(UroToday.com) The Bladder Cancer Advocacy Network (BCAN) Bladder Cancer Think Tank 2025 held in Washington, D.C., United States, between July 30th and August 1st. was host to the Session: Lessons Learned from Clinical Trials. Mr. Darrell Nakagawa discussed the importance of the patient’s perspective on the design of clinical trials for bladder cancer.
Mr. Nakagawa shared his powerful advocacy journey, which began during the early days of the HIV epidemic, when he served on the Board of Directors for the Montrose Counseling Center and observed firsthand how industry-funded clinical research at the time. Years later, in 2016, he was encouraged to participate in clinical trials himself. Initially treated for fatty liver, he was later evaluated for microhematuria, undergoing MRI, CT, and ultimately a TURBT that revealed non–muscle-invasive bladder cancer. He was treated with mitomycin C and required a stent. As his disease progressed, he received neoadjuvant chemotherapy for muscle-invasive bladder cancer and was offered radical cystectomy just as his urologist was retiring. His care transitioned to Dr. Joshua Meeks, who performed the surgery.
Throughout treatment, Mr. Nakagawa remained highly engaged in his care, maintaining a positive attitude and committed to recovery, something he acknowledged is not always the case for every patient, a perspective he gained while walking daily on the urology ward. In October 2020, he was invited to attend the BCAN Think Tank, an experience he described as eye-opening, particularly in how the organization embraces patients as partners. Since then, he has become a dedicated patient advocate, serving with BCAN, the SWOG Cancer Research Network, the Lurie Cancer Center’s Scientific Review Panel, and as a participant in the AACR Survivor and Patient Advocacy Program, ensuring that patient voices are included in research and care conversations at the highest level.
Mr. Nakagawa spoke about the importance of patient-centered trial design, drawing from the NCI Concept Evaluation framework. He encouraged investigators to ask critical questions early in the process:
- How relevant is the study to patients currently living with or at risk of being diagnosed with the disease?
- What elements of the trial might attract or discourage patients and families?
- Are the risks, benefits, and burdens appropriately balanced from the patient and caregiver perspective?
He also stressed the importance of broadening eligibility criteria and assessing whether the trial is realistically designed to meet accrual and retention goals. Finally, he challenged researchers to consider practical patient-related factors, such as the clarity of informed consent, financial strain, impact on quality of life, and whether the study could disproportionately affect specific communities.
Mr. Nakagawa shared a few key lessons learned through his advocacy work. First, clinical trials benefit immensely from patient advocate involvement not just as advisors, but as active partners. He encouraged investigators to leverage the patient advocates within BCAN, noting that many are eager to contribute meaningfully to trial development and execution. He praised BCAN as a medical organization that has evolved to fully integrate patient voices, including making advocates part of the Bladder Cancer Think Tank and giving them a seat at the table. Finally, he emphasized that patient care must be a dialogue, not a directive. Shared decision-making, he said, is fundamental to delivering respectful and effective care.
As outlined in the figure below, Mr. Nakagawa shared key observations and lessons learned from his advocacy experience. He emphasized the importance of engaging patient advocates throughout the NCI clinical trial lifecycle and praised BCAN as a model for integrating multidisciplinary voices, including urologists, medical and radiation oncologists, pathologists, advanced practice providers, and patient advocates. He underscored that patient care must be a dialogue rooted in understanding, and that population disparities and practice-area differences must be acknowledged when designing inclusive trials. Central to all of this, he noted, is putting the patient first and recognizing the invaluable role of patient advocacy.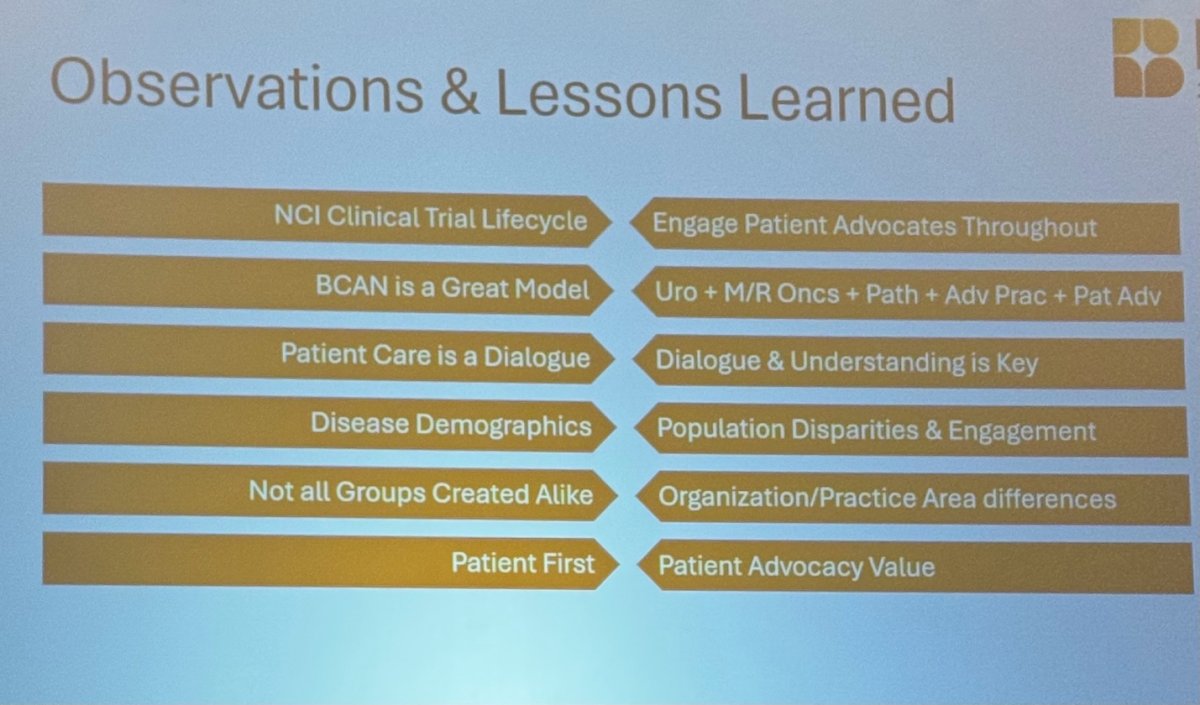
Lastly, Mr. Nakagawa encouraged clinicians and researchers to actively leverage the resources provided by BCAN, including BSCIs, webinars, podcasts, and the website, which he described as highly valuable and easily accessible for patients. These tools not only support education and empowerment but also help patients better understand their diagnosis and treatment options in a clear, patient-friendly way.
Presented by: Darrell Nakagawa, BCAN Patient Advocate, SWOG Bladder Cancer Patient Advocate
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the Bladder Cancer Advocacy Network (BCAN) Bladder Cancer Think Tank 2025 held in Washington, D.C., United States, between July 30th and August 1st
Related content: Strategies for Integrating Patient-Reported Outcomes in Urologic Oncology Research - Kelly Bree