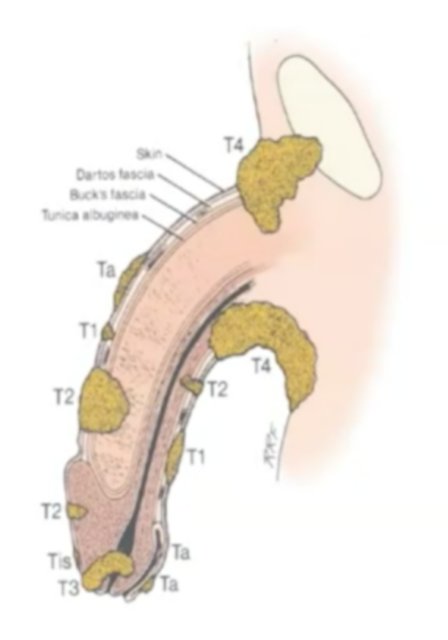
(UroToday.com) At the 2021 American Urological Association (AUA) Summer School session on the updates in the management of penile cancer, Dr. Timothy A. Masterson from Indiana University discussed local management of the penile primary tumor. Dr. Masterson started by highlighting that local recurrences occur secondary to surgical technique, pathological stage, and surgical margin status. This also has an impact on surveillance, salvage therapy options, and survival. With regards to the location of primary lesions, 85-95% involve the glans and the prepuce (glans 50-60%; prepuce 20%; glans plus prepuce 9%), with an additional 6% on the coronal sulcus and <5% on the shaft of the penis. According to the TNM classification of penile cancer’s 8th edition update (2018), the T stage classification is as follows:
- Tis carcinoma in situ
- Ta non-invasive verrucous carcinoma
- T1 tumor invades subepithelial connective tissue
- T1a is not poorly differentiated, with no lymphovascular invasion, and no perineural invasion
- T1b is poorly differentiated or with lymphovascular invasion, or with perineural invasion
- T2 tumor invades the corpus spongiosum +/- urethra
- T3 tumor invades the corpus carvernosa +/- urethra
- T4 invades other adjacent structures
Dr. Masterson notes that in the initial work-up of a penile cancer patient, lab evaluation should include a calcium level (to rule out hypercalcemia, which can be a para-neoplastic syndrome in penile cancer, secondary to PTH-like hormone-related factor), liver function tests, as well as radiographic evaluation with a CT of the abdomen/pelvis, chest x-ray, and possibly an MRI or bone scan or penile/groin ultrasound. Dr. Masterson then presented a case of a 48-year-old male with HIV and a nine-month history of a pink patch near the urethral meatus. The patient was referred to Dermatology where a shave biopsy was performed showing squamous cell carcinoma and a referral to Urology was made. According to the NCCN guidelines, there are several treatment options available to the patient, including topical therapy or wide local excision or laser therapy, or complete glansectomy.
There are several topical therapies available, including 5-fluorouracil, which has anti-cancer effects through the inhibition of thymidylate synthase and incorporation of its metabolites into RNA and DNA. For precancerous lesions, the dose is typically 0.5% or 1% cream/solution one to two times per day, and for cancerous lesions 5% cream/solution two times a day, with treatment continuing for several weeks. Side effects of 5-fluorouracil include redness, soreness, scaling, and peeling of affected skin after one to two weeks of use. A second topical therapy is imiquimod (Aldara), which is a 5% topical cream that activates the immune system through TLR-7, activating Langerhans cells, NK cells, B-cells, and macrophages, while releasing IFN-alpha, IL-6, and TNF-alpha. Dosing for imiquimod is once daily (6-8 hours) for 3-5 days/week, usually for 3-4 weeks, for a maximum of 16 weeks. Side effects include photosensitivity and hyperpigmentation, as well as avoiding use in those with immunodeficiency, cutaneous disorders, drug allergies, and pregnant-aged partners.
Several small, primarily retrospective studies have reported results for outcomes with local therapy. Alnajjar et al.1 previously reported their experience of 44 patients with carcinoma in situ treated with either 5-fluorouracil or imiquimod. They reported a complete response rate of 57% (n=25) and early side effects among 10% of patients. In a multi-center cohort analysis of 161 patients undergoing primary laser ablation as monotherapy, Tang et al.2 reported that over a median follow-up of 57.7 (IQR 28-90) months, the 5-year recurrence-free survival was 46%. When stratified by stage, the 5-year local recurrence-free survival was 50% for pTa/pTis, 41% for pT1a, 38% for pT1b, and 52% for pT2. Retreatment with laser ablation may also be feasible. Windahl and Andersson3 assessed 67 patients with primary penile cancer of which 13 patients had local recurrence and 10 had repeat laser treatment, with adequate local control (77% retreatment success) and cosmesis. In combination with our Dermatology colleagues, Mohs microscopic surgery is also feasible. In a single center assessment from Washington University, Shindel and colleagues4 identified 33 patients that underwent a total of 41 Mohs procedures. In this cohort, there were 26 carcinoma in situ patients, 4 T1, 7 T2, and 4 T3 patients. Over a median follow-up of 58 months, there was a 32% recurrence rate, with 7 patients being retreated with Mohs procedure and one patient undergoing a penectomy.
