(UroToday.com) Monday morning’s plenary featured Dr. Boyd Viers of Mayo Clinic, who delivered a data-driven, clinically actionable lecture on reducing opioid prescribing in urological surgery. Framing his opening with characteristic directness, Dr. Viers established the core premise of his talk: “We are the prescribers. We are the solution.” He presented data from national registries, multi-institutional collaboratives, and his own institution’s five-year journey from prescribing all patients five opioid tablets to zero. In a call to action, he offered every urologist in the room a practical framework they could implement the following morning.
The Problem
Dr. Viers opened with four numbers that frame the urgency of opioid stewardship in urology. New persistent opioid use occurs in 6.2% of opioid-naïve urologic patients at 3-6 months, with 1% progressing to chronic use beyond one year. After radical cystectomy, that rate rises to 14.6%. After radical orchiectomy in young men, the rate reaches 10.5% compared to 0% in opioid-free cohorts, and patients receiving an artificial urinary sphincter (AUS) face three times higher odds of new persistent use at 3-9 months. Extrapolating across approximately 930,000 urologic operations performed annually in the US, Dr. Viers estimated that roughly 57,000 new persistent opioid users can be attributed to urology each year. “The prescription,” he emphasized, “is the causal lever, not the surgery.”
The broader surgical literature reinforces this urgency. New persistent opioid use occurs in 6% of opioid-naïve adults after any elective surgery, with no meaningful difference between minor and major procedures. Between 67-92% of surgical patients have unused opioids remaining at recovery. Persistent opioid users face a 3.44 times hazards ratio for mortality and a 68% increased risk of opioid-related emergency department visits and readmissions in the year after surgery. Critically, as Dr Viers emphasized, across every procedure studied, the evidence supports zero as the recommended minimum opioid prescription.

Figure 1. Background: The incidence of new persistent opioid use in minor surgery = 5.9% vs. major surgery = 6.5%; OR 1.12, SE 0.06, 95% CI 1.01–1.24. From Brummett et al, 2020.
In the field of urology, even minor procedures carry meaningful risk. Among patients who fill a minor urologic opioid prescription, the odds ratio for long-term opioid use at 9-15 months is 1.43 (NNH=148), and the odds ratio for opioid overdose requiring emergency or hospital care is 3.01 (NNH=2,000). Sixty percent of prescribed opioids go unused, and 67% of those are kept unsecured at home for a median of 11 months. “It doesn’t matter if it’s minor or major surgery,” Dr. Viers noted. “The risk is real, and it’s sustainable.”
Dr. Viers highlighted the populations carrying the greatest lifetime burden. Hypospadias repair in adolescents and young adults carries a relative risk of 17.0 for new persistent opioid use disorder. In the most vulnerable patient group in urology, stewardship of opioid use is important, Dr. Viers noted. AUS implantation carries a relative risk of 3.08 (15% vs. 5% persistent use), the 7th-highest prescription rate among 21 urologic procedures. Radical orchiectomy is nationally associated with opioid prescribing in 89.8% of cases, despite a 0% persistent use rate in opioid-free cohorts. And radical cystectomy, at 14.6%, represents the highest persistent-use rate of all urologic procedures. Across all procedures, greater initial opioid prescription size shows a near-linear association with increased risk of persistence.
AUA Guidelines
The AUA Clinical Consensus Statement, reaffirmed in 2022, outlines eight strategies for reducing post-operative opioid prescribing. Dr. Viers walked through the most clinically impactful: patient-centered contextualization through shared decision-making rather than default prescribing; preoperative education and expectation-setting, which he called the highest-yield single intervention and the primary mechanism by which he shifted patient buy-in to non-opioid pathways in his own reconstructive practice. These strategies included maximizing non-opioid therapies, including scheduled acetaminophen and NSAIDs, procedure-specific prescribing where the minimum is always zero, regional anesthesia when feasible, mandatory Prescription Drug Monitoring Program (PDMP) query at every prescription, electronic prescribing to leverage the workflow “nudge,” and safe disposal education both preoperatively and postoperatively to close the home reservoir. The AUA’s reaffirmed its position: “Lowest effective dose, shortest duration. Do not continue beyond the immediate postoperative period.”
