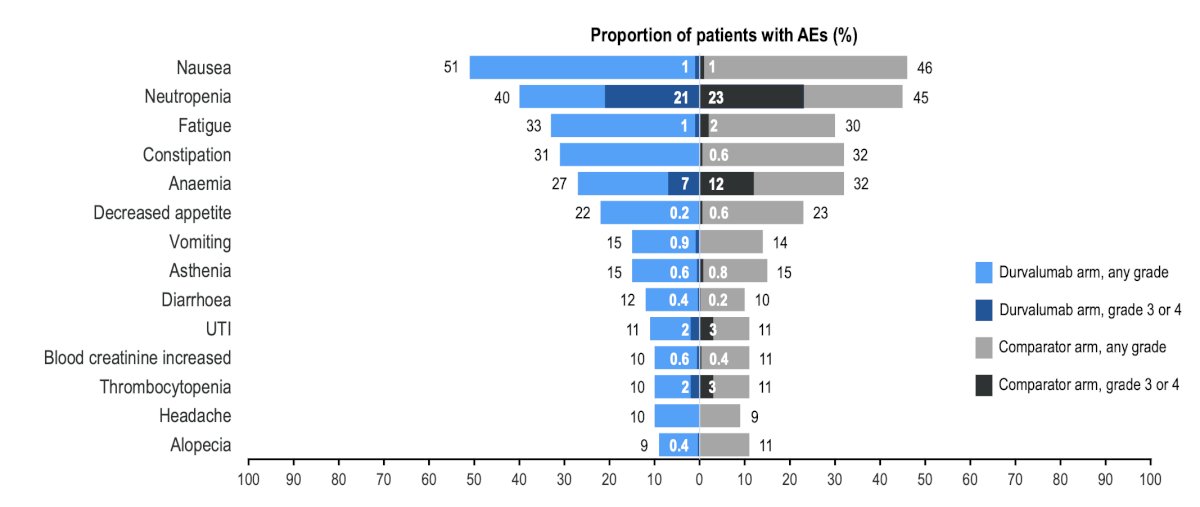
The adverse event profile in the neoadjuvant period was similar between the study arms, with the most common (>=10%) adverse events in each arm being nausea, neutropenia, and fatigue:
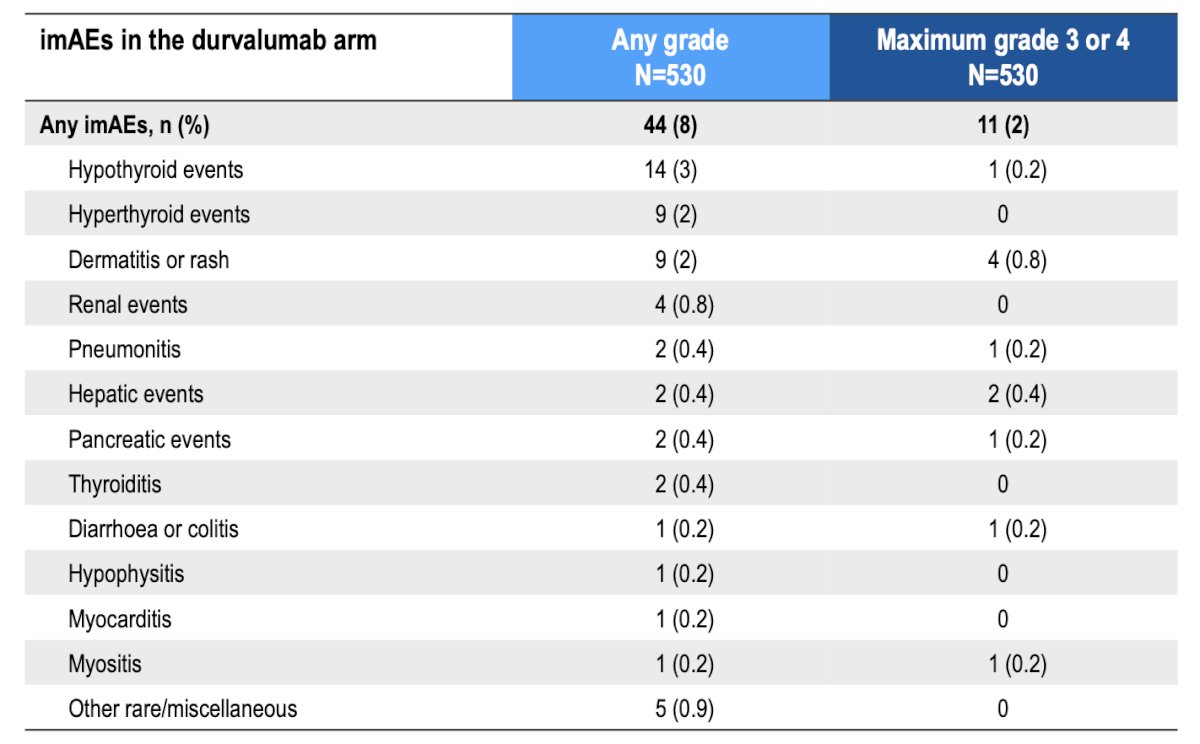
Immune mediate adverse events in the durvalumab arm were mostly low grade and consistent with the known safety profile of durvalumab. The median time to onset of hypothyroid events was 73.0 days (range: 29-141) and for hyperthyroid events was 38.0 days (range: 22-112), which Dr. Catto notes may be in the perioperative setting. The median time to dermatitis/rash was 4.0 days (range: 1-310) and for renal events was 25.5 days (range: 8-71), which is before the perioperative period:
Dr. Catto concluded his presentation by discussing surgical outcomes and neoadjuvant safety with perioperative durvalumab for muscle-invasive bladder cancer in the NIAGARA trial with the following take home points:
- NIAGARA demonstrated a statistically significant and clinically meaningful improvement in event free survival (HR 0.68, 95% CI 0.56-0.82) and overall survival (HR 0.75, 95% CI 0.59-0.93), with a 10% improvement in pathological complete response rate
- The addition of durvalumab to neoadjuvant chemotherapy did not impact the rate or timing of radical cystectomy, and did not increase the rate of surgical complications
- The adverse event profile in the neoadjuvant period was similar between study arms
- Immune mediated adverse events in the neoadjuvant period were mostly low grade and consistent with the known safety profile of durvalumab
- These additional NIAGARA data further support perioperative durvalumab with neoadjuvant chemotherapy as a potential new treatment for patients with cisplatin eligible muscle invasive bladder cancer
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References: