(UroToday.com) In anticipation of the 2021 American Urological Association (AUA) Annual Meeting which is being held, in a delayed fashion, in September, the AUA hosted a “May Kick-Off Weekend” which highlighted a variety of important topics in both benign urology and urologic oncology. Sunday morning, Costas Lallas led a course entitled “Chemotherapy and Immunotherapy for the Urologist and Advanced Practice Provider” along with faculty Edouard Trabulsi and Anne Calvaresi.
Presenting on prostate cancer, Anne Calvaresi began by highlighting the well-known and oft-cited continuum of prostate cancer.
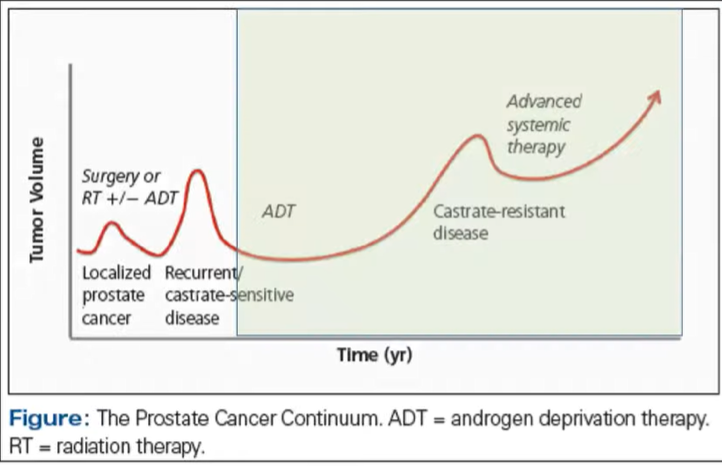
In this context, she then provided an overview of systemic therapy approaches, beginning with traditional hormonal ablation with androgen deprivation therapy. She first discussed gonadotropin-releasing hormone (GnRH) agonists including leuprolide, goserelin, and histrelin. These agents act by stimulating LH and FSH from the pituitary gland. Through chronic stimulation, there is negative feedback which leads to testosterone suppression. In contrast, GnRH antagonists such as degarelix directly inhibit pituitary LH and FHS release. She further discussed non-steroidal anti-androgens, which function by blocking the binding of androgens to the androgen receptor. As a result, while androgenic function decreases, testosterone levels often rise and may contribute to gynecomastia. Other approaches for androgen suppression including surgical castration with bilateral orchiectomy and ketoconazole, though these approaches are predominately historical despite their ability to induce rapid castration

