(UroToday.com) The controversies in onco-urology joint session of the ESOU, ERUS, ESMO, and ESTRO societies included a debate around whether we should perform PSMA PET/CT in the initial staging of prostate cancer.
Dr. Alexander Kretschmer from Munich, Germany started this session by presenting a case of a 65-year-old otherwise healthy male who had a screening PSA of 12 ng/mL and negative DRE. He then underwent an mpMRI that showed a PIRADS 4 (left anterolateral, no extracapsular disease) lesion, no suspect lymph nodes and no bone metastases. He subsequently underwent a fusion biopsy that showed 5 of 14 cores positive (including two target biopsy positive cores), Gleason 4+3, (60% pattern 4), ISUP 3 prostate adenocarcinoma. The patient then underwent a PSMA PET/CT as an initial staging procedure, which showed a PSMA positive focus in the left apex and base of the prostate, cN0, cM0. Ultimately, the patient proceeded with a robotic prostatectomy without pelvic lymph node dissection and pathological stage of pT3a, Gleason 4+3, pNx, R0. At 6 weeks postoperatively, his PSA was <0.03 ng/mL and he did not undergo adjuvant radiotherapy to the prostate bed or pelvic lymph nodes. 10 months from his surgery his PSA had increased to 0.27 ng/mL. He then had another PSMA PET/CT scan, which showed PSMA positivity in the right external iliac artery lymph node region. The patient ultimately proceeded with salvage radiation of the prostate bed and pelvic lymph nodes with a boost to the PSMA positive right iliac artery region.
Dr. Declan Murphy then took the pro approach for PSMA PET/CT for initial staging, emphasizing that PSMA PET/CT has established itself for its accuracy in regional disease, distant disease, and de novo and recurrent disease. To further illustrate his point, Dr. Murphy discussed the proPSMA prospective, randomized, multi-center clinical trial.1 To be eligible for inclusion in proPSMA, men must have had at least one high-risk factor including PSA >= 20 ng/mL, ISUP grade group 3-5, or clinical stage T3 or greater. Patients who had undergoing staging investigations (apart from prostate MRI) within eight weeks prior to randomization were excluded. Following enrollment, patients were randomly assigned in a 1:1 ratio to either conventional imaging performed using bone scan and CT or PSMA PET/CT. Patients who were randomized to conventional imaging underwent an abdominopelvic CT scan with contrast as well as a technetium-99m bone scan with SPECT CT of chest, abdomen, and pelvic in keeping with the standard of care. For patients randomized to PET/CT, gallium-68 PSMA-11 PET/CT was performed. In patients who had fewer than three unequivocal sites of metastasis, cross-over imaging for confirmation was performed within 14 days. Confirmatory testing following imaging was performed at the discretion of the treating physician and included biopsy confirmation.
Between 2017 and 2018, the trial randomly assigned 302 patients of whom 300 received assigned first-line imaging. In the primary outcome assessment, PSMA PET-CT had a 27% absolute greater AUC for accuracy compared to conventional imaging (95% CI 23-31): 92% (95% CI 88-95%) vs. 65% (60-69%):