The Multimodal Cocktail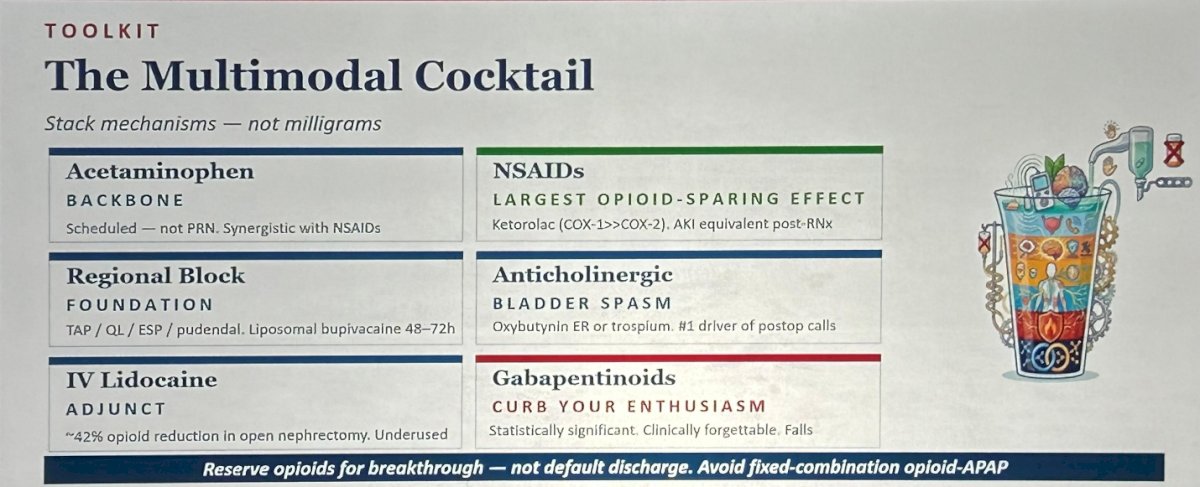
Figure 2: The Multimodal Cocktail: Non-opioid regimen for pain control.
Dr. Viers presented the multimodal analgesic cocktail as the operational backbone of opioid stewardship. Scheduled acetaminophen, not PRN, is the first pillar. NSAIDs provide the largest single opioid-sparing effect of any adjunct, he emphasized. Regional nerve blocks are the structural pillar, using blocks with liposomal bupivacaine for 48-72 hours of duration. Anticholinergics, such as oxybutynin ER or trospium, address bladder spasm, the number one driver of post-operative calls in reconstructive urology. Dr. Viers recommended IV lidocaine, a significantly underused adjunct associated with approximately 42% opioid reduction in open nephrectomy. Opioids, when prescribed at all, should be reserved for breakthrough, and fixed-combination opioid-acetaminophen preparations should be avoided.
Dr. Viers then devoted a dedicated slide to rehabilitating ketorolac’s reputation, subtitling it “Friend, Not Felon.” The longstanding fears, such as bleeding, acute kidney injury (AKI), anastomotic leak, and delayed bone healing, represent what he called “generations of dogma” rather than evidence. The data show that ketorolac provides the largest single opioid-sparing effect of any adjunct, with AKI rates equivalent to opioid-only regimens post-nephrectomy (27.6% vs. 27.9%), safety at ≤5 days in selected patients, and no increased bleeding in modern radical cystectomy, radical prostatectomy, or PCNL cohorts. Appropriate exclusions apply: CKD, active hypovolemia, and frail elderly patients. “Scheduled NSAID plus acetaminophen,” Dr. Viers stated, “is the foundation of every contemporary urologic pain pathway.”
