In bladder cancer, chronological age is of limited relevance. It is critical to assess the patient's comorbidities by validated scores of all elderly patients before deciding on the appropriate treatment of their muscle-invasive bladder cancer.
Previously published data have shown that older bladder cancer patients are less likely to receive standard treatment. However, the untreated disease will progress and severely impair the quality of life and the cancer-specific survival of these elderly patients. It is critical we consider the individual's life expectancy, his/her goals, and preferences. Clinical decision making must balance the benefits and risks of treatment against the morbidity and mortality arising from untreated or undertreated cancer.
Geriatric assessment in older cancer patients is required before choosing the appropriate management strategy. Screening with the G8 and mini-COG tests is recommended (Figures 1 and 2). As previously mentioned, no treatment should be denied based on age alone, and it is important to assess frailty using these tools to determine what treatment option is best. Additionally, especially in elderly patients, it is important to assess malnutrition with the ESPEN questionnaire, sarcopenia using the skeletal muscle index (SMI), and frailty with the fried frailty index.

Figure 1. Geriatric assessment
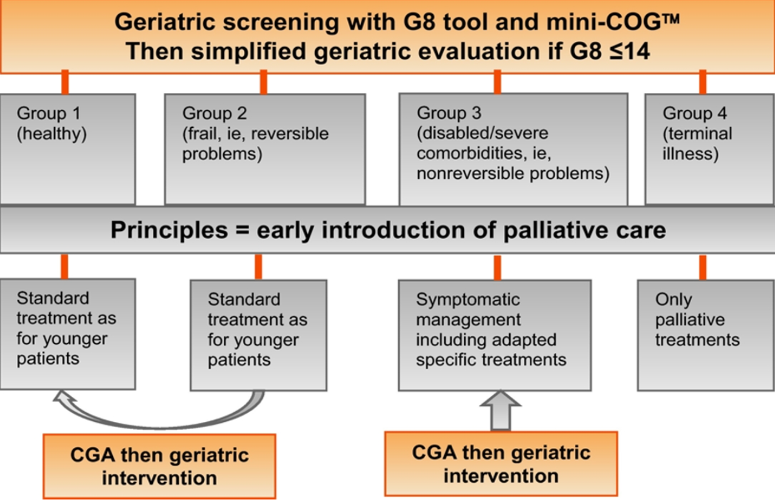
Figure 2. Geriatric screening with G8 tool and mini-COG and simplified geriatric evaluation if G8 ≤ 14
When deciding that palliative management is the best option, it should consist of the following:
- Monitoring patients and treating them according to their symptoms without applying oncological or invasive treatments during their follow-up
- These patients can be managed with analgesics, continuous saline bladder irrigation, or blood transfusion, but without oncological surgery, bladder instillations, radiotherapy, or chemotherapy
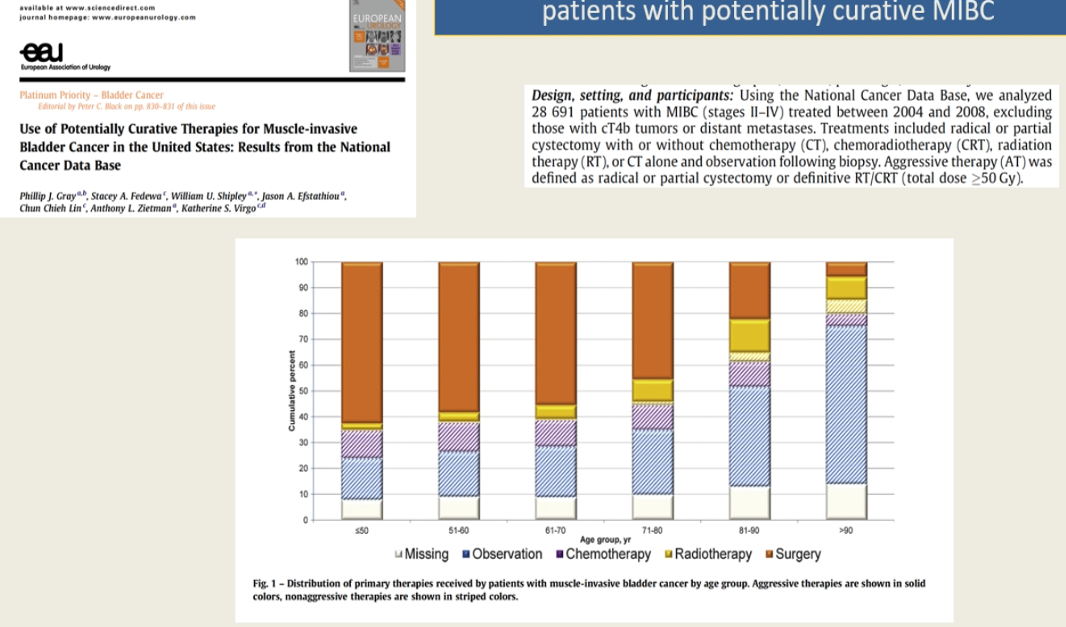
Figure 3. Use of potentially curative therapies for muscle-invasive bladder cancer in the US - results from the National Cancer Data Base
The current recommendations for radical therapy in localized disease in elderly patients include implementation of the ERAS® protocol, treating preoperative anemia, optimizing patients before surgery, the use of thromboprophylaxis, avoiding bowel reconstruction, and performing trimodal bladder sparing therapies and radical cystectomy in large referral centers. There is currently no data on the implications of avoiding lymph node dissection in elderly patients.
It is clear that there is extensive undertreatment of elderly patients according to the published data. These patients require proper staging before treatment, independent of their surgical fitness. These patients should be offered standard therapies, which include radical cystectomy and trimodal bladder sparing therapy. It is highly recommended that they are referred to large experienced centers for their treatments. If they are fit enough, it is suggested to consider neoadjuvant an adjuvant chemotherapy as well. Patients who are unfit for standard therapy should be considered for radiotherapy or transurethral resection of bladder tumor (TURBT) alone.
In elderly patients with metastatic bladder cancer, proper palliation should begin immediately following diagnosis. Standard therapy is cisplatin-based chemotherapy, carboplatin, or immunotherapy with checkpoint inhibitors. It is important to note that checkpoint inhibitors are tolerated in a similar fashion in young and elderly patients without more adverse effects noted in the elderly. Second-line immunotherapy treatments should be a standard treatment option in those progressing on cisplatin chemotherapy. Lastly, for gross hematuria or significant pain, palliative radiotherapy should be considered.
Dr. Maria José Ribal Caparrós mentioned that there is a lack of clinical trial data on the treatment of older adult bladder cancer patients. In order to help guide the choice of treatment in this unique patient population, efforts should be made to enroll these patients in controlled randomized trials and in studies assessing routine practice. Studies should include at least a minimum of geriatric data to provide a representative description of the older adult patients that are treated in the real world.
Presented by: María José Ribal Caparrós, MD, PhD, Medical Director, Serrate & Ribal Institute of Urology, Head, Multidisciplinary Urologic Oncology Unit, Hospital Clínic of Barcelona, Associate Professor of Surgery, University of Barcelona, Barcelona, Spain
Written by: Hanan Goldberg, MD, MSc, Urology Department, SUNY Upstate Medical University, Syracuse, New York, Twitter: @GoldbergHanan at the Virtual 2020 EAU Annual Meeting #EAU20, July 17-19, 2020