(UroToday.com) The joint session of the European Association of Urology (EAU) and the Maghreb Union Countries included a presentation by Dr. Maximilian Burger who discussed the main steps of an optimal transurethral resection of a bladder tumor (TURBT). Dr. Burger highlighted that the main steps to an optimal TURBT are to (i) appreciate the patient, (ii) appreciate the importance of the procedure, and (iii) appreciate the management that proceeds after the TURBT is performed.
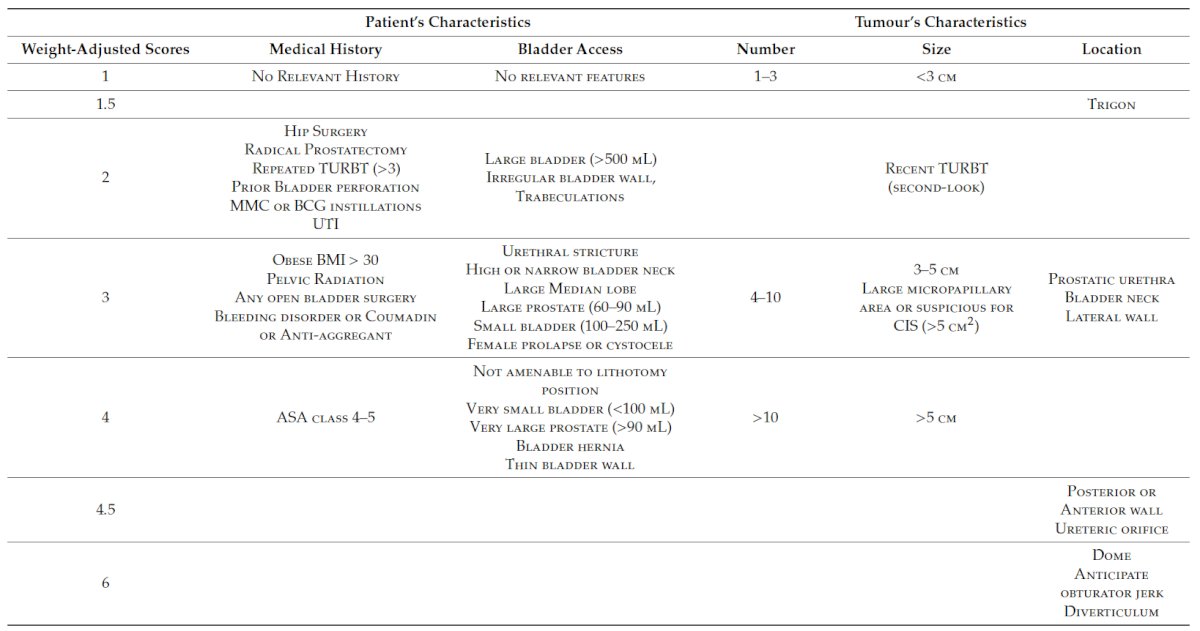
With regards to appreciating the patient, Dr. Burger makes reference to a recent publication by Roumiguie et al.1 predicting the complexity of TURBT for each patient. The five key domains for predicting complex TURBTs (ie. the Bladder Complexity Score) include the patient’s medical history, bladder access, number of tumors, tumor size, and tumor location. As follows is a table delineating the weight-adjusted scores for each domain:
In order to appreciate the procedure, the EAU guidelines highlight the importance of the procedure by stating that “the goal of TURB in TaT1 bladder cancer is to make the correct diagnosis and completely remove all visible lesions. It is a crucial procedure in the management of bladder cancer. Transurethral resection of the bladder should be performed systematically in individual steps. Specifically, the steps as outlined by the guidelines are as follows:

For each TURBT, surgeons must (i) perform an adequate resection, which is visually complete and down to muscle; (ii) recognize the presence of complications, such as perforation; (iii) measure the size of the largest tumor (the cutting loops as a reference is 1 cm); and (iv) comment on the characteristics of the tumor, such as nodular or papillary.
Thirdly, the surgeon must appreciate the management plan. As noted in the EAU guidelines, there are three risk groups of tumors, with specific definitions, and specific treatment recommendations, as follows:

Dr. Burger also notes that it is useful to use the EAU NMIBC risk calculator, which is available at nmibc.net, providing the probability of progression after TURBT without induction or maintenance BCG after appropriate clinicopathologic information.
Dr. Burger concluded by once again highlighting that each TURBT should include an assessment of the complexity of the procedure, an appreciation of a quality procedure, and realizing that this information must be formulated into a comprehensive management plan.
Presented by: Maximilian Burger, MD, St. Josef Medical Center, University of Regensburg, Regensburg, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 European Association of Urology, EAU 2021- Virtual Meeting, July 8-12, 2021.
References:
- Roumiguie M, Xylinas E, Brisuda A, et al. Consensus definition and predicting complexity in transurethral resection or bladder endoscopic dissection of bladder tumours. Cancers (Basel). 2020 Oct 20;12(10):3063.