(UroToday.com) At the 2021 American Urological Association (AUA) Summer School session on the updates in the management of penile cancer, Dr. Andrea Necchi from IRCCS San Raffaele Hospital and Scientific Institute in Milan discussed the perioperative treatment of penile cancer. Dr. Necchi notes that the prognosis of penile cancer is predictable based on the importance of N and M stage, with the most clinically important stage, with regards to management decision-making, being the N stage as highlighted in the following figure:

Dr. Necchi notes that population-level studies have highlighted the importance of doing an inguinal lymphadenectomy. Data from Joshi and colleagues looking at 1,123 patients with lymph node-positive disease in the National Cancer Database from 2004-2014 showed that the use of systemic chemotherapy has significantly increased from 38.2% to 47.8%.1 However, in this study, on multivariable analysis, inguinal lymph node dissection was associated with better overall survival (HR 0.64, 95% CI 0.52-0.78) while neither chemotherapy nor radiotherapy was associated with an improvement in overall survival:

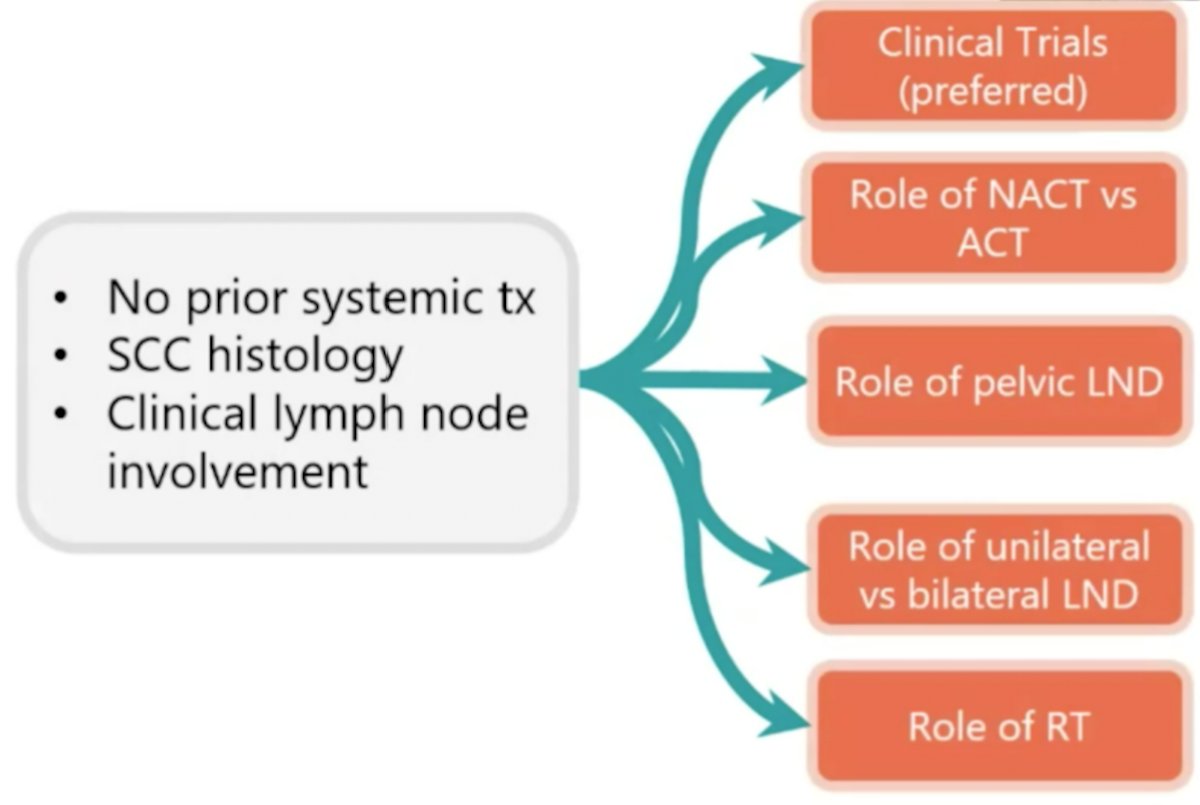
Dr. Necchi emphasized that the decision making in locally-advanced penile squamous cell carcinoma for patients with no prior systemic therapy and clinical lymph node involvement is challenging and not clear-cut:
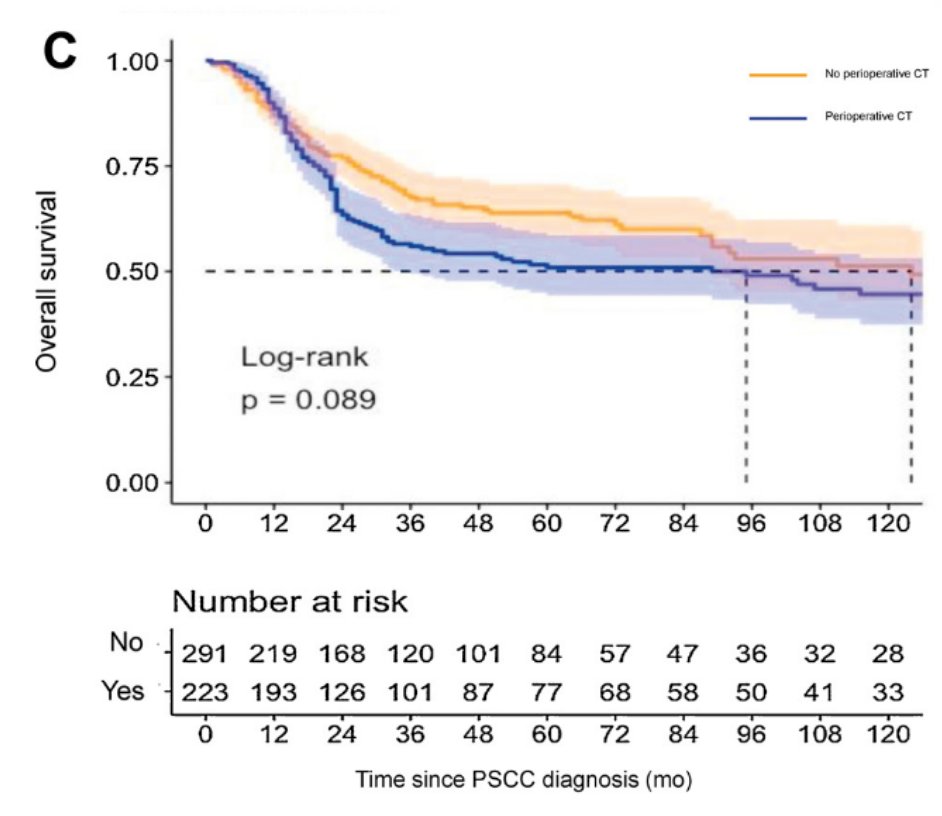
Work from Dr. Necchi’s group has recently assessed outcomes of perioperative chemotherapy in locally advanced penile squamous cell carcinoma.2 Using an international, multicenter database of 630 patients who received an inguinal lymph node dissection from 1980 to 2019 in the United States, Europe, Brazil, and China, there was no significant difference in overall survival based on use of perioperative chemotherapy:
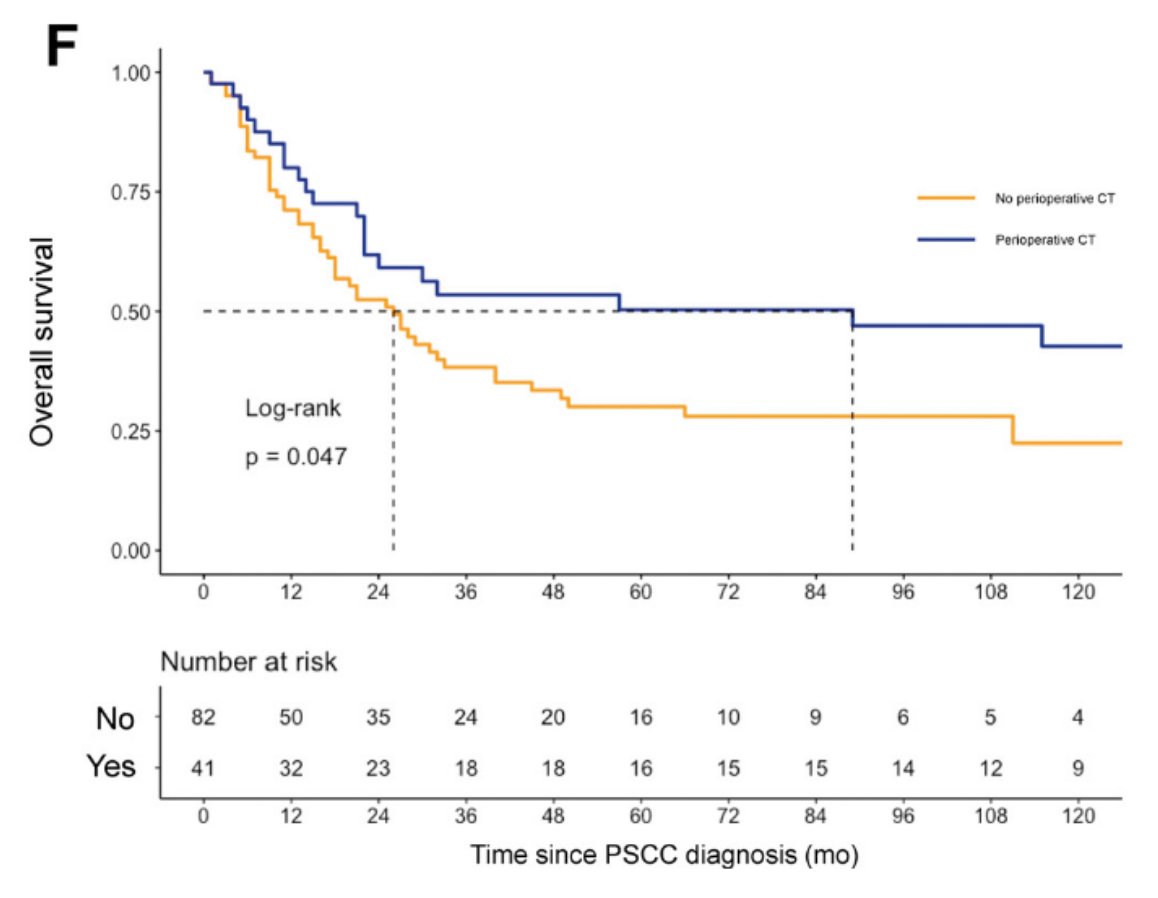
However, perioperative chemotherapy significantly improved overall survival for patients with pN2-N3 disease who did not receive a pelvic lymph node dissection:
With regards to the EAU guidelines for penile cancer, Dr. Necchi notes that for fixed inguinal lymph nodes (cN3), patients should receive neoadjuvant chemotherapy followed by radical inguinal lymphadenectomy in responders (weak recommendation), and adjuvant chemotherapy should be used in pN2/pN3 patients after radical lymphadenectomy (strong recommendation).
Looking at neoadjuvant TIP efficacy in a retrospective cohort, Dickstein and colleagues identified 61 patients, of which 54 (90%) received chemotherapy with paclitaxel/ifosfamide/cisplatin.3 Overall, 39 patients (65%) had either a partial or complete response to chemotherapy. Following neoadjuvant chemotherapy, 10 patients (16.4%) were pN0 with combined therapy and 20 patients (33%) were alive and disease-free at a median follow-up of 67 months. A recent meta-analysis of all neoadjuvant studies from Dr. Spiess’ group, included 10 studies (182 patients).4 Overall, 66 (36.3%) and 116 (63.7%) men were treated with non-taxane-platinum and taxane-platinum regimens, respectively. The pooled results demonstrated an objective response rate of 53% (95% CI 42-64), pathological complete response rate of 16%, grade 3 or greater toxicity rate of 40% (95% CI 19-64), and overall mortality of 55% (95% CI 40-70) among those treated with neoadjuvant chemotherapy.
