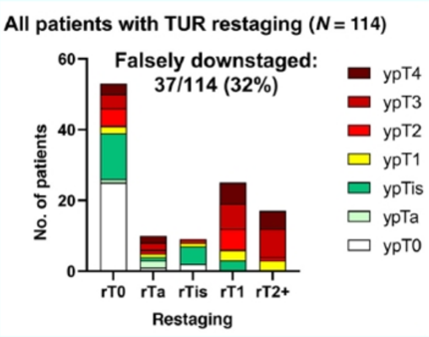
A recent publication from Becker et al.1 evaluated the ability of post-neoadjuvant chemotherapy clinical restaging, with or without tumor sequencing, to predict final radical cystectomy pathologic staging. Among 114 patients that underwent restaging TUR following neoadjuvant chemotherapy prior to radical cystectomy, the diagnostic accuracy of post-neoadjuvant chemotherapy clinical restaging including TUR was poor, with 32% of patients being downstaged falsely when compared with their final cystectomy pathology:
Dr. Witjes notes that the undetected non-responders to neoadjuvant chemotherapy do poorly. An NCDB population-level study from Pfail et al.2 analyzed differences in overall survival of patients with residual MIBC treated with neoadjuvant chemotherapy plus radical cystectomy, radical cystectomy alone, or radical cystectomy plus adjuvant chemotherapy. Among 8,288 patients included in the analysis, 1,899 (23%) received neoadjuvant chemotherapy plus radical cystectomy, 5,529 (67%) received radical cystectomy alone, and 860 (10%) received radical cystectomy plus adjuvant chemotherapy. >ypT2 disease after neoadjuvant chemotherapy was associated with significantly decreased overall survival compared to matched patients undergoing radical cystectomy alone or radical cystectomy plus adjuvant chemotherapy: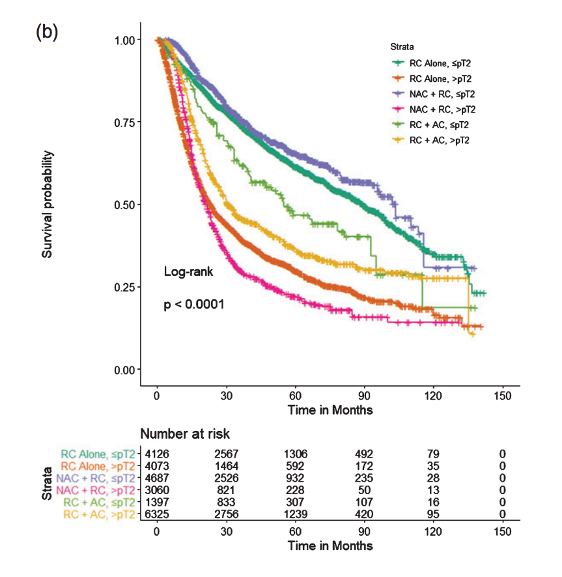
According to Dr. Witjes, the future will incorporate improved imaging modalities for detecting residual disease, biomarkers, and clinical trials. Yan et al.3 assessed the diagnostic performance of delayed 18F FDG PET/CT in the differentiation of residual tumors from postoperative inflammatory reactions in 79 patients with bladder cancer after initial TURBT. When compared with inflammatory reactions, residual tumors had higher mean standardized uptake value (SUVmean) (mean, 5.8 ± 2.0 vs 9.3 ± 5.4; P < .001), higher maximum standardized uptake value (SUVmax) (mean, 15.5 ± 9.8 vs 22.2 ± 13.6, P = .01), and greater lesion thickness (mean, 9.6 mm ± 4.1 vs 17.9 mm ± 11.1, P < .001) at 18F FDG PET/CT. Much has also been made of mpMRI and the VI-RADS scoring system for locally staging bladder cancer. Although mpMRI is not advocated for all patients with bladder cancer, bladder mpMRI may be most useful for differentiating between T1 and T2 bladder cancer and for determining response to chemo and bladder-sparing approaches.
With regards to biomarkers, several have been assessed for predicting neoadjuvant chemotherapy response. The ERCC2 alteration was found in 36% of responders (n=25) and 0% of non-responders (n=25), with a correlation with response and overall survival, both in discovery and validation datasets. Additionally, previous work has suggested that the basal subtype responds better to neoadjuvant chemotherapy, and defects in DNA repair genes also predict a better response to neoadjuvant chemotherapy.
Three current trials are of interest with regards to neoadjuvant chemotherapy, including the RETAIN trial (NCT02710734), the Alliance for Clinical Trials on Oncology (NCT03609216), and the phase II Hoosier Cancer Research Network trial (NCT03558087), which includes perioperative and postoperative nivolumab. Additionally, there is interest in using gene panels to enroll patients in a bladder-sparing active surveillance program after rT0 (or rTa or rTis) and neoadjuvant chemotherapy.
Dr. Witjes concluded his presentation with the following take-home messages:
- Bladder preservation can go well in highly selected patients, with a highly selected tumor, in a highly selected center, with a highly selected aggressive therapy and follow-up
- However, the loss (7% excess mortality) nullifies the gain of neoadjuvant chemotherapy (5-8%)
- cT0 after T2 and neoadjuvant chemotherapy: At the moment, radical cystectomy should still be the standard of care
Presenter By: J. Alfred Witjes, MD, Ph.D., Erasmus Medical Center, Nijmegen, Netherlands
Written By: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 European Association of Urology, EAU 2021- Virtual Meeting, July 8-12, 2021.
References:
- Becker REN, Meyer AR, Brant A, et al. Clinical restaging and tumor sequencing are inaccurate indicators of response to neoadjuvant chemotherapy for muscle-invasive bladder cancer. Eur Urol. 2021 Mar;79(3):364-371.
- Pfail JL, Audenet F, Martini A, et al. Survival of patients with muscle-invasive urothelial cancer of the bladder with residual disease at time of cystectomy: A comparative survival analysis of treatment modalities in the National Cancer Database. Bladder Cancer 2020;6(3):265-276.
- Yan H, Zhou X, Wang X, et al. Delayed 18F FDG PET/CT Imaging in the Assessment of Residual Tumors after Transurethral Resection of Bladder Cancer. Radiology. 2019 Oct;293(1):144-150.
Read the Opposing Argument: EAU 2021: There Is No Role for Radical Cystectomy in cT0 After Neoadjuvant Chemotherapy: Yes