There is clear evidence with multiple prospective randomized controlled trials demonstrating a survival advantage resulting from neoadjuvant chemotherapy for all eligible patients with muscle-invasive bladder cancer. However, only 40% of patients show a major response and appear to benefit from neoadjuvant chemotherapy. Additionally, neoadjuvant chemotherapy is not commonly used in most parts of the world. The solution proposed for these two limitations is to use a marker which would help us recognize which patient is likely to respond to neoadjuvant chemotherapy, and which patient would not benefit from it.
There are three markers which can be utilized as predictors of response to neoadjuvant chemotherapy:
- Molecular subtypes
- Co-eXpression ExtrapolatioN (COXEN) model
- Genomic alterations
Figure 1 – Bladder Cancer Molecular Subtypes:
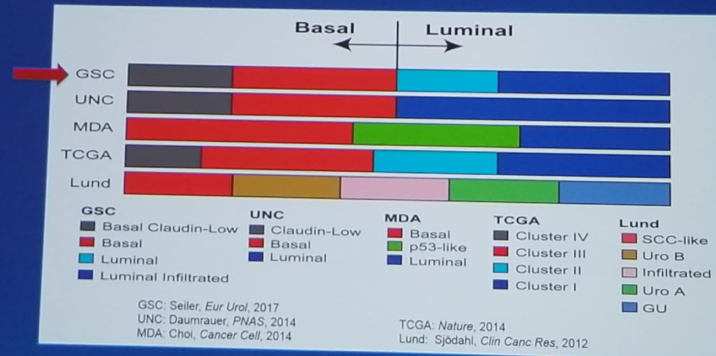
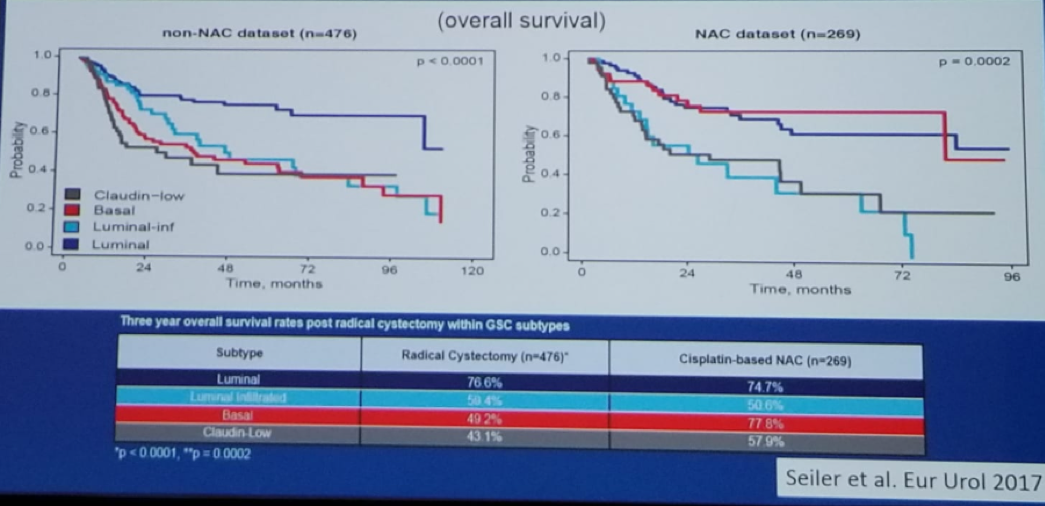
Figure 2 – Basal Tumors Are the Most Sensitive to Neoadjuvant Chemotherapy:
Next, Dr. Black explained briefly on the COXEN model, that helps us to construct a gene expression model from a large pool of genes, enabling us to have the smallest number of genes that when combined, offer the best correlation of expression with drug sensitivity.
Lastly, he mentioned some genomic alterations that might predict response to neoadjuvant chemotherapy. These include the ERCC2 mutations which have been shown to predict survival.1 Other genomic mutations with a similar effect include those of DNA repair genes (ATM, RB1, FANCC) – which are also associated with improved survival, following neoadjuvant chemotherapy.2
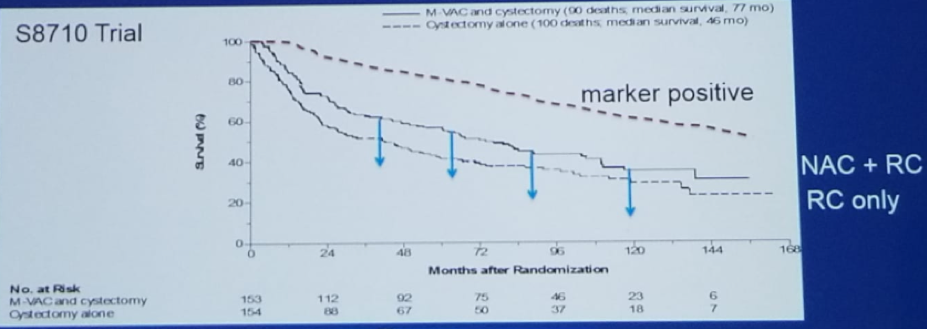
Dr. Black believes that using these methods to elucidate which patients would respond best to neoadjuvant chemotherapy, would result in the survival benefit seen with neoadjuvant chemotherapy to be significantly higher than if neoadjuvant chemotherapy is given to all patients in an “all or nothing” manner. There is no doubt that administering neoadjuvant chemotherapy to patients with a negative marker of response, lowers the survival benefit that could potentially be demonstrated with marker-positive patients (figure 3, 4).
Concluding his talk, Dr. Black summarized and stated that it is also important to remember, that neoadjuvant chemotherapy is not the only option, and patients can also receive adjuvant chemotherapy following radical cystectomy if decided upon.
The discussed markers should be used specifically to:
- Prioritize neoadjuvant chemotherapy in likely responders (“positive marker patients”)
- Expedite radical cystectomy in likely non-responders (“negative marker patients”)
- For those who believe markers have not been validated well enough, it is possible to proceed with the risk-adapted adjuvant chemotherapy following radical cystectomy.
Figure 3 – What Would Happen to the Neoadjuvant Arm in the Original Grossman et al. NEJM 2003 Trial if Marker-negative Patients Were Removed?

Figure 4 – What Would Happen to the Neoadjuvant Arm in the Original Grossman et al. NEJM 2003 Trial if Marker-positive Patients Were Removed?
Presented by: Peter Black, MD, FRCSC, Vice Chair, Medical Advisory and Research Board, University of British Columbia, Vancouver, British Columbia, Canada
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, Twitter: @GoldbergHanan at the CUOS – Canadian Uro-Oncology Summit 2019, #CUOS19 January 10-12, 2019 Westin Harbour Castle, Toronto, Ontario, Canada
References:
1. Liu et al. Jama Oncol 2016
2. Plimack et al. Eur Urol 2015
Further Related Content:
Neoadjuvant Chemotherapy for All Muscle-Invasive Bladder Cancer