Referring back to the aforementioned case presentation, Dr. Masterson noted that after urology referral the patient underwent an excisional biopsy of the glans that showed squamous carcinoma in situ extending to the margin, and a repeat excisional biopsy of the glans six months later that showed carcinoma in situ of the meatus and a negative urethral margin. However, one year later, the patient had another recurrence and he underwent a partial glansectomy with squamous carcinoma in situ of the glans with urethral involvement. Since then he has had no evidence of disease on surveillance with an additional three years of follow-up.
Dr. Masterson then presented a second case of a 63-year-old male who presented with a six-month history of a penile mass with a urethral fistula. Initial management included a dorsal slit with a penile biopsy, a negative metastatic workup, and a urologic oncology referral. Dr. Masterson summarizes that from small studies assessing glansectomy for T1b (grade 3) and T2 lesions confined to the glans of the penis, local recurrence rates range from 0-4%. Albersen et al.5 retrospectively analyzed 117 patients at European high-volume centers that underwent glansectomy and glans reconstruction, noting that over a median follow-up period of 33.7 months (95% CI 26.8-40.3 months) 12.8% of patients had a local recurrence. Univariate Cox proportional hazards regression revealed that the risk factors for recurrence were the presence of perineural invasion, carcinoma in situ, positive margin on definitive pathology, and high-grade disease:
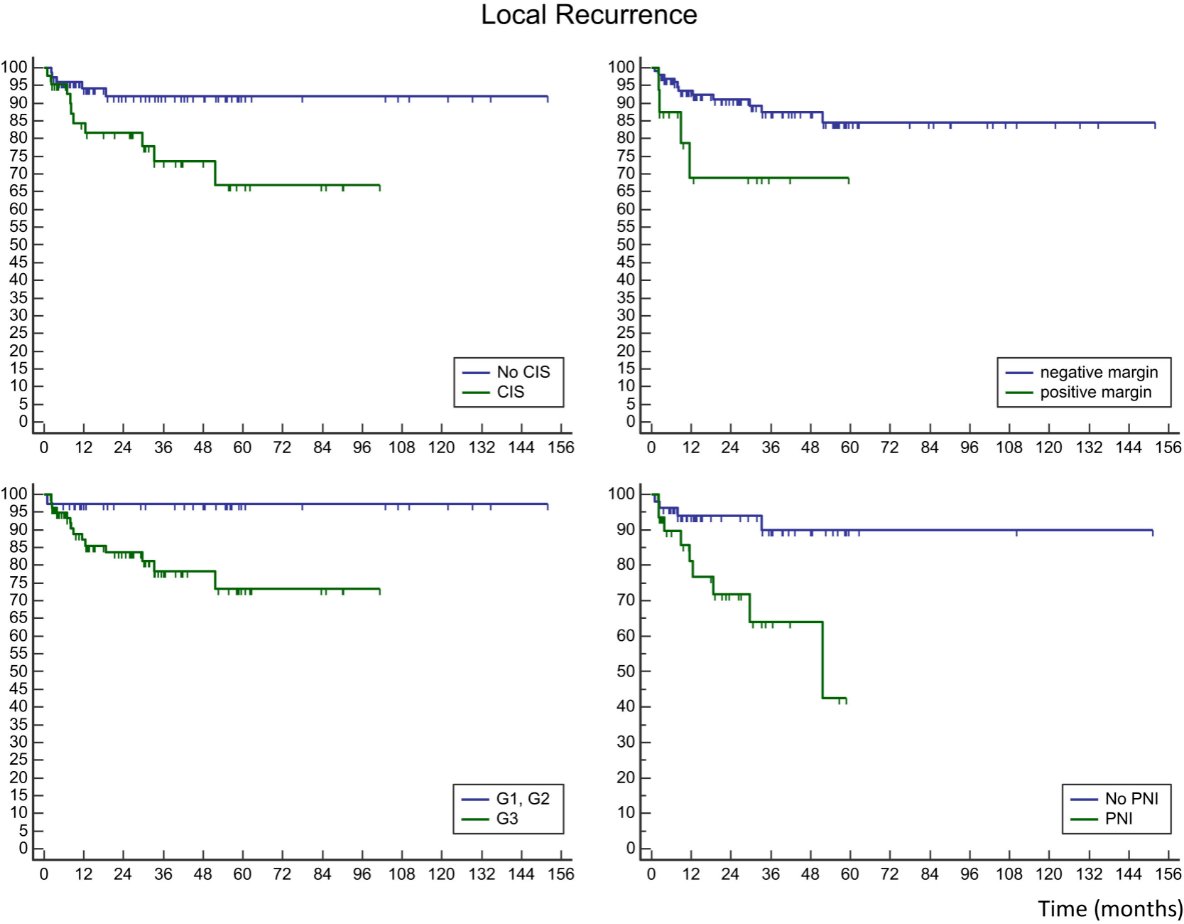
Based on these risk factors, Albersen and colleagues defined 3 risk groups for local recurrence: low (0-1 risk factors) as reference, intermediate (2-3 risk factors) with HR of 13.9 (95% CI 1.81-107.04), or high risk (all 4 risk factors present) with a HR of 34.2 (95% CI 3.07-381.81)

Summarizing the literature, Dr. Masterson highlighted that partial penectomy for pT2/pT3 penile cancer results in a local recurrence rate of 3.5%