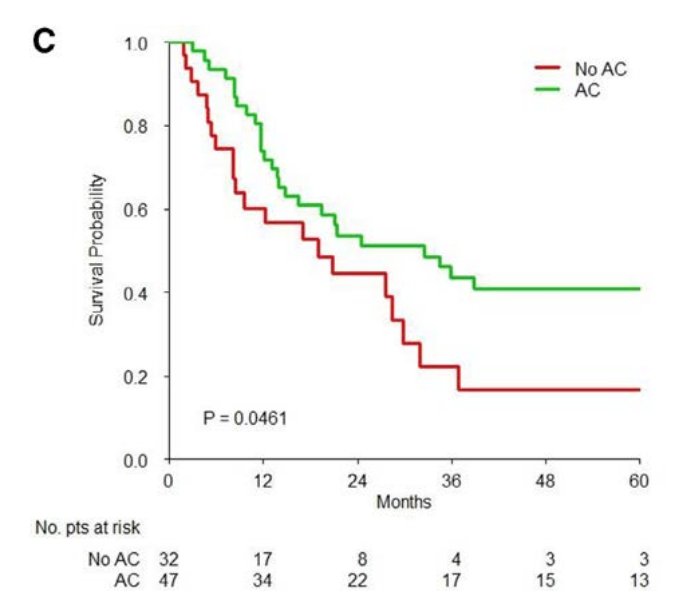
To assess the role of perioperative chemotherapy in N3 state disease, Dr. Necchi discussed a study from his group that included 689 patients who received lymph node dissection at seven referral centers. There were 86 (12.5%) patients that received neoadjuvant chemotherapy, 171 (24.8%) patients that received adjuvant chemotherapy, and 74 (10.7%) patients that received adjuvant radiotherapy. Neoadjuvant chemotherapy and adjuvant chemotherapy were ineffective in clinical and pathologic N1-2 patients, whereas adjuvant chemotherapy provided overall survival improvements in N3 patients:
Dr. Necchi summarized the real-world data from retrospective studies with the following recommendations:
- cN3 (pelvic lymph node positive): recommendation – neoadjuvant chemotherapy may be considered
- pN3 (pelvic lymph node positive): recommendation – adjuvant chemotherapy may be considered
- pN3 (extranodal extension): recommendation – adjuvant radiotherapy may be considered
- cN0,1,2: recommendation – neoadjuvant chemotherapy is not recommended; clinical trials are warranted
- pN0,1,2: recommendation – adjuvant chemotherapy is not recommended; clinical trials are warranted
Dr. Necchi also highlighted the InPACT trial, an important global clinical trial in penile cancer. Inclusion criteria for the trial include (i) men >= 18 years of age, (ii) biopsy proven squamous cell carcinoma of the penis, (iii) clinical T any, N1-N3, (iv) measurable disease by RECIST criteria (>= 1.5 cm short axis diameter), (v) ECOG performance status 0-2, (vi) patients able/willing to be randomized given preoperative parameters, (vii) laboratory evaluation consistent with potential randomization to various treatment arms (ie. adequate hematologic, renal, and liver function), (viii) willing and able to comply with the follow-up schedule, and (ix) written informed consent. Key exclusion criteria included (i) pure verrucous carcinoma, (ii) squamous cell carcinoma of the urethra, (iii) non-squamous penile malignancy, (iv) stage M1 penile carcinoma, (v) prior chemotherapy or chemoradiotherapy outside of the InPACT trial, (vi) concurrent malignancy (other than SCC skin or basal cell carcinoma) that required any treatment in the last 3 years (low risk prostate cancer on active surveillance was allowed), (vii) sexually active patients who are unwilling to use effective contraception. The InPACT trial design is as follows:
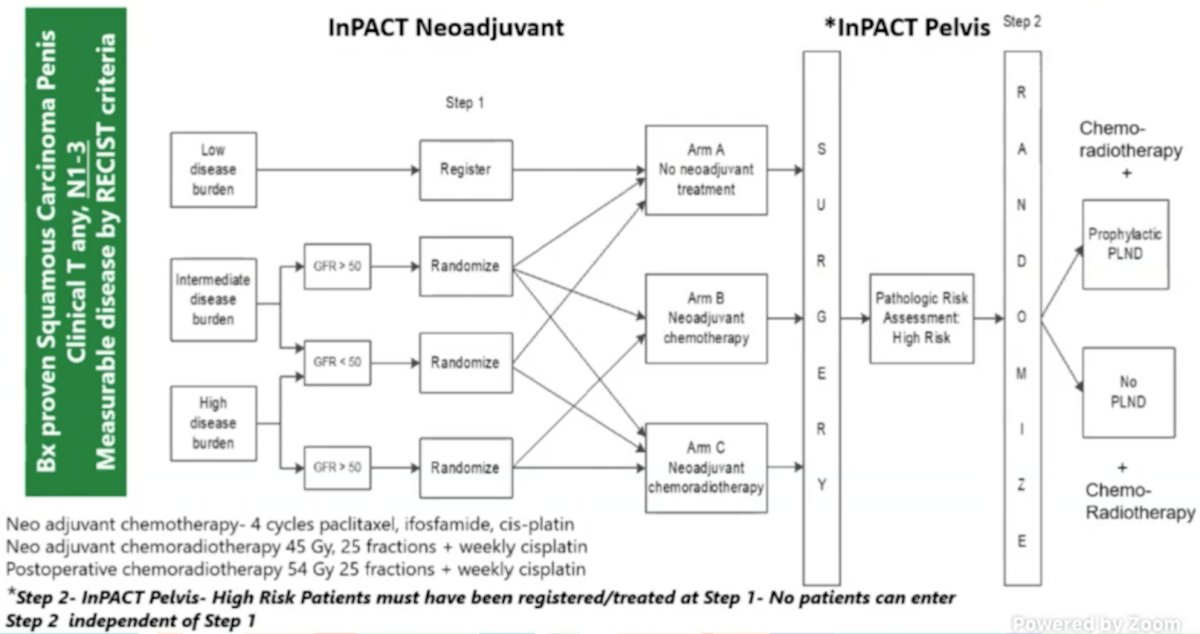
The primary endpoint for the InPACT trial is survival, with secondary endpoints including DSS, DFS, DMFS, LRFS, pN0 rate, toxicity, surgical complications, and feasibility of delivering treatment on schedule. The target accrual for InPACT is 400 patients across all international sites, including 200 in North and South America.
Dr. Necchi concluded his presentation with the following take-home messages:
- For neoadjuvant chemotherapy, the EAU guidelines and retrospective studies advise that neoadjuvant chemotherapy should be used for unresectable or recurrent lymph node metastases (the main effect being observed in clinical/pathological N3 stage)
- For adjuvant chemotherapy, the EAU guidelines and retrospective studies recommend adjuvant chemotherapy if there are nodal metastases (>pN1), with the main effect observed in pN3 patients
- For clinical trials, the InPACT trial needs to be supported to definitively evaluate the role of neoadjuvant chemotherapy versus chemoradiotherapy, and pelvic lymph node dissection in those undergoing adjuvant chemoradiation
Presented by: Andrea Necchi, MD, IRCCS San Raffaele Hospital and Scientific Institute, Milan, Italy
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the AUA2021 May Kick-off Weekend May 21-23.
References:
- Joshi SS, Handorf E, Strauss D, et al. Treatment trends and outcomes for patients with lymph node-positive cancer of the penis. JAMA Oncol. 2018;4(5):643-649.
- Bandini M, Zhu Y, Ye DW, et al. Contemporary treatment patterns and outcomes for patients with penile squamous cell carcinoma: Identifying management gaps to promote multi-institutional collaboration. Eur Urol Oncol. 2021 Feb;4(1):121-123.
- Dickstein RJ, Munsell MF, Pagliaro LC, et al. Prognostic factors influencing survival from regionally advanced squamous cell carcinoma of the penis after preoperative chemotherapy. BJU Int 2016;117(1):118-125.
- Azizi M, Aydin AM, Hajiran A, et al. Systemic review and meta-analysis—Is there a benefit in using neoadjuvant systemic chemotherapy for locally advanced penile squamous cell carcinoma? J Urol. 2020;203(6):1147-1155.
- Necchi A, Lo Vullo S, Mariani L, et al. Nomogram-based prediction of overall survival after regional lymph node dissection and the role of perioperative chemotherapy in penile squamous cell carcinoma: A retrospective multicenter study. Urol Oncol. 2019 Aug;37(8):531.e7-531.