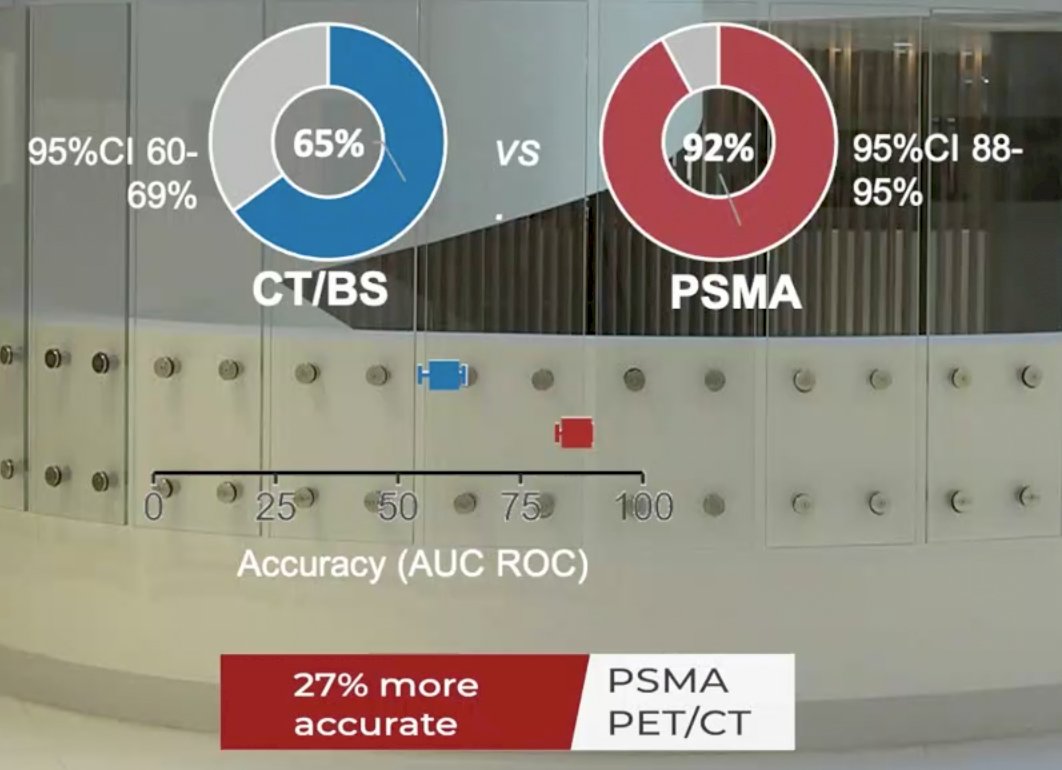
Conventional imaging had both a lower sensitivity (38% vs. 85%) and also a lower specificity (91% vs. 98%). Prior to treatment, the results of conventional imaging studies resulted in treatment change for 23 men (15%, 95% CI 10-22) while the results of PSMA PET-CT resulted in treatment change for 41 (28%, 95% confidence interval 21-36). These changes included both a transition from curative intent to palliative intent treatment in 20 patients (14%) and also a change in treatment approach in 22 (14%). Additionally, conventional imaging was associated with a higher radiation dose (19.2 mSv compared to 8.4 mSv; absolute difference 10.9 mSv, 95% CI 9.8-12.0 mSv0. PSMA PET-CT was not associated with any adverse events and reporter agreement was high for both nodal (kappa 0.87, 95% CI 0.81-0.94) and distant metastatic disease (kappa 0.88, 95% CI 0.94-0.92). Dr. Murphy notes that this patient likely had micrometastatic lymph node disease at the time of his robotic prostatectomy and he will now do very well with salvage treatment. Dr. Murphy concluded that the more accurate PSMA PET/CT for initial staging should replace the rather useless conventional imaging modalities we use to currently stage our patients.
Dr. Briganti then presented from the standpoint of no, we should not use PSMA PET/CT to initially stage high-risk patients. There are some certainties in prostate cancer staging, including PSMA PET/CT (i) is more accurate than conventional imaging, (ii) is more sensitive and specific than conventional imaging for primary staging, (iii) can miss micro-metastatic disease, and (iv) can lead to change in management in a significant proportion of men. However, Dr. Briganti states that it is unknown if better staging and change in management translates into better outcomes!
In view of the evidence from the proPSMA trial [1], the EAU guidelines suggest that replacing bone scan and abdominopelvic CT by PSMA PET/CT may be a consideration in patients with high-risk prostate cancer undergoing initial staging. However, in the absence of prospective studies demonstrating a survival benefit, caution must be used when discussing therapeutic decisions. The prognosis and ideal management of patients diagnosed as metastatic by these more sensitive tests are unknown.
Dr. Briganti then posed several questions/considerations with regards to the utilization of PSMA PET/CT for initial staging. First, should PSMA PET/CT be used for all patients? In a study by Kishan et al. (Eur Urol Oncol in press), 213 patients were included from two prospective trials with negative conventional imaging who underwent PSMA PET/CT. Overall, 90% of patients who had a nomogram-estimated risk below the cutoff of 22% for overall upstaging could have been spared a PSMA PET/CT as the model correctly predicted no upstaging. Dr. Briganti notes that, for example, if a patient has a nomogram calculated risk of 12% for lymph node involvement, the patient should have received an extended pelvic lymph node dissection regardless of PSMA PET/CT.