Radiotherapy as primary therapy has also been assessed for penile cancer with varying results. Dr. Masterson notes that for brachytherapy (for <4 cm, superficial tumors), the 5-year local control rate is 70-87% and the 5-year penile preservation rate is 72-88%. For external beam therapy for more advanced tumors, the 5-year local control rate is 41-70% and the 5-year penile preservation rate is 36-66%. Complications of radiotherapy for penile cancer include soft tissue necrosis (~23%), urethral stricture (10-45%), and erectile dysfunction.
The aforementioned patient in the case presentation subsequently underwent a partial penectomy with pathology noted as T3, well-differentiated squamous cell carcinoma, positive for corpus cavernosum and spongiosum invasion, negative for lymphovascular invasion, with focally positive margins. He then underwent a completion penectomy and bilateral inguino-femoral lymphadenectomy two months later with pathology pT0N0. He is currently with no evidence of disease after 36 months of follow-up.
Dr. Masterson then discussed additional studies assessing predictors of recurrence and the impact of survival outcomes. A study from the high-volume St. George’s Hospital in London, UK assessed the significance of close surgical margins in organ-sparing surgery among 332 patients in the treatment of penile squamous cell carcinoma, and clinicopathological factors that may influence local recurrence among.6 There were 64% of patients that had a <5 mm clear deep surgical margin, with 16% clear by <1 mm. Overall, 4% of patients had a true local recurrence, with a median time to recurrence of 6 months. There was a statistically significant relationship between cavernosal involvement (p = 0.014) and lymphovascular invasion (p = 0.001) and local recurrence. Another UK study at a supraregional center for penile cancer assessed outcomes among 203 penile cancer patients, of which 18% had organ preservation surgery, and 4% had amputation surgery.7 They found that 94% of recurrences occurred during the first 3 years and surgical approach had no impact on survival, whereas cancer-specific survival was dictated by nodal/metastatic status. Finally, a study from the Netherlands reviewing an experience of 1,000 patients also assessed the impact of penile sparing surgery on survival. Over more than 50 years of experience, significantly fewer penile amputations were performed:
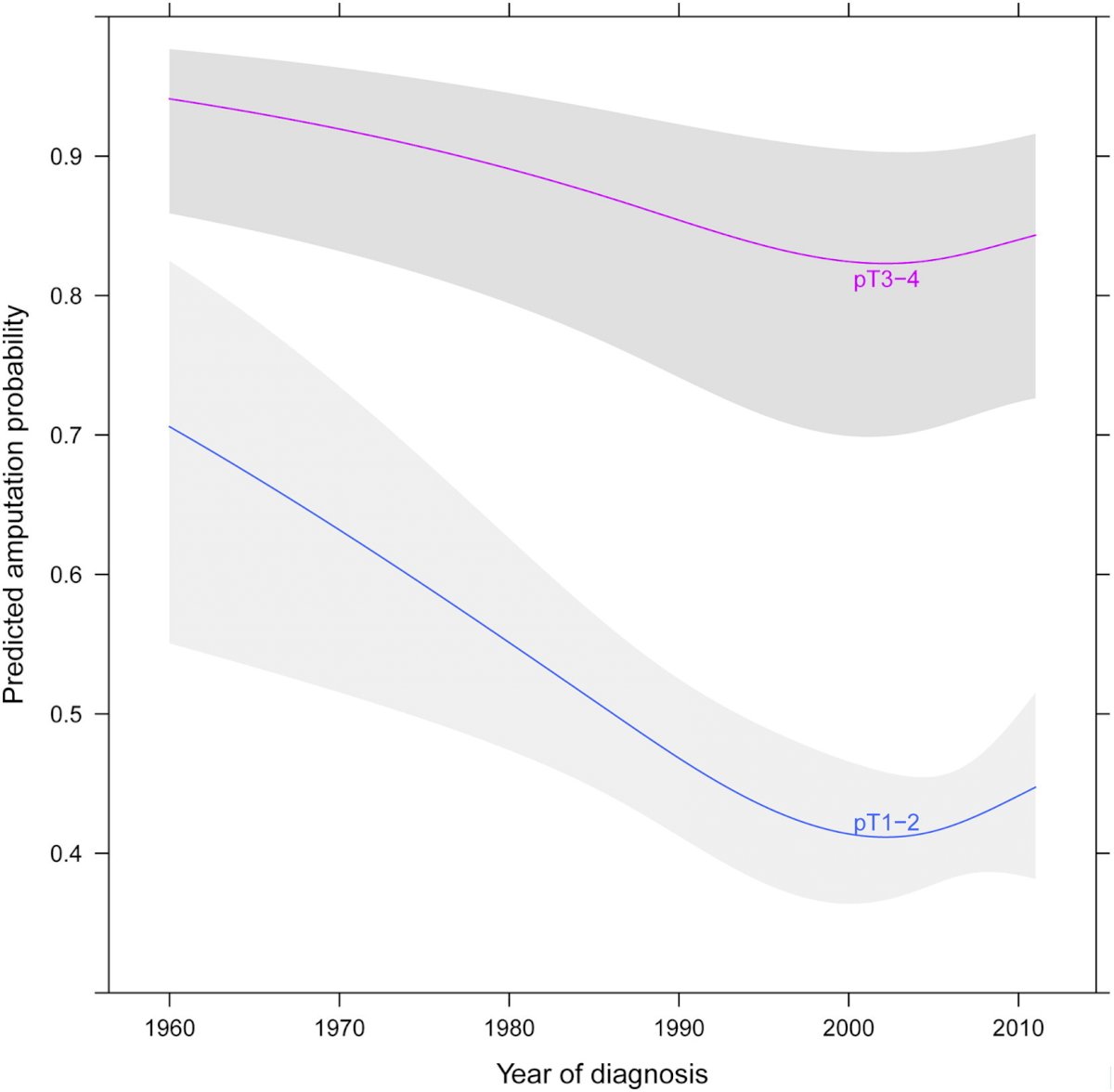
