(UroToday.com) The Bladder Cancer Advocacy Network (BCAN) Bladder Cancer Think Tank 2025, held in Washington D.C., United States, was host to the Session: Lessons Learned from Clinical Trials. Dr. Seth Lerner and Dr. Andrea Apolo co-chaired this session, bringing together expert panelists to reflect on key lessons learned from their involvement in bladder cancer clinical trials. Dr Andrea Apolo began by discussing insights from the Alliance A031501: AMBASSADOR study and gave advice on how to manage a cooperative group study in a rapidly evolving treatment landscape.
Dr. Apolo presented phase III AMBASSADOR study (NCT03244384), which evaluated adjuvant pembrolizumab versus observation in patients with high-risk muscle-invasive urothelial carcinoma of the bladder, ureter, or renal pelvis. Despite early concerns about patient dropouts and comparisons to the negative atezolizumab trial, the outcomes were positive. The study enrolled 739 patients randomized 1:1 to receive pembrolizumab (200 mg IV every 3 weeks for 1 year) or observation, with co-primary endpoints of disease-free survival (DFS) and overall survival (OS).1 These findings have led to the incorporation of adjuvant pembrolizumab into NCCN guidelines for high-risk MIBC, irrespective of prior neoadjuvant chemotherapy.

Notably, both PD-L1–positive and negative groups derived benefit from adjuvant pembrolizumab as illustrated below.

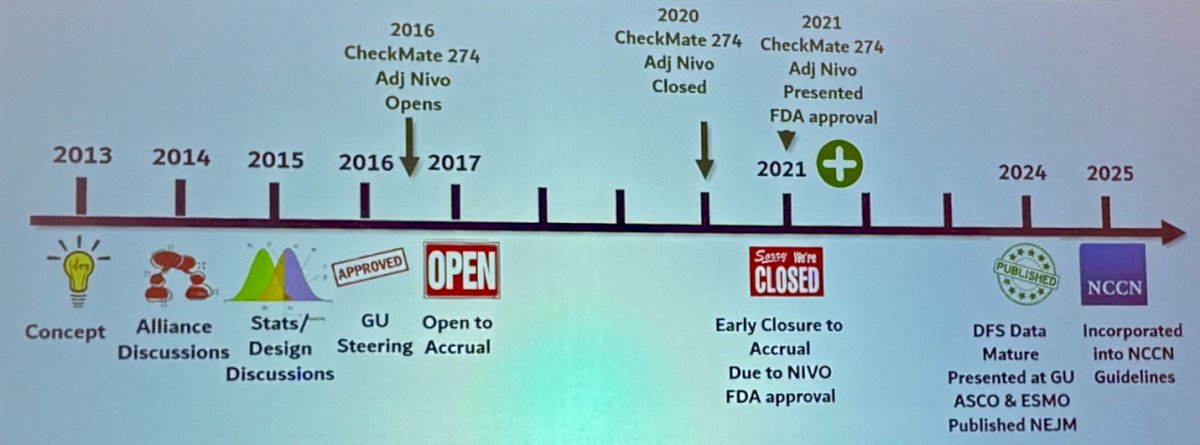
The timeline for the AMBASSADOR study began in 2013 with the initial concept, followed by alliance and statistical design discussions in 2014–2015. The trial received steering approval in 2016 and opened to accrual in 2017. In 2020, accrual was closed early due to the FDA approval of nivolumab in the adjuvant setting, making continued observation inappropriate. In 2021, results were presented, and the study received FDA approval. By 2024, disease-free survival data matured and were presented and published. In 2025, the study was incorporated into NCCN guidelines. The timeline of the study is illustrated below
Dr. Apolo highlighted that following the 2021 FDA approval of adjuvant nivolumab, continued observation in the control arm became inappropriate, prompting early closure of the study. The AMBASSADOR trial had co-primary endpoints: DFS and OS. Although DFS had matured, the co-primary design initially prevented reporting. A subsequent amendment allowed for DFS to be analyzed and shared independently.
At the time AMBASSADOR was enrolling patients, two other adjuvant IO trials were ongoing: IMvigor010, which was shockingly negative when reported in 2020 (a major disappointment for anyone running an adjuvant IO study), and CheckMate 274, which was strongly positive, nearly doubling DFS with adjuvant nivolumab.2,3
In 2023, enfortumab vedotin (EV) received FDA approval for the treatment of metastatic urothelial carcinoma based on the results of the phase III EV-302 trial, which demonstrated a significant survival benefit when combined with pembrolizumab. This combination has since emerged as the new standard of care for patients with advanced disease, offering an effective first-line treatment option regardless of cisplatin eligibility. Dr Apolo highlighted that arguably this could make adjuvant immunotherapy less desirable. However, in real-world clinical practice, the use of EV plus pembrolizumab is often extended to patients who have previously received adjuvant immune checkpoint inhibitors, despite the absence of prospective data in this specific population. The rationale for this approach stems from the distinct mechanisms of action of the two agents and the potential for synergistic antitumor activity.