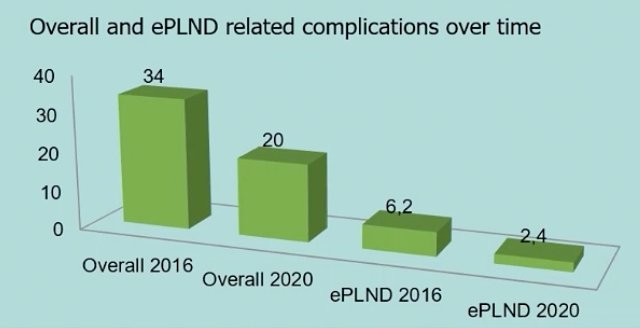
Second, PSMA-related clinical scenarios (N0 disease) – should we skip staging extended pelvic lymphadenectomy in the case of negative PSA PET/CT? According to Dr. Briganti, the answer is no, the overall sensitivity of PSMA PET/CT per node is 59% (and in high-risk patients is 54%). Furthermore, in men with unfavorable characteristics, approximately one in five patients would be erroneously deemed clinical node-negative based on unpublished data from Pellegrino et al. In data presented by Rosiello et al. at this meeting, the risk of major complications from an extended pelvic lymph node dissection has decreased substantially with time and more experienced robotic surgeons, thus the onus of an optimal staging procedure is not as great as perhaps it once was:
Dr. Briganti noted that as part of the trial design for proPSMA was a built-in health economics perspective published in European Urology.2 They found that the estimated cost per scan for PSMA PET/CT was AUD$1203, which was less than the conventional imaging cost at AUD$1412.
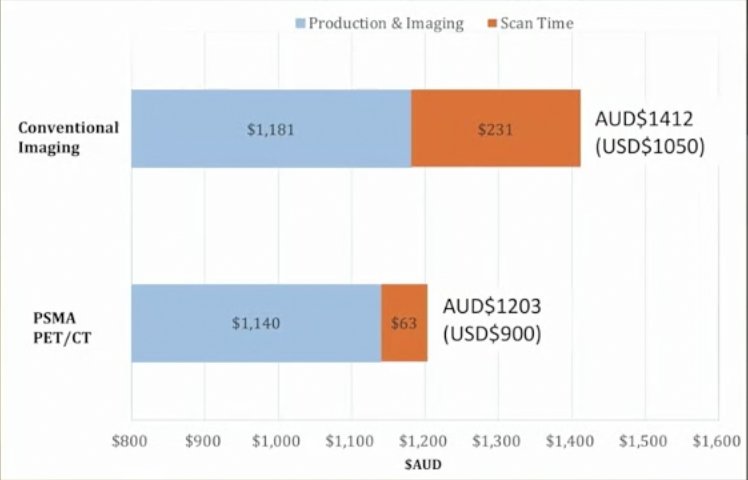
PSMA PET/CT was thus dominant, having both better accuracy and a lower cost, resulting in a cost of AUD$959 saved per additional accurate detection of nodal disease, and AUD$1412 saved for additional accurate detection of distant metastases. However, Dr. Briganti cautions that the unanswered question remains as to whether PSMA PET/CT maintains its higher cost effectiveness when repeated imaging and (potentially avoidable) salvage treatments are taken into account. Taking the current case into consideration, the patient had one unnecessary PSMA PET/CT at the time of staging, one potentially avoidable PSMA PET/CT at the time of recurrence, and one avoidable salvage treatment, all at the cost of saving one extended pelvic lymphadenectomy.
Dr. Briganti concluded that PSMA PET/CT for primary staging in 2021 is a sensitive approach, however, it currently raises more questions than it has answers.
Presented by: Declan Murphy, FRACS, FRCS, Peter MacCallum Cancer Centre, Melbourne, Australia; Alberto Briganti, San Raffaele, Milan, Italy
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 European Association of Urology, EAU 2021- Virtual Meeting, July 8-12, 2021.
References:
- Hofman MS, Lawrentschuk N, Francis, RJ, et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomized, multicentre study. Lancet 2020 Apr 11;395(10231):1208-1216.
- De Feria Cardet RE, Hofman MS, Segard T, et al. Is Prostate-specific Membrane Antigen Positron Emission Tomography/Computed Tomography Imaging Cost-effective in Prostate Cancer: An Analysis Informed by the proPSMA Trial. Eur Urol. 2020 Dec 16;S0302-2838(20)30946-5.