(UroToday.com) At the 2021 American Urological Association (AUA) Summer School session on the updates in the management of penile cancer, Dr. Viraj Master from Emory University discussed the management of inguinal lymph nodes in patients with no palpable adenopathy and in patients with non-bulky lymph nodes (<3-4 cm). According to Dr. Master, it is very difficult to salvage bad decision-making or bad inguinal surgery for penile cancer. Given that our risk assessment tools are imperfect for predicting the involvement of inguinal lymph nodes, Dr. Master emphasizes that we should err on the side of doing a groin dissection.
By way of reference, Dr. Master notes that the clinical staging TNM 8th edition update from 2018 for clinical nodal disease are as follows:
- N0: no palpable or visibly enlarged lymph nodes
- N1: palpable, mobile, unilateral inguinal nodes
- N2: palpable, mobile >=2 unilateral or bilateral inguinal nodes
- N3: palpable, fixed inguinal nodal mass or unilateral pelvic adenopathy or bilateral pelvic adenopathy
Over the last decade, penile cancer guidelines have upped their emphasis on the importance of lymph nodes. The European Association of Urology guidelines notes that ‘Management of the regional lymph node is decisive for long term survival. Cure can be achieved in metastatic disease confined to the regional lymph nodes.’ The 2021 updated NCCN guidelines note ‘the presence and extent of regional inguinal lymph node metastases have been identified as the single most important prognostic indicator in determining long-term survival in men with invasive penile squamous cell carcinoma.’
Dr. Master notes that according to the NCCN guidelines, palpable inguinal lymph nodes that are unilateral and <4 cm (mobile), in the setting of high-risk primary lesions, inguinal lymph node dissection is at the crux of management, either upfront or after neoadjuvant chemotherapy. In the setting of clinically visible lymphadenopathy, there is nowhere in any guideline that a trial of antibiotics should be considered. Additionally, for patients with non-palpable inguinal lymph nodes, those with an intermediate/high-risk tumor (T1b, or any T2 or greater) should undergo an inguinal lymph node dissection or a dynamic sentinel node biopsy. Dr. Master emphasized that it is important to define ‘high-risk’ penile tumors, which are those that are >=pT1b or >=pT2, those with vascular invasion/perineural invasion, or those that are poorly differentiated. However, interobserver accuracy of grading penile cancer specimens is not good, with interobserver agreement as low as kappa = 0.34 (low agreement).
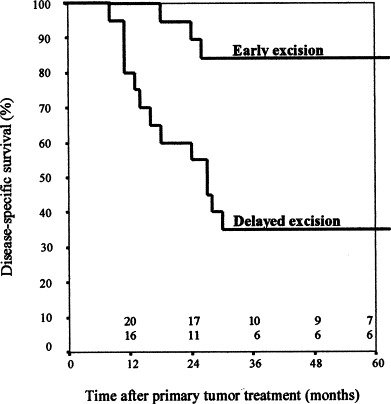
Additional reasons to err on the side of groin dissection is that there is micro-metastatic disease in 25% of impalpable groins and that in small case series of T1G2 tumors with nonpalpable lymph nodes, up to 44% of patients have microscopic metastatic disease. Dr. Master also highlighted that delayed lymphadenectomy for inguinal nodes is not a feasible approach. Kroon and colleagues previously compared the clinical outcome of early (n=20) vs delayed excision (n=20) of lymph node metastases in patients with penile squamous cell carcinoma.1 Despite similar age, T-stage, pathological tumor grade, and vascular invasion, they found that disease-specific 3-year survival of patients with positive lymph nodes detected during surveillance was 35%, and in those who underwent early resection was 84% (log-rank p = 0.0017):
Dr. Master then discussed dynamic sentinel node biopsy, which is rarely used in North America and primarily utilized in Europe. If used in the United States, dynamic sentinel node biopsy should be limited to centers with experience (at least 20 procedures/year), given the technical challenges of the procedure. However, dynamic sentinel node biopsy should not be done for patients with palpable lymph nodes, as these patients should proceed straight to a groin dissection.
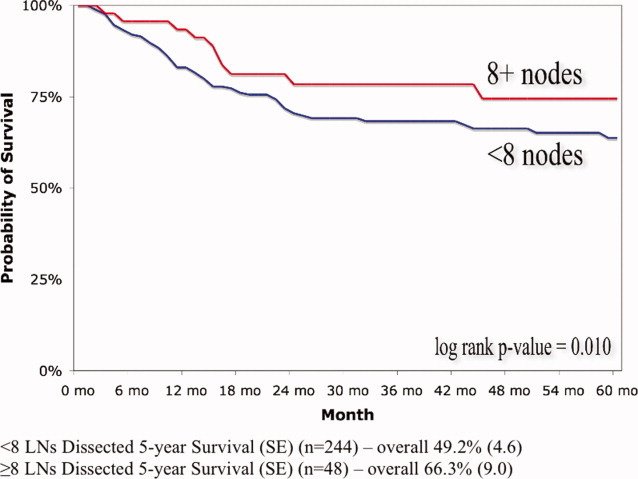
A decade ago, work from Dr. Master’s group assessed the frequency of inguinal lymphadenectomy and the impact of dissection extent on survival using the Surveillance, Epidemiology, and End Results (SEER) database (1988-2005).2 Specifically, they assessed the 5-year survival across patient- and disease-related characteristics for patients receiving inguinal lymphadenectomy involving <8 or >= 8 lymph nodes, the latter a surrogate for extent of dissection based on other malignancies. Among 593 patients, only 26.5% received an inguinal lymphadenectomy. Additionally, improved overall 5-year survival (HR 0.54, 95% CI 0.36-0.79) was observed in patients of all ages who received lymphadenectomy involving >= 8 lymph nodes:
With regards to the surgical approach to inguinal lymph node dissection, Dr. Master notes that he endorses both open and videoscopic groin dissections, noting that it is the surgeon’s experience that is most critical in performing an oncologically sound operation. From his experience, a videoscopic approach is technically easier for patients that are super obese (BMI >50). With adequate surgical experience, lymph node yield should be the same regardless of surgical approach.
Prophylactic radiotherapy in patients with cN0 groins is not recommended secondary to (i) failure to prevent the development of metastatic lymph nodes, (ii) complications of radiotherapy, and (iii) more difficult to follow a patient secondary to fibrotic changes. Adjuvant radiotherapy may improve locoregional control in patients with extensive metastases and/or extranodal spread, however, control is achieved at the cost of severe side effects including debilitating lymphedema and/or pain.
To conclude his presentation, Dr. Master highlighted via a case presentation that it is hard to salvage poor clinical decision-making. This patient is a 46-year-old male with multiple medical problems, including a kidney transplant secondary to Prune Belly syndrome who presented with the following lesion and was subsequently referred to Dermatology for a Mohs procedure:

Pathology from the Mohs procedure demonstrated squamous cell carcinoma, moderately differentiated, diffusely invading the dermis and subcutaneous tissue with perineural invasion present. Dr. Master noted that there was no cross-sectional imaging pre-procedure, and no mention of a groin examination. Six months later, the patient had palpable groin lymphadenopathy:
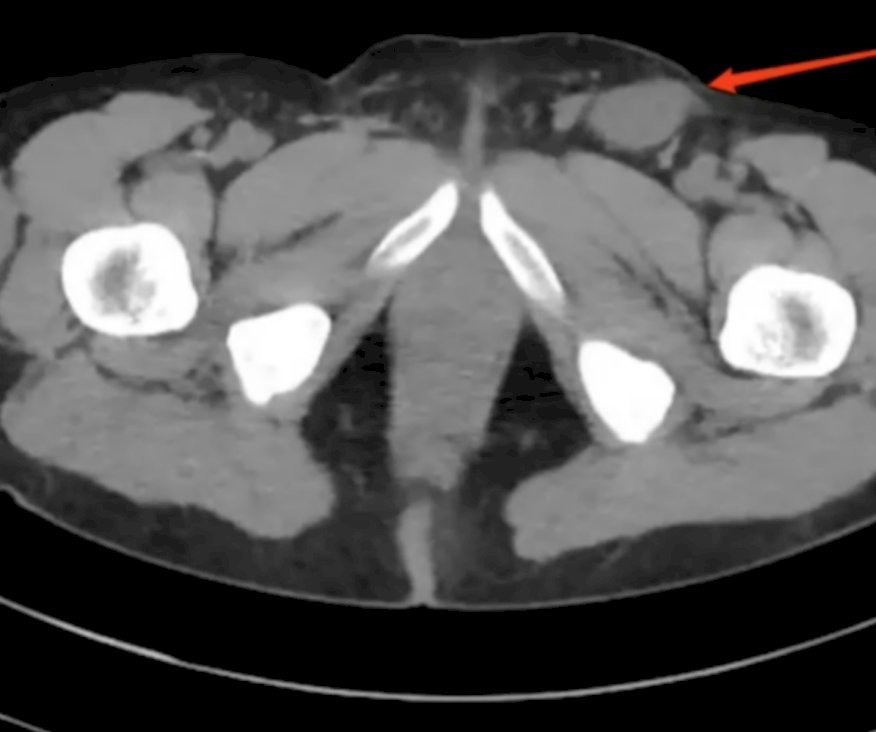
The patient was subsequently referred to Dr. Master who performed an open groin dissection that revealed a 4.2 cm metastatic lymph that was positive for extranodal extension of disease. To summarize, if it is difficult to obtain high-fidelity pathologic information (grade), and imaging has poor sensitivity, and if outcomes are poor when we wait for positive nodes to appear, then…err on the side of performing an inguinal lymph node dissection!
Presented by: Viraj Master, MD, PhD, Emory University, Atlanta, GA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the AUA2021 May Kick-off Weekend May 21-23.
References:
- Kroon BK, Horenblas S, Lont AP, et al. Patients with penile carcinoma benefit from immediate resection of clinically occult lymph node metastases. J Urol. 2005 Mar;173(3):816-819.
- Johnson TV, Hsiao W, Delman KA, et al. Extensive inguinal lymphadenectomy improves overall 5-year survival in penile cancer patients: Results from the Surveillance, Epidemiology, and End Results program. Cancer 2010 Jun 15;116(12):2960-2966.