She then discussed the side effects of hormonal therapy, as well as mitigation strategies.
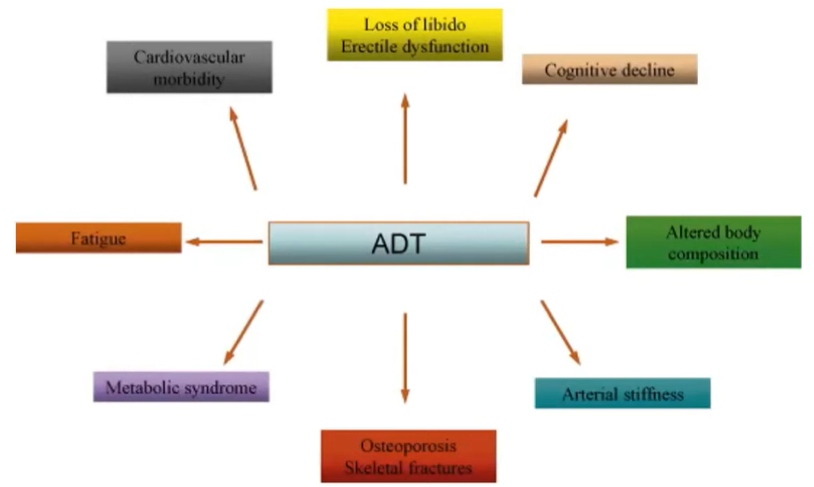
ADT-associated cognitive decline may specifically affect verbal memory, visuomotor function, attention and executive function. She suggested that to counter these effects, we should encourage patients to engage in physical activity, use mindfulness-based stress relief, and employ mental stimulation and brain training. In terms of the metabolic dysfunction and fatigue associated with ADT, she emphasized the importance of involving the patient’s primary care physician as well as encouraging daily exercise, a well-balanced diet, and a regular sleep routine. More specifically addressing the cardiovascular morbidity of ADT, she recommended smoking cessation where relevant, aerobic exercise, a heart healthy diet, and involvement of cardiologists where appropriate.
In terms of the neuro-psychiatric effects, she suggested that optimized management of physiologic side-effects of ADT may help protect mood. On a patient-by-patient basis, anti-depressants, counseling, and support groups may be helpful. In terms of side effects, hot flashes are difficult to manage in Anne Calvaresi’s experience. Many of the suggested treatments have their own side effects; however, she suggested megestrol acetate and SSRIs, as well as considering non-pharmacologic interventions such as acupuncture and vitamin B supplementation.
In terms of bone health, all patients should be receiving vitamin D and calcium supplementation. In addition, she advocated for routine use of DEXA, which she felt is underutilized. For patients with osteoporosis or those at particularly high risk, anti-resorptive agents such as denosumab or zoledronic acid are beneficial.
Following this, she transitioned to discussing treatment options in metastatic castration sensitive prostate cancer, highlighting the trials supporting each intensified approach. As she emphasized, each of these treatments in premised on a backbone of ongoing ADT. While not discussed, the first intensified approach utilized docetaxel, on the basis of data from CHAARTED and STAMPEDE. However, Anne Calvaresi began by highlighting the ARCHES trial and the ENZAMET trial, each of which demonstrated the superiority of adding enzalutamide to ADT in this disease space. Notably, ARCHES allowed prior use of docetaxel while ENZAMET allowed docetaxel therapy after index. Further ENZAMET used an active comparator with NSAA including bicalutamide, nilutamide, or flutamide.
She then transitioned to discussing the TITAN trial which, in a similar patient population, demonstrated that the addition of apalutamide improved overall survival and progression-free survival.
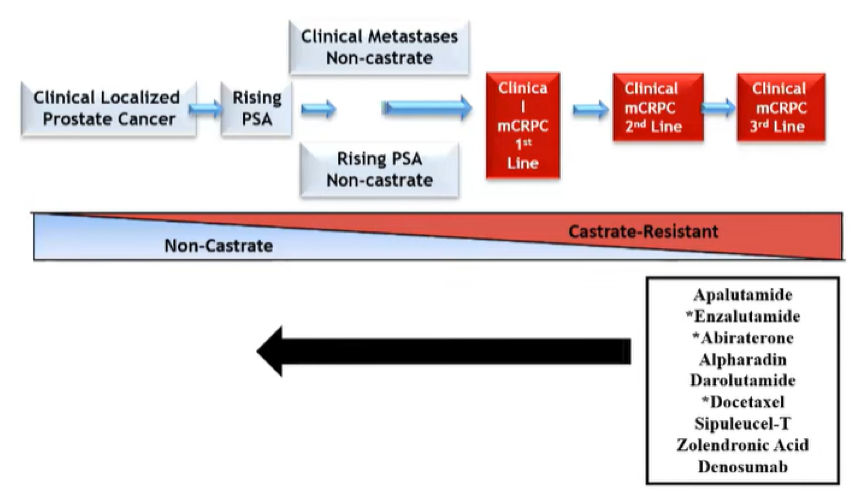
As these trials have shown, treatment approaches that were originally assessed and proved beneficial in advanced disease have moved forward in the treatment continuum.
Moving from the mCSPC disease space, she then discussed advances in the treatment of patients with non-metastatic castration-resistant disease. Based on relatively recently published data, the NCCN guidelines offer the option of ongoing ADT with either close observation or treatment with apalutamide, enzalutamide, or darolutamide. She noted that apalutamide is associated with the risk of hypothyroidism, skin rash, and fracture.
She then moved to discuss treatment approaches for mCRPC. She emphasized that guidelines recommend ongoing castration, consideration of bone anti-resorptive agents, and the potential role for sipuleucel-T in patients with bone-only asymptomatic or minimally symptomatic disease. While phase III data have demonstrated a survival benefit for the use of sipuleucel-T, it is not routinely used as it does not necessarily have a monitorable effect (on either PSA or radiographic disease). However, observational data suggested that the benefit of sipuleucel-T is maximized when it is used early.

As most UroToday readers will know, Anne Calvaresi highlighted the multitude of approvals in the mCRPC disease space since 2004, and in particular since 2010: docetaxel was approved on the basis of the TAX-327 trial in 2004. Subsequently, the androgen-axis targeting agents abiraterone acetate and enzalutamide were approved, first in the post-chemotherapy and then in the pre-chemotherapy setting.