Dr. Viers then delivered an equally direct assessment of gabapentinoids, summarizing the evidence in one phrase: “Statistically significant. Clinically forgettable.” Meta-analysis shows pooled pain-score reduction below the minimally important difference, with no benefit beyond 72 hours. In addition, adverse effects, from dizziness to falls to sedation that undermines early ambulation goals to respiratory depression carrying a 2019 FDA black-box warning, strongly argue against the routine use of gabapentinoids. His bottom line: individualize and reserve gabapentinoids strictly for neuropathic or chronic pain phenotypes. “Don’t sprinkle it on every patient,” he said.
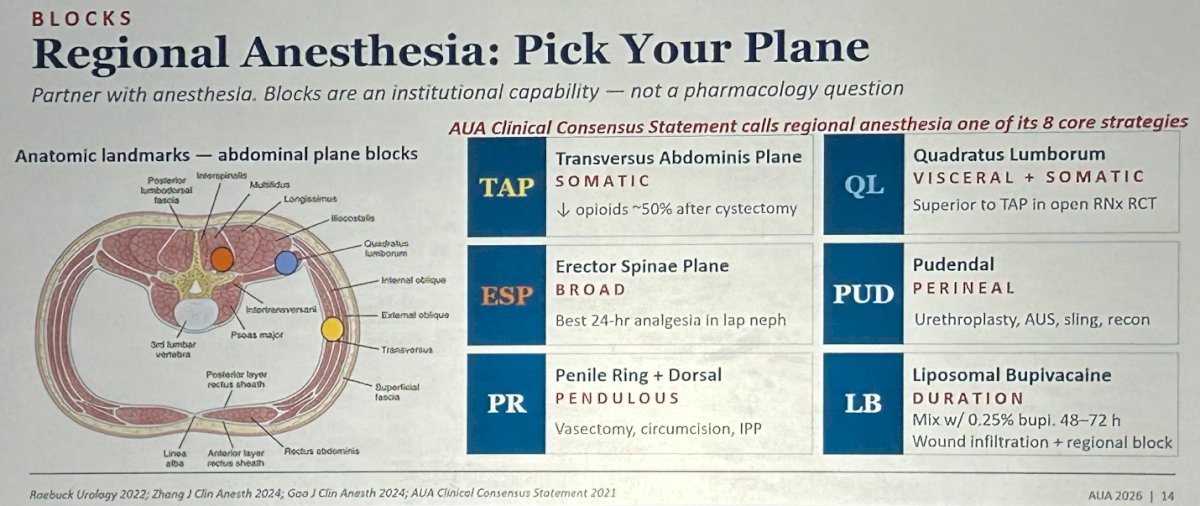
Figure 3: Regional Anesthesia Blocks: pick your plane.
Regional anesthesia, Dr. Viers emphasized, is essential in non-opioid pain management, and requires a deliberate partnership with anesthesia colleagues. The AUA Consensus Statement lists it as one of eight core strategies. The choice of block should match the operative anatomy: TAP (transversus abdominis plane) for somatic abdominal coverage, reducing opioid requirements approximately 50% after cystectomy; quadratus lumborum (QL) for combined visceral and somatic coverage, superior to TAP in open nephrectomy RCTs; erector spinae plane (ESP) for broad coverage with the best 24-hour analgesia in laparoscopic nephrectomy; pudendal for perineal cases including urethroplasty, AUS, and sling; penile ring and dorsal block for vasectomy, circumcision, and inflatable penile prosthesis.
Procedure-Specific Playbooks
Drawing on data from MUSIC ROCKS (Michigan Urological Surgery Improvement Collaborative – Reducing Operative Complications from Kidney Stones), Dr. Viers described one of the most striking opioid reduction success stories in urology. Opioid prescriptions after ureteroscopy fell from 83% to 13% between 2016 and 2023, with opioid-free discharge not associated with any increase in emergency department visits, and $4.8 million was avoided in statewide prescription spending.
Achieving this was straightforward, as the plan integrates preoperative acetaminophen 1,000 mg with patient counseling focused on setting expectations around stent bother rather than pain, intraoperative IV ketorolac 15 mg for patients with eGFR ≥60 alongside intraurethral 2% lidocaine, and postoperative scheduled acetaminophen plus NSAID continued for 72 hours. Anticholinergics address urgency symptoms, with tamsulosin and phenazopyridine rounding out the regimen. Discharge opioid defaults are procedure-matched and intentionally minimal: zero for cystoscopy and TURP, zero to five tablets for ureteroscopy, and zero to fifteen for PCNL.
