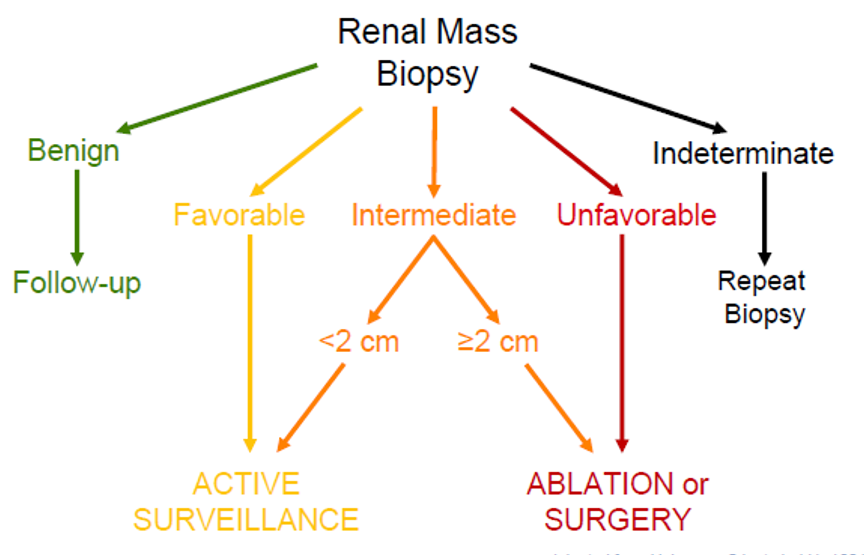
Dr. Gorin provided the first presentation in this session, focusing on the use of molecular imaging for risk stratification of localized renal tumors. He began by emphasizing that small renal masses may either be renal cell carcinoma (RCC) (including clear cell, 55%; papillary 20%; or chromophobe, 5%) as well as benign histologies including angiomyolipoma (5%) and oncocytoma (10%). These differences in histology are important as the prognosis differs substantially, not just between the benign and malignant entities but also among the subset of renal cell carcinoma. Thus, treatment decisions may differ on the basis of underlying tumor histology. A renal mass biopsy is one approach to histologically characterize small renal masses. As highlighted in the flow diagram below, renal mass biopsy results may meaningfully affect management choice.
However, there are meaningful limitations to renal mass biopsy. These include the associated pain and discomfort, a non-diagnostic rate of 10-20%, a major complication rate of 1%, an inability to perform a biopsy for many patients due to anatomic location, an inability to accurately determine tumor grade based on sampling, the innate molecular heterogeneity of renal masses, and the conundrum of the oncocytic neoplasm in which the pathologist is unable to distinguish between oncocytoma and chromophobe RCC. Thus, the question is can molecular imaging approaches differentiate among the various renal tumor histologies.
Dr. Gorin transitioned to discussing the basis of nuclear/molecular imaging, highlighting that this is a branch of radiology that leverages radiopharmaceuticals to diagnose and treat disease. Unlike anatomic imaging which we are more familiar with (including x-ray, CT, MRI, and ultrasonography) that measures structure information, molecular imaging allows for an assessment of the functional, metabolic, or molecular characteristics of cellular processes. This may be performed with either single-photon emission computed tomography (SPECT) or positron emission tomography in combination with low-dose computed tomography (CT).

SPECT has substantially lower spatial resolution compared with PET and cannot be directly quantifiable. However, it is low cost and allows for the potential concurrent use of multiple tracers.
In the context of molecular imaging for renal tumors, there are many tracers available. Imaging widely metastatic disease may be accomplished using FDG-PET/CT based on metabolic activity. However, in the context of localized disease, Dr. Gorin focused on girentuximab which binds to carbonic anhydrase IX (CAIX), an enzyme that is implicated in clear cell renal cell carcinoma through the VHF-HIF pathway. CAIX may act as a biomarker for ccRCC based on its presence on the cell surface. This is not seen in other subtypes of RCC, including papillary disease.

