(UroToday.com) The 2026 American Urological Association (AUA) Annual Meeting featured a podium presentation by Dr. Fred Saad reporting prostate-specific antigen (PSA) endpoints from the phase 3 PSMAddition trial evaluating Lutetium Lu 177 vipivotide tetraxetan ([177Lu]Lu-PSMA-617) in combination with androgen deprivation therapy (ADT) and an androgen receptor pathway inhibitor (ARPI) for patients with prostate-specific membrane antigen (PSMA)-positive metastatic hormone-sensitive prostate cancer (mHSPC).
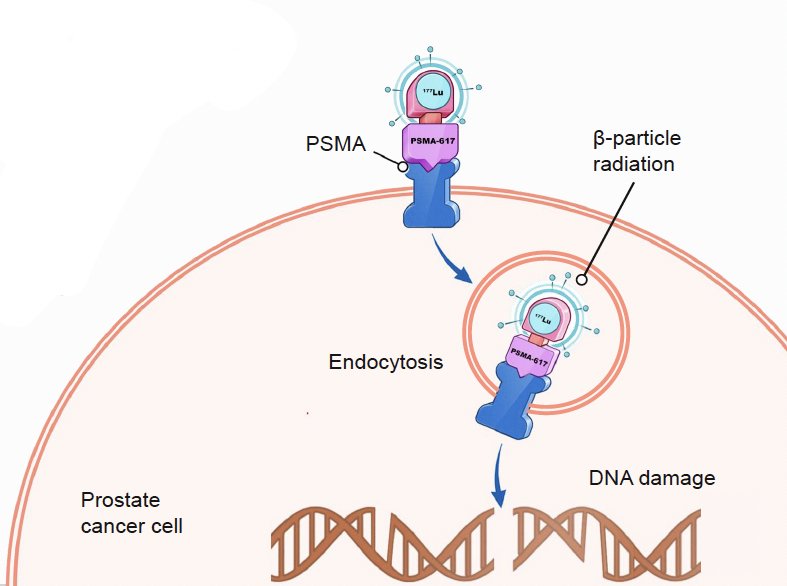
[177Lu]Lu-PSMA-617 is a targeted radioligand therapy that selectively binds PSMA-expressing tumor cells and delivers β-particle radiation, resulting in DNA damage and tumor cell death. This agent has previously demonstrated significant clinical benefit in PSMA-positive metastatic castration-resistant prostate cancer (mCRPC) in both the post-taxane VISION and taxane-naïve PSMAfore settings.1,2 PSMAddition is the first phase III trial to evaluate targeted radioligand therapy in the mHSPC setting.
PSMAddition is an international, randomized phase III trial enrolling men with mHSPC diagnosed by conventional imaging who had at least one PSMA-positive metastatic lesion on 68Ga-PSMA-11 PET/CT, were untreated or minimally treated, had ECOG performance status 0–2, and were appropriate candidates for ADT plus an ARPI. Patients were randomized 1:1 to receive six cycles of [177Lu]Lu-PSMA-617 (7.4 GBq ±10% every 6 weeks) in combination with ADT and an ARPI, or ADT plus an ARPI alone, with crossover to radioligand therapy allowed upon radiographic progression.
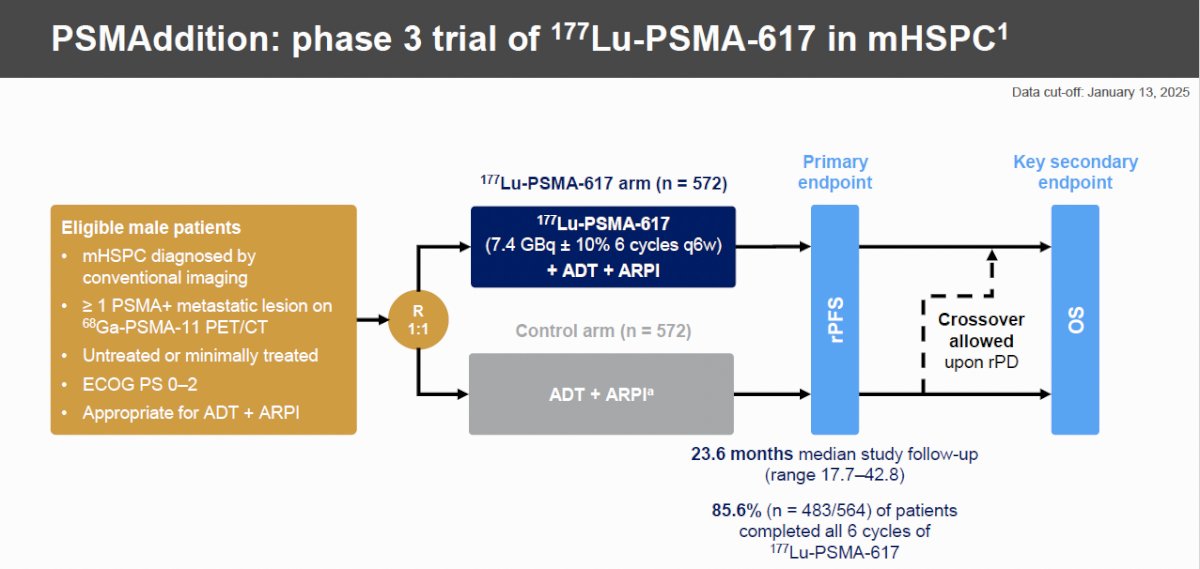
The primary endpoint was radiographic progression-free survival (rPFS), with overall survival (OS) as the key secondary endpoint. Among 1,529 patients screened, 1,420 underwent PSMA PET/CT and 1,232 (86.8%) were PSMA-positive. A total of 1,144 patients were randomized, with 572 assigned to each treatment arm. Importantly, treatment completion was excellent, with 85.6% (483/564) of patients in the experimental arm completing all six cycles of radioligand therapy.