Dr. Viers paused for what he called a public service announcement: the belladonna and opium (B&O) suppository has returned. For decades, the B&O suppository was the standard for refractory bladder spasm after TURP, TURBT, stent placement, and ureteroscopy, with RCT evidence supporting improved quality of life and reduced urinary pain through postoperative day 3, and preemptive use reducing urinary urgency after URS. A 2021 corporate split between Padagis and Perrigo caused a nationwide shortage through 2024. The suppository remains Schedule II, unapproved by the FDA since 1938, and still effective. “We buried it too soon,” Dr. Viers said. “The multimodal pathway has a rectal option again.”
For ambulatory urologic procedures, Dr. Viers’ message was unequivocal. He stated that if a patient walks out the door the same day, they almost certainly do not need an opioid. Vasectomy is managed with ibuprofen and ice, and patients prefer it. Adult circumcision and hydrocelectomy use a penile or spermatic cord block plus scheduled NSAIDs and APAP. Urethral sling and AUS implantation now have published zero-opioid series: in Pence/Viers 2024, 0 of 6 sling patients and 0 of 7 AUS patients received opioid prescriptions. Urethroplasty reaches a median of zero opioids used in recent series. Inflatable penile prosthesis remains the one ambulatory procedure where 5-10 tablets is still a reasonable default, with emerging perineal block pathways being studied.
Dr. Viers then shared his own institution’s five-year trajectory as a case study in what sustained commitment to opioid stewardship can achieve. Beginning in 2019–20 with the EAMUS (Enhanced Ambulatory Urological Surgery) pathway, which prescribed a default of 5 opioid tablets with a median of 3 actually used and 93% patient satisfaction, his team scaled to a Mayo Clinic tri-site implementation across 20,071 patients, creating a four-tier procedure-specific guideline that reduced median morphine equivalents from 150 to 0 and refill rates from 9.4% to 6.5% with 91% guideline adherence. Extending to a men’s health subset through SMSNA (n=2,347) achieved 89.5% adherence. By 2023, a third of patients in the refinement series used zero opioids, and 78% used five or fewer tablets. In 2024, his team achieved a milestone: 91% opioid-free perineal reconstruction with 0% refills, 0 of 7 AUS patients, and 0 of 6 sling patients requiring opioids, and only 3% of patients requiring electronic medical record opioid prescribing post-operatively. “This is published, not aspirational,” Dr. Viers stated.
For major oncologic procedures, the evidence is equally compelling. In robotic prostatectomy, the MUSIC MPOP collaborative drove opioid prescription rates from 79% to 57% with pain scores unchanged and $1.6 million avoided in prescription spending; Lewicki 2025 also demonstrated that opioid prescriptions are independently associated with increased readmission. In nephrectomy, a Mayo Clinic tier-2 pathway reduced median morphine equivalents from 2,225 to 120, with ESP superior to QL superior to TAP for laparoscopic cases and QL superior in open nephrectomy RCTs; Fox Chase achieved an 81% OME reduction through EHR default modification alone. For radical cystectomy, updated ERAS Society guidelines support TAP/QL/ESP over thoracic epidural, and opioid-free anesthesia is associated with faster bowel recovery.
The Payer-Provider Story
Dr. Viers presented the MUSIC–Blue Cross Blue Shield of Michigan (BCBSM) partnership as a model for aligning clinical and financial incentives. Published in NEJM Catalyst in 2020, the pay-for-performance model added opioid stewardship as a quality metric, with practices earning incremental reimbursement for hitting prescribing targets and quality data flowing automatically from the MUSIC registry to the insurer for peer benchmarking and transparency. The result was that median morphine milligram equivalents fell from 75 to 45, refill rates dropped from 6.0% to 2.6%, opioid prescription fill rates fell from 78.6% to 56.5%, and pain scores were unchanged. Modifier 22 tied stewardship to reimbursement, generating approximately $525 per case in additional professional fees. “Aligning clinical and payer incentives,” Dr. Viers concluded, “accelerates adoption of what the evidence already supports.”
