Data on CN is largely derived from retrospective analysis. The SURTIME is a study (EORTC30073) providing prospective data regarding CN. [1] The study randomized metastatic RCC patients to either immediate (and then systemic therapy) or deferred nephrectomy (after systemic therapy). The study faced poor accrual and therefore only 99 patients were recruited. Results demonstrated a progression free survival (PFS) and overall survival (OS) of 6.5 and 15 months respectively, for the immediate group, with a PFS and OS of 6.8 and 32.4 months, respectively for deferred CN. Landmark analysis showed a clear advantage for the deferred arm (Figure 1). These results show a clear survival advantage for the pre-surgical systemic therapy (Sunitinib) being clinically meaningful. Due to these results the EAU guidelines now recommend offering CN to intermediate risk patients with clear cell metastatic RCC who require systemic therapy with sunitinib.
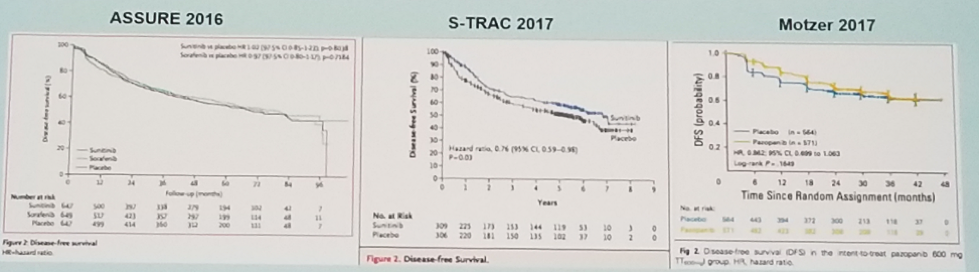
There have been 3 different trials assessing the benefit of adjuvant therapy in high risk RCC. The studies were different in their results due to the different high-risk population analyzed and the varying dosing of drugs (Figure 2). These included the ASSURE [2], S-TRAK [3], and Motzer [4]. Only S-TRAC showed a statistically significant benefit for adjuvant therapy in disease free survival, while the other 2 studies did not show a benefit. All studies did not show an OS benefit.
Currently there are planned studies to assess the impact of immune checkpoint inhibitors as adjuvant treatment in high risk RCC. These include the IMmotion 010, Keynote-564, and Checkmate 914.
The IMmotion 151 compared Atezolizumab (ATEZ) and Bevacizumab (BEV) to Sunitinib in metastatic treatment naïve RCC patients with clear cell and/or sarcomatoid histology. The results demonstrated a complete response of 9% vs. 4% in ATEZ + BEV vs. Sunitinib, respectively, and a partial response of 34% vs. 30% in ATEZ + BEV vs. sunitinib, respectively. No clear benefit was shown in OS, although data is still immature. Checkmate 214 compared Nivolumab (NIV) + Ipulimumab (IP) to sunitinib in treatment naïve metastatic RCC patients. Results showed a clear benefit in OS and PFS for the NIV+IP. Lastly, the CABOSUN trial compared CABOZANTINIB (CAB) to Sunitinib in patients with advanced measurable RCC disease. The results showed a clear advantage in PFS in favor of CAB, with a ratio of 0.48, p=0.0008.
More studies are being planned and the field is growing immensely, with different treatment options being assessed including monotherapy and various combination trials.
Figure 1: Landmark analysis showing benefit for the deferred approach of cytoreductive nephrectomy:
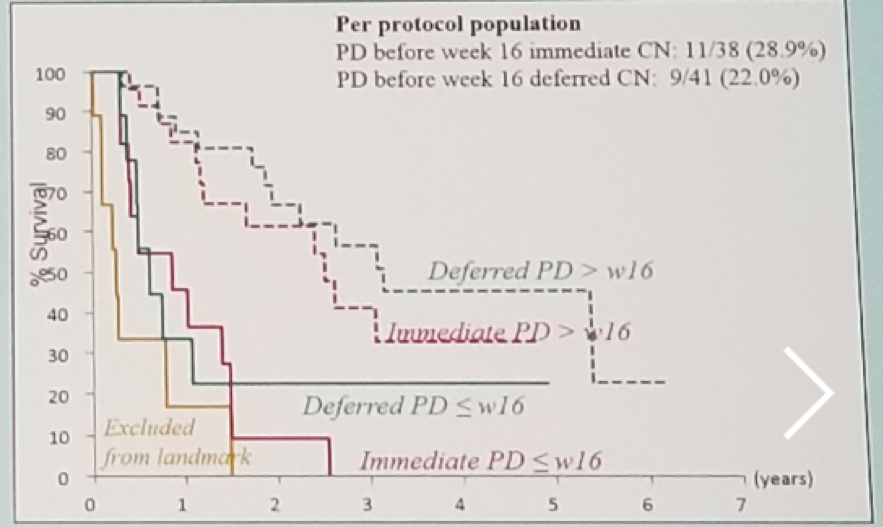
Figure 2: Disease free survival in the different adjuvant treatment for high risk patients:
Presented by: J. Bedke, MD, Tübingen, Germany
References:
[1] Bex A et al. ESMO 2017
[2] Haas N T et al. Lancet 2016
[3] Ravaud et al. NEJM 2016
[4] Motzer RJ et al. JCO 2017
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, twitter: @GoldbergHanan at the 2018 European Association of Urology Meeting EAU18, 16-20 March, 2018 Copenhagen, Denmark