When such a recurrence is identified the therapeutic options include expectant management, androgen deprivation therapy (ADT), chemotherapy, abiraterone, enzalutamide, radiation therapy, and surgery. The EAU guidelines have a grade C recommendation regarding the role of salvage lymph node dissection (SLND) in men experiencing nodal recurrence after local treatment. However, it is still regarded as an experimental approach.
The largest series on SLND have shown a complete PSA response in 22%-73% of patients (Figure 1). A recently published study: Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial [1] analyzed 62 patients which were treated with surveillance or with a metastasis directed therapy for all metastatic lesions. At a median follow-up time of 3 years (interquartile range, 2.3-3.75 years), the median ADT-free survival was 13 months (80% CI, 12 to 17 months) for the surveillance group and 21 months (80% CI, 14 to 29 months) for the MDT group (hazard ratio, 0.60 [80% CI, 0.40 to 0.90]; log-rank P = .11) (Figure 2). Quality of life was similar between arms at baseline and remained comparable at 3-month and 1-year follow-up. The ideal patients for the SLND approach include patients with single or oligometastatic disease who demonstrate complete PSA response after surgery.
There is still debate whether the approach for SLND should be robotic or open. The multi-institutional SLND collaboration of EAU compared between open and robotic approach (Figure 3) showing a difference with shorter length of hospital stay and larger mean number of nodes removed for the robotically treated patients (Figure 4).
In conclusion, several institutions worldwide have embraced SLND for recurrent PC and data are slowly becoming mature. SLND represents a viable therapeutic approach for delaying clinical progression in nodal recurrence in prostate cancer. Current imaging is still underestimating the real extent of the disease. Lastly, the robotic approach may reduce the invasiveness of this surgical approach, but complications need to be considered when discussing with our patients.
Figure 1: Largest series of salvage of lymph node dissection
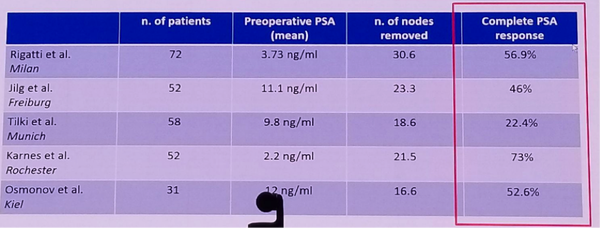
Figure 2: Clear advantage to the Metastasis directed therapy approach over surveillance:
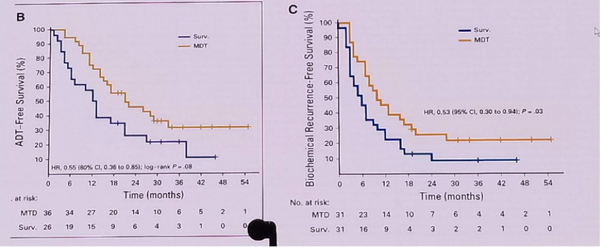
Figure 3: Comparison of open and robotic salvage lymph node dissection – perioperative outcomes:
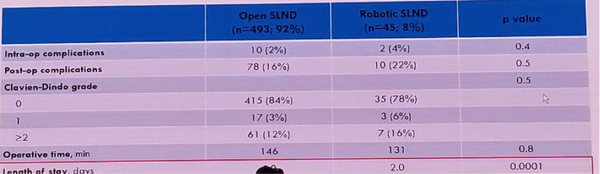
Figure 4: Comparison of open and robotic salvage lymph node dissection – Pathologic and oncologic outcomes:

Speaker: N. Suardi, Milan (IT), A. Heidenreich, Cologne (DE)
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, Twitter:@GoldbergHanan at the 2018 European Association of Urology Meeting EAU18, 16-20 March, 2018 Copenhagen, Denmark
Read More:
Against Robotic Assisted Salvage Lymphadencetomy