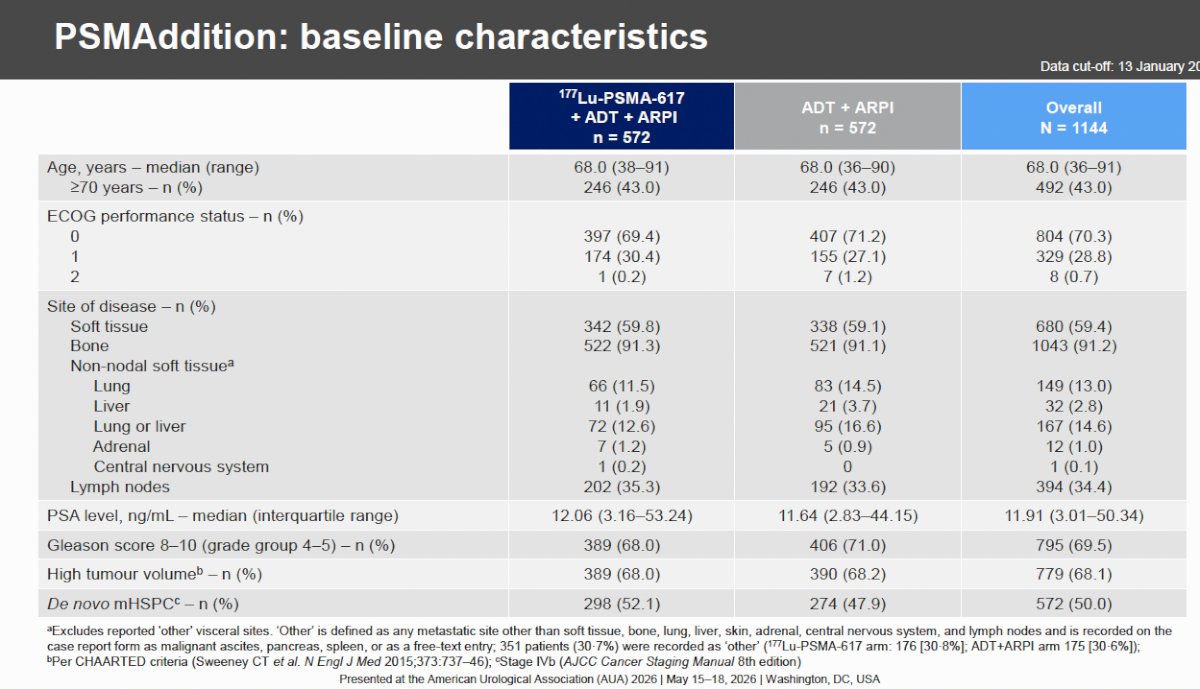
Baseline characteristics were well balanced between arms. The median age was 68 years, and 43% of patients were aged ≥70 years. ECOG performance status was 0 in 70.3%, 1 in 28.8%, and 2 in only 0.7%. Bone metastases were present in 91.2% of patients, soft tissue disease in 59.4%, lymph node involvement in 34.4%, liver metastases in 14.6%, and lung metastases in 2.8%. The median baseline PSA was 11.91 ng/mL (interquartile range [IQR] 3.01–50.34), 69.5% had Gleason score 8–10 (grade group 4–5), 68.1% had high-volume disease by CHAARTED criteria, and 50% presented with de novo metastatic disease.
