(UroToday.com) The Bladder Cancer Advocacy Network (BCAN) Bladder Cancer Think Tank 2025 held in Washington D.C., United States, was host to the Session: Lessons Learned from Clinical Trials. Dr. Jeannie Hoffman-Censits discussed EA8192 for upper tract urothelial carcinoma (UTUC), highlighting how cooperative group trials in rare tumors can serve as powerful platforms for both scientific leadership and career development.
Dr. Hoffman-Censits, reflecting on her early career, shared that during her first role out of fellowship, she saw a striking number of patients with upper tract urothelial carcinoma (UTUC). Building on the ECOG-ACRIN 8141 trial—which evaluated neoadjuvant systemic chemotherapy followed by surgery in high-grade UTUC—she proposed what would become ECOG/ACRIN EA8192, a pivotal phase II/III trial (NCT04628767) now investigating the addition of durvalumab to perioperative chemotherapy.
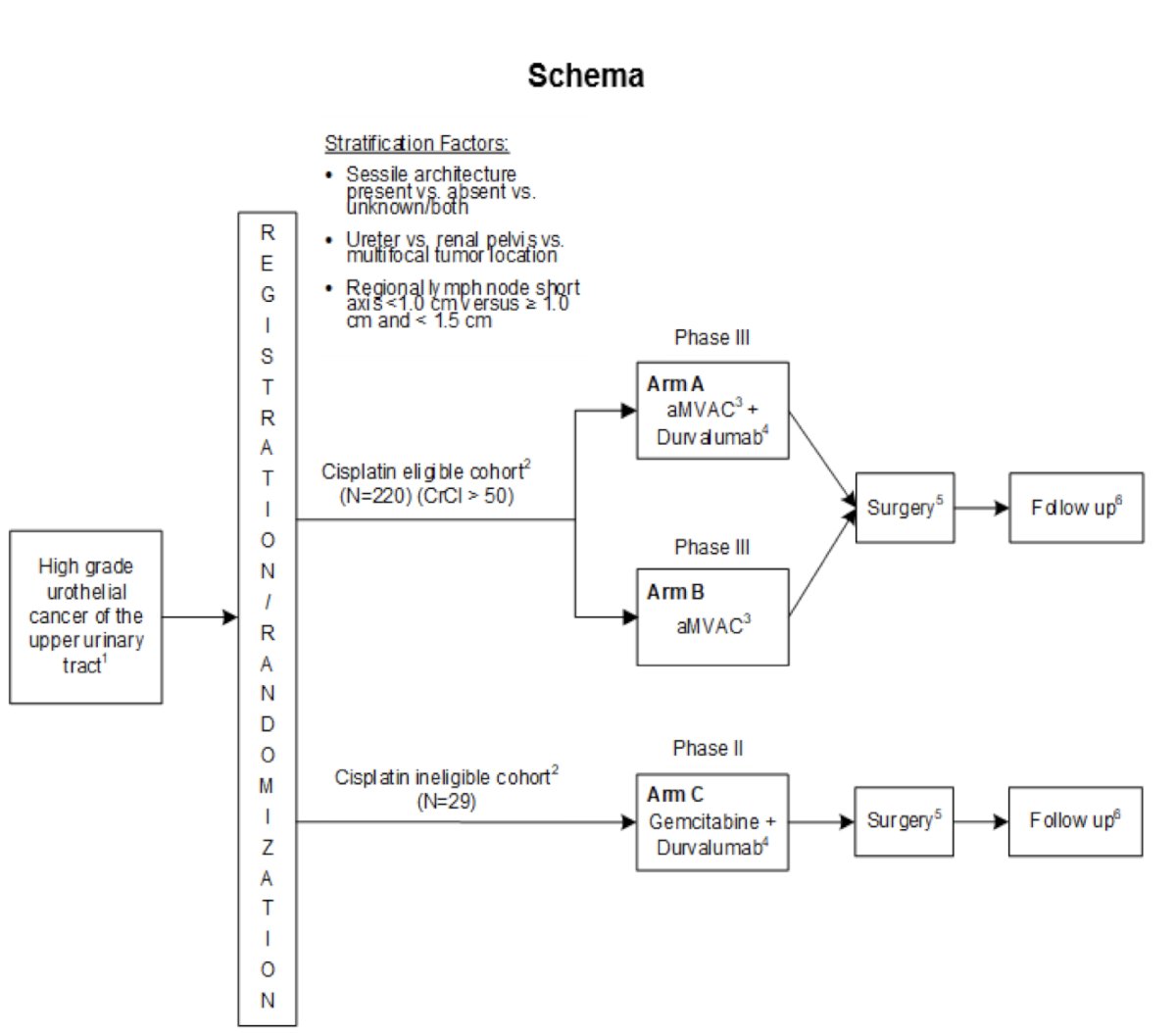
The EA8192 trial enrolls patients with high-grade upper tract urothelial carcinoma and stratifies them by tumor architecture, location, and lymph node characteristics. Cisplatin-eligible patients (CrCl >50) are randomized in the phase III portion to receive either accelerated MVAC with durvalumab or accelerated MVAC alone, followed by surgery and surveillance. Cisplatin-ineligible patients are enrolled in a separate phase II cohort and receive gemcitabine plus durvalumab before surgery. The trial aims to determine whether the addition of immunotherapy to neoadjuvant chemotherapy improves outcomes in this high-risk population. The study schema is shown below.
The concept of this trial was discussed years in advance during EORTC and ECOG-ACRIN 8141 planning meetings, laying the groundwork for EA8192. The final trial design emerged through multiple rounds of committee input and consensus. The core of the trial is the phase III comparison between accelerated MVAC alone versus MVAC plus durvalumab, with event-free survival (EFS) as the primary endpoint. Building on the EA8141 experience, which had a separate arm for platinum-ineligible patients, the EA8192 protocol also includes a cisplatin-ineligible cohort treated with gemcitabine and durvalumab allowing for a non–platinum-based neoadjuvant strategy in this population.
The development of EA8192 was a multi-year process shaped by iterative input across several cooperative group committees. The concept originated in late 2017, with early endorsement from ECOG and its sponsor, followed by NCI Bladder Taskforce review in 2018. Building on the feasibility shown in the precursor EA8141 trial, the team submitted a revised eligibility and design proposal including a pCR endpoint—for ECOG-ACRIN executive committee review, which approved the redesigned phase II/III concept in September 2019.
From there, the protocol underwent multiple rounds of review, including GUSC, NCI, CTEP, and internal ECOG assessments between 2019 and 2020. Notably, EA8186 was withdrawn during this period to streamline development. A key lesson learned was that once a cooperative group study enters broader steering committee review, the final version can evolve substantially from the original vision. The mandate for tissue collection, driven by the need to support biomarker development, was non-negotiable emphasizing the growing role of translational science in cooperative group trials. Final protocol approval and activation occurred in early 2021.
Conducting a trial in UTUC comes with inherent challenges, given the rarity of the disease. One major hurdle for EA8192 was the requirement for mandatory biopsy, which slowed accrual. Compounding this, the POUT trial supporting adjuvant chemotherapy was published in 2020, just before EA8192 opened, making neoadjuvant enrollment an uphill battle as patients and clinicians increasingly leaned toward post-operative treatment. Despite this, the trial remains active, and accrual has recently picked up pace as illustrated below. Discussions continue around whether regimens like NIAGARA could have a role in UTUC as well, highlighting the dynamic nature of treatment planning in this space.
Dr. Hoffman-Censits concluded her presentation with the following lessons learned and opportunities:
- Patience is essential when navigating cooperative group processes
- Expanding eligibility criteria, such as including patients with positive cytology, can help boost accrual
- Emerging data supporting alternative regimens can be leveraged to strengthen trial enrollment
- For EA8141 and similar studies, it's critical to discuss authorship early and transparently to ensure alignment and avoid conflicts later in the process
Presented by: Jean Heather Hoffman-Censits, MD, Assistant Professor of Oncology, Co-Director, Women’s Bladder Cancer Program, Greenberg Bladder Cancer Institute, Co-Director, Upper Tract Urothelial Cancer Multidisciplinary Clinic, Johns Hopkins University, Baltimore, MD
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the Bladder Cancer Advocacy Network (BCAN) Bladder Cancer Think Tank 2025 held in Washington D.C., United States, between July 30th and August 1st.
Reference:
- Margulis V, Puligandla M, Trabulsi EJ, Plimack ER, Kessler ER, Matin SF, Godoy G, Alva A, Hahn NM, Carducci MA, Hoffman-Censits J; Collaborators. Phase II Trial of Neoadjuvant Systemic Chemotherapy Followed by Extirpative Surgery in Patients with High Grade Upper Tract Urothelial Carcinoma. J Urol. 2020 Apr;203(4):690-698. doi: 10.1097/JU.0000000000000644. Epub 2019 Nov 8. PMID: 31702432; PMCID: PMC7735436.