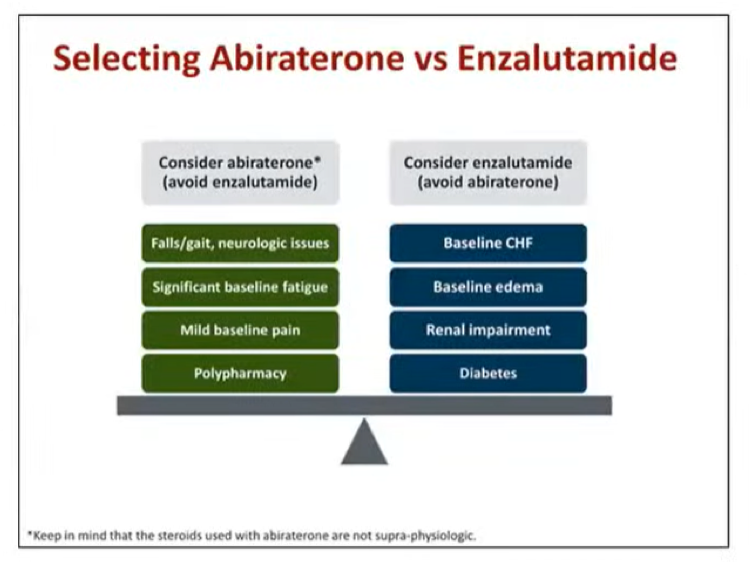
Discussing each agent, abiraterone acetate functions as an androgen biosynthesis inhibitor, targeting the cytochrome p450 enzyme 17-alpha-hydroxylase. She highlighted the potential for a number of drug interactions including rifampin, antifungals, HIV antiretrovirals, and anti-epileptics. She highlighted that, after being prescribed abiraterone, patients need to be followed closely, including liver function testing, electrolyte monitoring, and assessment of cardiovascular health. She suggested that this ongoing monitoring for toxicity and response may be a valuable area in which advanced practice providers (APPs) can contribute to the care of these patients.

She then transitioned to discussing enzalutamide, a high-affinity androgen receptor inhibitor that also functions to prevent the translocation of the androgen receptor to the nucleus and prevents the transcription of tumor-related genes. As with abiraterone acetate, there are many drug-drug interactions, including gemfibrozil, rifampin, phenytoin, carbamazepine, warfarin, and immunosuppressives.
She then transitioned to discussing the role of chemotherapy in advanced prostate cancer. While, for many years, chemotherapy had not proven survival benefit in prostate cancer, this changed with the publication of the TAX-327 trial of docetaxel. Subsequently, cabazitaxel showed benefit and was approved for patients who progressed following docetaxel.
Moving from chemotherapeutics, she then discussed radioisotopes. As bony growth develops around metastases, this bone turnover can be targeted by calcium mimetics. While many of these are used for palliation only, radium-223 has proven survival benefits in addition to symptomatic improvements in patients with mCRPC following chemotherapy or in those who are chemotherapy-ineligible.
Moving forward, she highlighted new directions including combinations of chemotherapy and androgen-axis targeting agents, abiraterone and anti-androgens, and others. However, some caution is warranted given the worse outcomes seen in the ERA-223 trial of radium-223 and abiraterone acetate. Other agents including PARP inhibitors, novel anti-androgens targeting splice variants, and theranostic treatment with radio-isotopes.
As immune checkpoint inhibition has proven beneficial in many solid organ malignancies, she then discussed why it has not gained traction in prostate cancer. This is driven, in part at least, by the lower mutational burden in prostate cancer which results in fewer neoantigens and fewer targets for immune response.

Briefly highlighting the Philadelphia consensus conference, she mentioned the growing importance of genetic and germline testing in advanced prostate cancer.
In closing, she highlighted that APPs may contribute to advanced prostate cancer care through routine screening of laboratory studies and imaging studies, management of toxicities, administration of treatment, and oncology follow-up.
Presented by: Anne E. Calvaresi, DNP, CRNP, Director of Clinical Operations and Urology Nurse Practitioner, Jefferson University Hospital
Written by: Christopher J.D. Wallis, Urologic Oncology Fellow, Vanderbilt University Medical Center, @WallisCJD on Twitter during the AUA2021 May Kick-off Weekend May 21-23