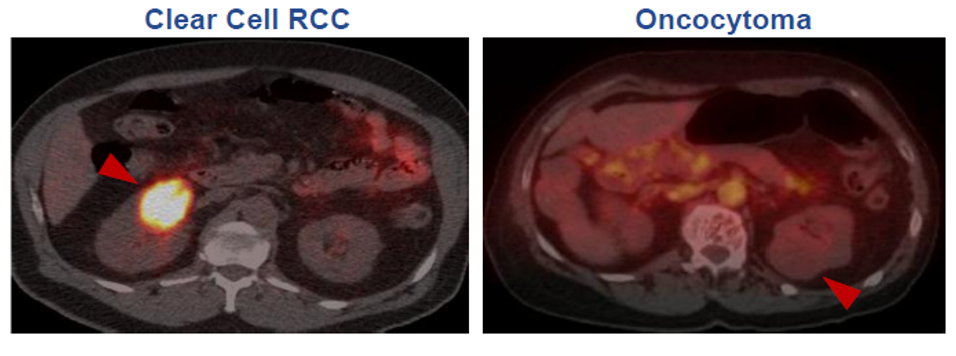
124I-girentuximab immune-PET/CT can be used for imaging renal masses. As highlighted in the figure below, clear cell renal cell carcinoma avidly enhances with the use of this tracer whereas oncocytomas do not. He suggested that this may be used as an “imaging-based biomarker”.
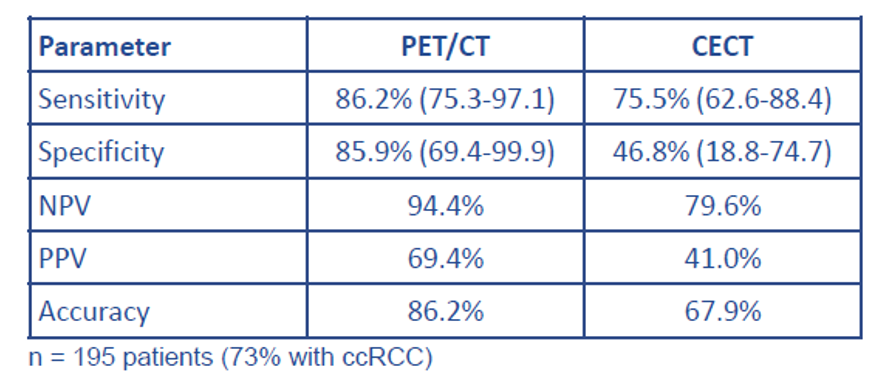
The REDECT trial assessed the role of 124I-girentuximab immune-PET/CT for the identification of clear cell renal cell carcinoma. Compared to contrast-enhanced CT, PET/CT had improved sensitivity, specificity, negative predictive value, positive predictive value, and accuracy on the basis of the blinded review. Surgical pathology was used as the gold standard for the comparison of these imaging approaches. He noted in particular, that PET/CT had substantially better specificity compared with contrast-enhanced CT.
This agent did not proceed into the second trial necessary for FDA approval, until recently with the ongoing phase III ZIRCON trial expected to complete accrual in the fall of 2021. This may lead to approval in the relatively near future.
Dr. Gorin then discussed the role of 99mTc-sestamibi, a mitochondrial imaging agent, which can be used (with SPECT/CT) to distinguish clear cell renal cell carcinoma from oncocytoma. Sestamibi is currently used for imaging of parathyroid adenomas as well as cardiac imaging. Clear cell RCC is relatively devoid of mitochondria, thus, they postulated that ccRCC would not take up this radiotracer.
In a work where Dr. Gorin was the first author, oncocytoma/HOCT was positive on 99mTc-sestamibi SPECT/CT in 87.5% of patients (83.3% of those with oncocytoma and 100% with HOCT) whereas only 4.8% of patients with renal cell carcinoma or AML. These findings were subsequently independently validated, showing a sensitivity of 93% and specificity of 87.5% for oncocytoma and hybrid oncocytoma-chromophobe tumors. A subsequent pooled analysis suggested similar findings, with a sensitivity of 83% (95% CI 66-92%) and specificity of 96% (95% CI 84-99%). Both positive and negative predictive values differed on the basis of

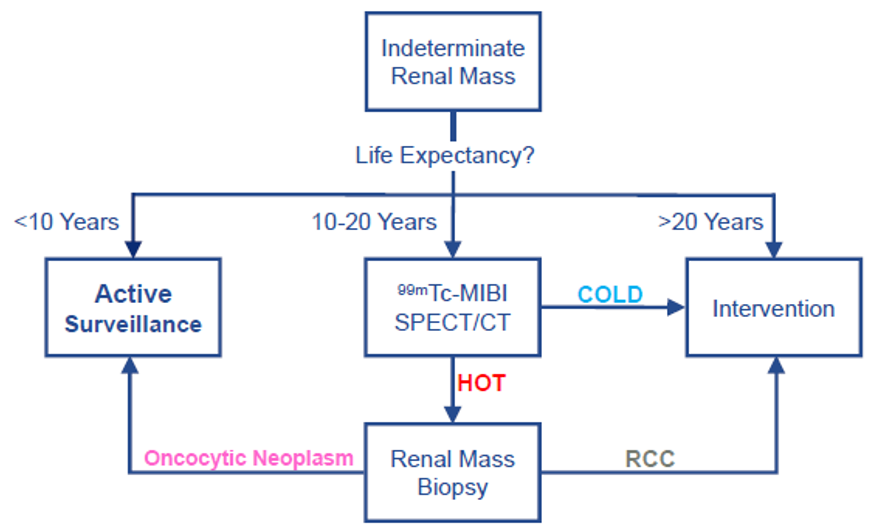
On the basis of these data, Dr. Gorin then postulated an evolving approach to small renal masses guided by a combination of life expectancy, imaging findings based on 99mTc-MIBI SPECT/CT, and renal mass biopsy to guide management.
He, therefore, concluded that molecular imaging offers a promising non-invasive means to determine renal mass histology and guide risk stratification.
Presenter: Michael A Gorin, M.D., Urologist, Urology Associates, Cumberland, Maryland.
Written by: Christopher J.D. Wallis, Urologic Oncology Fellow, Vanderbilt University Medical Center, @WallisCJD on Twitter, during the AUA2021 May Kick-off Weekend May 21-23.