Novel Pharmacotherapy
Dr. Viers turned to suzetrigine, the first-in-class peripheral NaV1.8 sodium channel inhibitor approved by the FDA in January 2025. Its mechanism of action includes stabilizing closed-state peripheral nociceptors without crossing the blood-brain barrier, eliminating addiction risk, respiratory depression, and sedation. In the NAVIGATE 1 (abdominoplasty, n=1,118) and NAVIGATE 2 (bunionectomy, n=1,073) phase 3 trials, suzetrigine was superior to placebo. However, in both trials, it did not achieve superiority over hydrocodone/acetaminophen. An open-label 14-day study (n=256) found 83% of patients rated pain control as good, very good, or excellent. Most importantly, Dr. Viers flagged a critical gap: there are no published RCTs exist in any urologic procedure. “I hope somebody will see this as an opportunity,” he noted.
Future Directions
Figure 4: Future Directions of Urologic Perioperative Pain Management.
Dr. Viers mapped eight parallel advances poised to reshape urologic perioperative pain management. Next-generation Nav inhibitors are in phase 2 trials. Regional anesthesia is evolving with bupivacaine-meloxicam (Zynrelef). Opioid-free anesthesia combining lidocaine, dexmedetomidine, and ketamine achieves better postoperative nausea and vomiting and recovery with similar 24-hour pain scores. Novel surgical technologies are reducing pain through surgical innovation itself. Non-pharmacologic interventions, including virtual reality, music therapy, and preoperative cognitive behavioral therapy, represent what Dr. Viers called “zero-cost multipliers.”
Dr. Viers outlined seven research priorities for the field: 1) suzetrigine RCTs in urologic procedures (prostatectomy, URS, cystectomy, reconstruction), 2) multi-institutional opioid-free collaborative, 3) procedure-by-procedure head-to-head comparisons of regional block modalities (ESP vs. QL vs. TAP vs. pudendal), 4) comparator trials of multimodal pathways with versus without novel agents, 5) EHR choice-architecture implementation studies across diverse practice environments, 6) MUSIC-style 5- and 10-year long-term outcome data on persistent use, overdose, and mortality, and 7) health-equity research addressing differential access to multimodal, regional, and novel non-opioid therapies across patient populations.
The Takeaways
Dr. Viers closed with a five-move implementation checklist that every urologist could begin the next morning. First, schedule the backbone: acetaminophen 1,000 mg q6h plus ibuprofen 600 mg q6h, offset by three hours, and reject fixed-combination opioid-acetaminophen preparations. Second, block what you can: partner with anesthesia for regional blocks. Third, match pills to the case: zero is a valid default for cystoscopy, vasectomy, URS, and robotic prostatectomy. Fourth, electronic Rx for breakthrough, not prophylaxis. Lastly, the most important point: “If we don’t write it, the patient doesn’t become persistent,” Dr Viers stated. The prescription is the causal lever. The solution is in our hands.