In parallel, the NIAGARA trial, presented in 2024 and approved by the FDA in 2025, ushered in a new era of perioperative immunotherapy in muscle-invasive bladder cancer (MIBC). The study evaluated neoadjuvant durvalumab in combination with gemcitabine and cisplatin followed by adjuvant durvalumab in patients with resectable MIBC. The trial met its primary endpoints, thereby establishing a new perioperative standard of care. Importantly, for patients who are ineligible for or do not receive this combined neoadjuvant and adjuvant approach, adjuvant immunotherapy alone, such as that studied in the AMBASSADOR trial, continues to represent a meaningful treatment option in high-risk MIBC.
Dr. Apolo concluded her presentation by outlining the key advantages and challenges of conducting a clinical trial in a rapidly evolving therapeutic landscape, as exemplified by her experience with the AMBASSADOR study. Among the major challenges, she emphasized the difficulty in planning an appropriate control arm when standards of care (SOC) are shifting, and the possibility that trials may need to halt enrollment prematurely if the SOC changes mid-study. She also noted the uncertainty around the clinical utility of incorporating biomarkers prospectively and the concern that trial findings may become less relevant if surpassed by new therapies.
Despite these challenges, she highlighted the significant rewards of leading such studies: the invaluable learning experience, the opportunity to make a substantial impact on patient care, the critical importance of the clinical data generated, and the value of the biospecimens collected, which may serve future research well beyond the scope of the original study.
Presented by: Andrea Apolo, MD, Medical Oncologist and Senior Investigator at the National Institutes of Health (NIH).
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the Bladder Cancer Advocacy Network (BCAN) Bladder Cancer Think Tank 2025 held in Washington D.C., United States, between July 30th and August 1st.
Reference:
- Apolo AB, Ballman KV, Sonpavde G, Berg S, Kim WY, Parikh R, Teo MY, Sweis RF, Geynisman DM, Grivas P, Chatta G, Reichert ZR, Kim JW, Bilen MA, McGregor B, Singh P, Tripathi A, Cole S, Simon N, Niglio S, Ley L, Cordes L, Srinivas S, Huang J, Odegaard M, Watt C, Petrylak D, Hoffman-Censits J, Wen Y, Hahn O, Mitchell C, Tan A, Streicher H, Sharon E, Moon H, Woods M, Halabi S, Perez Burbano G, Morris MJ, Rosenberg JE. Adjuvant Pembrolizumab versus Observation in Muscle-Invasive Urothelial Carcinoma. N Engl J Med. 2025 Jan 2;392(1):45-55. doi: 10.1056/NEJMoa2401726. Epub 2024 Sep 15. PMID: 39282902; PMCID: PMC11698643.
- Bellmunt J, Hussain M, Gschwend JE, Albers P, Oudard S, Castellano D, Daneshmand S, Nishiyama H, Majchrowicz M, Degaonkar V, Shi Y, Mariathasan S, Grivas P, Drakaki A, O'Donnell PH, Rosenberg JE, Geynisman DM, Petrylak DP, Hoffman-Censits J, Bedke J, Kalebasty AR, Zakharia Y, van der Heijden MS, Sternberg CN, Davarpanah NN, Powles T; IMvigor010 Study Group. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2021 Apr;22(4):525-537. doi: 10.1016/S1470-2045(21)00004-8. Epub 2021 Mar 12. PMID: 33721560; PMCID: PMC8495594.
- Galsky MD, Witjes JA, Gschwend JE, Milowsky MI, Schenker M, Valderrama BP, Tomita Y, Bamias A, Lebret T, Shariat SF, Park SH, Agerbaek M, Jha G, Stenner F, Ye D, Giudici F, Dutta S, Askelson M, Nasroulah F, Zhang J, Brophy L, Bajorin DF. Adjuvant Nivolumab in High-Risk Muscle-Invasive Urothelial Carcinoma: Expanded Efficacy From CheckMate 274. J Clin Oncol. 2025 Jan;43(1):15-21. doi: 10.1200/JCO.24.00340. Epub 2024 Oct 11. PMID: 39393026; PMCID: PMC11687940.