(UroToday.com) Dr. Ramin Nateghi presented a podium session investigating the biologic and histopathologic characteristics associated with MRI-visible and MRI-invisible clinically significant prostate cancer (csPCa) using artificial intelligence (AI)-based digital pathology analysis. While multiparametric MRI has substantially improved prostate cancer detection and risk stratification, clinically significant tumors may still evade detection despite contemporary imaging protocols. The investigators sought to better understand the tissue-level features that contribute to false-negative MRI findings.
To evaluate this question, Dr. Nateghi and colleagues applied deep learning algorithms to digitally analyze prostate biopsy slides to quantify tissue architecture and cellular composition. Two separate patient cohorts were analyzed. The first cohort included patients with unilateral MRI-visible lesions but bilateral clinically significant prostate cancer, allowing direct within-patient comparison between MRI-visible and MRI-occult tumors. The second cohort consisted of patients with false-negative MRI findings who were propensity-matched to MRI-visible controls according to age, PSA, and Gleason score.
The AI-based pathology models quantified numerous histologic variables, including benign glandular tissue, Gleason patterns, inflammatory cell density, epithelial density, connective tissue composition, malignant cellularity, and tumor extent. Statistical modeling was then performed to determine which pathologic features independently correlated with MRI visibility.
A total of 179 patients and 504 biopsy cores were analyzed in the first cohort, while the matched cohort included 124 patients and 258 biopsy cores. MRI-visible tumors demonstrated a larger tumor burden and higher cellular density compared with MRI-invisible lesions. Notably, inflammatory density was not significantly associated with MRI conspicuity, challenging prior theories suggesting prostatitis or inflammatory infiltrates may contribute substantially to false-negative MRI examinations.
Multivariable analysis further demonstrated that AI-derived cancer extent and cellularity were the strongest independent predictors of MRI visibility, whereas Gleason architectural patterns and inflammatory density were not significantly associated with lesion detectability (Table 1). These findings suggest that tumor density and overall tumor burden may play a greater role in MRI conspicuity than histologic grade alone.
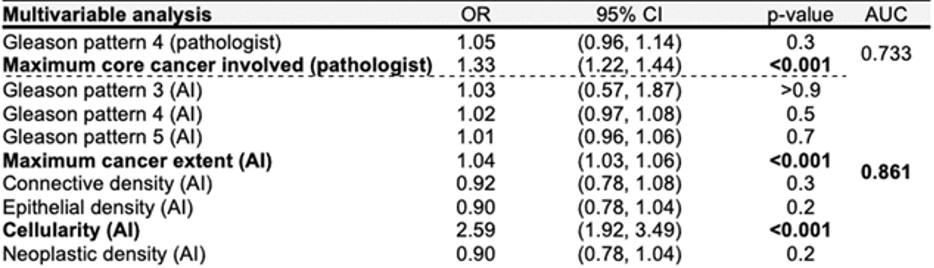
Table 1. Multivariable AI-based digital pathology analysis demonstrated that cancer extent and cellularity were independently associated with prostate MRI visibility, while inflammatory density and Gleason growth patterns were not significant predictors.
The investigators noted that these findings may help explain why certain clinically significant prostate cancers remain occult despite high-quality multiparametric MRI. MRI-invisible tumors may possess subtler tissue characteristics with lower cellular density and smaller tumor volume, reducing visibility on conventional imaging sequences.
Dr. Nateghi emphasized that future improvements in prostate cancer imaging may require optimization of diffusion-weighted imaging techniques, refinement of contrast-enhanced MRI protocols, incorporation of AI-assisted imaging analysis, or development of targeted molecular tracers capable of improving detection of MRI-occult disease.
Overall, this study highlights the growing role of AI-driven digital pathology in prostate cancer diagnostics and provides new insight into the biologic mechanisms underlying MRI-occult clinically significant disease.
During the discussion period, a moderator questioned whether reliance on biopsy specimens may have limited the analysis by potentially missing additional cancer cells present elsewhere within the prostate. In response, Dr. Nateghi explained that the investigators intentionally utilized biopsy tissue because many patients in the early stages of prostate cancer had not yet undergone definitive surgical treatment. He noted that biopsy specimens, therefore, represented the most clinically relevant and readily available tissue source for evaluating MRI-visible and MRI-invisible disease at the time of diagnosis.
Presented by: Ramin Nateghi, PhD, Postdoctoral Scholar, Northwestern University Feinberg School of Medicine, Chicago, Illinois
Written by: Ian Ong, Junior Specialist, Department of Urology, University of California, Irvine, during the 2026 American Urological Association (AUA) Annual Meeting, May 15– 18, 2026, Washington, D.C.