Presented by: Boyd Viers, MD, Associate Professor of Urology, Program Director, Residency Program, Department of Urology, Mayo Clinic, Rochester, MN, USA. @boyd_viersMD
Written by: Helen Gao, Medical Student at Robert Wood Johnson Medical School, Leadership and Innovation Fellowship Training (LIFT) Scholar at Department of Urology, University of California, Irvine. @helengao295 on X during the 2026 American Urological Association Annual Meeting, May 15 – 18, 2026, Washington, DC
References:
- Brummett CM, Waljee JF, Goesling J, et al. New Persistent Opioid Use After Minor and Major Surgical Procedures in US Adults. JAMA Surg. 2017;152(6):e170504. doi:10.1001/jamasurg.2017.0504
- Bicket MC, Long JJ, Pronovost PJ, Alexander GC, Wu CL. Prescription Opioid Analgesics Commonly Unused After Surgery: A Systematic Review. JAMA Surg. 2017;152(11):1066-1071. doi:10.1001/jamasurg.2017.0831
- Berger I, Strother M, Talwar R, et al. National Variation in Opioid Prescription Fills and Long-Term Use in Opioid Naïve Patients after Urological Surgery. J Urol. 2019;202(5):1036-1043. doi:10.1097/JU.0000000000000343
- Welk B, McClure JA, Clarke C, Vogt K, Campbell J. An Opioid Prescription for Men Undergoing Minor Urologic Surgery Is Associated with an Increased Risk of New Persistent Opioid Use. Eur Urol. 2020;77(1):68-75. doi:10.1016/j.eururo.2019.08.031
- Ivan SJ, Holck HW, Robinson MM, et al. Persistent opioid and benzodiazepine use after radical cystectomy in enhanced recovery after surgery (ERAS) patients. Urol Oncol. 2023;41(10):432.e1-432.e9. doi:10.1016/j.urolonc.2023.05.022
- Alsyouf M, Farkouh A, Wood EL, et al. Opioid prescription following radical orchiectomy associated with new persistent opioid use. Urol Oncol. 2024;42(11):375.e15-375.e21. doi:10.1016/j.urolonc.2024.06.019
- Robles J, Abraham NE, Brummett C, et al. Rationale and Strategies for Reducing Urologic Post-Operative Opioid Prescribing. American Urological Association White Paper. 2021.
- Verret M, Lauzier F, Zarychanski R, et al. Perioperative Use of Gabapentinoids for the Management of Postoperative Acute Pain: A Systematic Review and Meta-analysis. Anesthesiology. 2020;133(2):265-279. doi:10.1097/ALN.0000000000003428
- Sherif H, Sebay A, Kandeel W, et al. Safety and efficacy of Intravesical hyaluronic acid/chondroitin sulfate in the treatment of refractory painful bladder syndrome. Turk J Urol. 2018;45(4):296-301. Published 2018 Nov 21. doi:10.5152/tud.2018.63600
- Grimaud LW, Peterson AC. Eulogy for B&O Suppositories: A Resident's Remembrance of Rectal Relief. Urology. 2024;191:34-35. doi:10.1016/j.urology.2024.04.044
- Hawken SR, Hiller SC, Daignault-Newton S, et al. Opioid-Free Discharge is Not Associated With Increased Unplanned Healthcare Encounters After Ureteroscopy: Results From a Statewide Quality Improvement Collaborative. Urology. 2021;158:57-65. doi:10.1016/j.urology.2021.07.037
- Pence ST, Findlay BL, Bearrick EN, et al. Evaluation of an Opioid-free Pathway for Perineal Reconstructive Surgery: A 1-year Pilot Study. Urology. 2024;190:110-114. doi:10.1016/j.urology.2024.04.032
- Findlay BL, Britton CJ, Glasgow AE, et al. Long-term Success With Diminished Opioid Prescribing After Implementation of Standardized Postoperative Opioid Prescribing Guidelines: An Interrupted Time Series Analysis. Mayo Clin Proc. 2021;96(5):1135-1146. doi:10.1016/j.mayocp.2020.10.045
- Ancker JS, Gossey JT, Nosal S, et al. Effect of an Electronic Health Record "Nudge" on Opioid Prescribing and Electronic Health Record Keystrokes in Ambulatory Care. J Gen Intern Med. 2021;36(2):430-437. doi:10.1007/s11606-020-06276-1
- Chen SL, Liu MA, Swisher MW. Suzetrigine, a selective NaV1.8 inhibitor in acute and chronic pain: mechanistic insights, clinical outcomes, and future perspectives. Curr Opin Anaesthesiol. 2026;39(2):183-187. doi:10.1097/ACO.0000000000001599
- Koo K, Winoker JS, Patel HD, et al. Evidence-Based Recommendations for Opioid Prescribing After Endourological and Minimally Invasive Urological Surgery. J Endourol. 2021;35(12):1838-1843. doi:10.1089/end.2021.0250