(UroToday.com) As part of a plenary presentation at the European Association of Urology (EAU) Virtual 2020 meeting assessing “Testis cancer and surgical andrology,” Marij Dinkelman-Smit, PhD, outlined an approach to testicular microlithiasis and germ-cell neoplasia in situ (GCNIS).
Dr. Dinkelman-Smit began by highlighting that cure rates for testicular cancer are high following orchiectomy with or without adjuvant therapy as indicated. This paradigm is well established; however, the role of screening of the contralateral testicle with identification of testicular microlithiasis or GCNIS is fraught with significant uncertainty regarding optimal treatment with options including surveillance, orchiectomy, radiotherapy, and chemotherapy. Thus, it leaves open the question of whether we should actively pursue the diagnosis of GCNIS, to offer preventative therapy, with the hopes of improving already high rates of cure.
Dr. Dinkelman-Smit then transitioned to an overview of testicular microlithiasis, which are calcium deposits within the seminiferous tubules, comprising hydroxyapatite core with concentric rings of cellular debris, glycoprotein, and collagen. The etiology is somewhat uncertain but hypothesized mechanisms including inflammation, defective phagocytosis by Sertoli cells, immune response, nanoparticles, or rapid cell turn over. However, she highlighted that testicular microlithiasis are not a precursor lesion for testicular cancer, not are they a causal factor for the development of testicular cancer.
Dr. Dinkelman-Smit highlighted that testicular microlithiasis is a common finding on scrotal ultrasound, present in 2.4-5.6% of asymptomatic men and up to 15% of symptomatic men. Testicular microlithiasis has been associated with testicular cancer, particularly among infertile men in observational cohort. However, there are significant issues with the heterogeneity of the data and shared risk factors.
She recommended a treatment approach driven by reassurance. As with all men, monthly self-examination should be recommended for men with microlithiasis. Ultrasound follow-up, in her estimation, is cost-ineffective. In particularly high-risk patients, biopsy may be considered to exclude GCNIS and cancer.
Transitioning to a discussion of GCNIS, Dr. Dinkelman-Smit highlighted that, unlike testicular microlithiasis, GCNIS may be a precursor lesion to testicular cancer as germ cell tumors are diagnosed in 50% of patients with GCNIS within 5 years and 70% within 7 years. This is an immunohistochemical diagnosis on the basis of testicular biopsy.
GCNIS may be diagnosed adjacent to existing testicular tumors, contralateral to known testicular tumors, and among patients undergoing testicular biopsy for other reasons.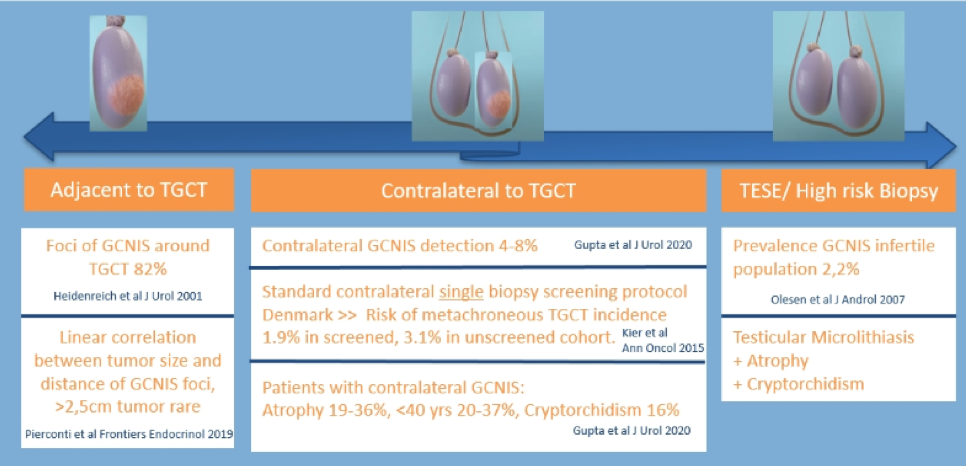
Treatment options for patients with GCNIS include preventative orchiectomy, radiotherapy, surveillance, or chemotherapy. Each of these options has strengths and weaknesses, on the basis of a balance of oncologic control and impairment in testicular function.
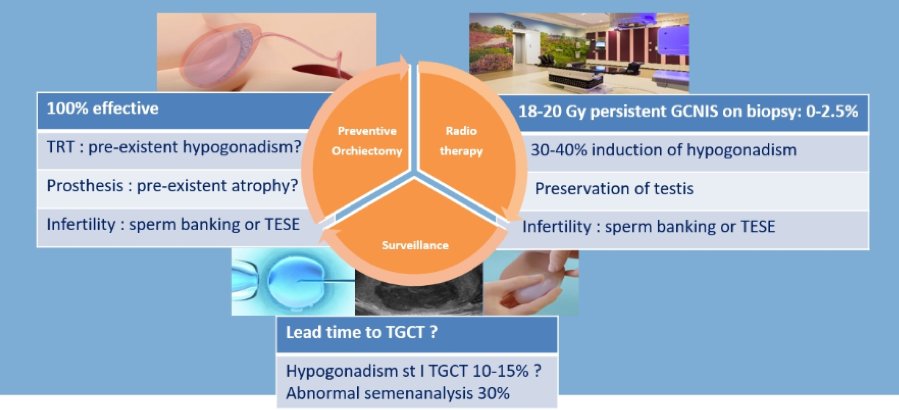
In patients who opt for chemotherapy, repeat biopsy to prove resolution of GCNIS is recommended with radiotherapy for those with persistent disease.
Presented by: Marij Dinkelman-Smit, PhD, Erasmus University Medical Center, Rotterdam, The Netherlands
Written by: Christopher J.D. Wallis, Urologic Oncology Fellow, Vanderbilt University Medical Center, Nashville, TN, USA, Twitter: @WallisCJD, at the Virtual 2020 EAU Annual Meeting #EAU20, July 17-19, 2020.