They found that the 5-year cumulative incidence of local recurrence as the first event after penile preservation was 27% (95% CI 23-32) while after partial penectomy it was 3.8% (95% CI 2.3-6.2, p <0.0001). Importantly, patients treated with penile preservation showed no significant difference in survival compared to patients treated with partial penectomy after adjusting for relevant covariates.
Dr. Masterson concluded his presentation by highlighting that the NCCN guidelines suggest long-term clinical exam follow-up for patients with penile preservation surgery, including every three months for years 1-2, every six months for years 3-5, and every 12 months for years 5-10.
Presented by: Timothy A. Masterson, MD, Indiana University, Indianapolis, IN
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the AUA2021 May Kick-off Weekend May 21-23.
References:
- Alnajjar HM, Lam W, Bolgeri M, et al. Treatment of carcinoma in situ of the glans penis with topical chemotherapy agents. Eur Urol. 2012 Nov;62(5):923-928.
- Tang DH, Yan S, Ottenhof SR, et al. Laser ablation as monotherapy for penile squamous cell carcinoma: A multi-center cohort analysis. Urol Oncol. 2018 Apr;36(4):147-152.
- Windahl T, Andersson SO. Combined laser treatment for penile carcinoma: Results after long-term follow-up. J Urol. 2013 Jun;169(6):2118-2121.
- Shindel AW, Mann MW, Lev RY, et al. Mohs micrographic surgery for penile cancer: Management and long-term follow-up. J Urol. 2007 Nov;178(5):1980-1985.
- Albersen M, Parnham A, Joniau S, et al. Predictive factors for local recurrence after glansectomy and neoglans reconstruction for penile squamous cell carcinoma. Urol Oncol. 2018 Apr;36(4):141-146.
- Sri D, Sujenthiran A, Lam W, et al. A study into the association between local recurrence rates and surgical resection margins in organ-sparing surgery for penile squamous cell cancer. BJU Int. 2018 Oct;122(4):576-582.
- Veeratterapillay R, Teo L, Asterling S, et al. Oncologic outcomes of penile cancer treatment at a UK supraregional center. Urology. 2015 May;85(5):1097-1103.
- Djajadiningrat RS, van Werkhoven E, Meinhardt W, et al. Penile sparing surgery for penile cancer –does it affect survival? J Urol 2014 Jul;192(1):120-125.