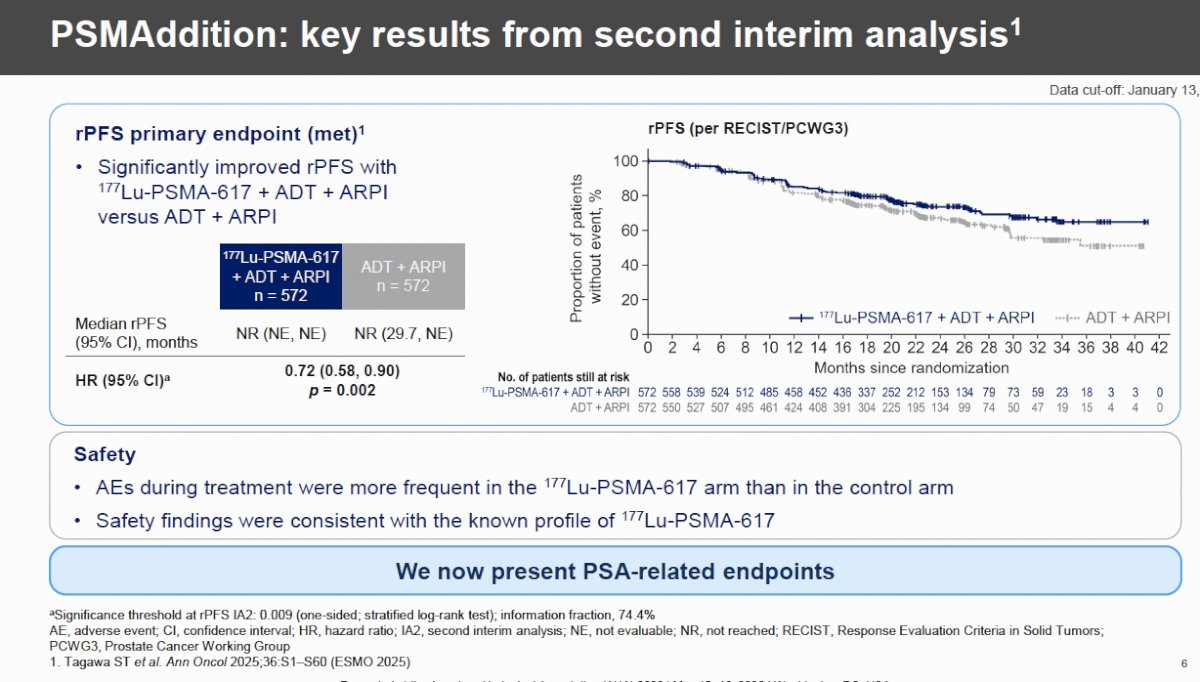
At the second interim analysis (data cutoff January 13, 2025; median follow-up 23.6 months), the trial met its primary endpoint. rPFS was significantly improved with [177Lu]Lu-PSMA-617 plus ADT and ARPI compared with ADT and ARPI alone (hazard ratio [HR] 0.72, 95% confidence interval [CI] 0.58–0.90; p=0.002). Median rPFS was not reached in either arm. Safety findings were consistent with the known toxicity profile of [177Lu]Lu-PSMA-617, although adverse events during treatment were more frequent in the radioligand arm.
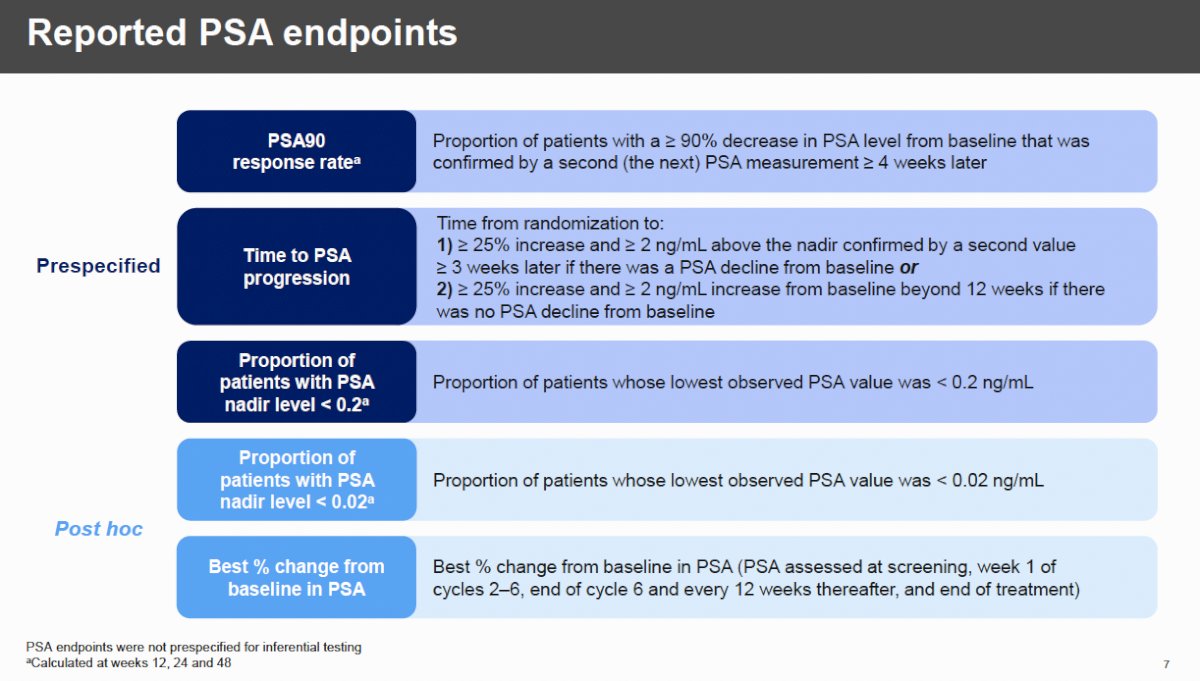
Dr. Saad then focused on PSA-based efficacy endpoints, emphasizing that although these analyses were not prespecified for formal inferential testing, they provide important insights into treatment depth and durability of response. The prespecified PSA endpoint was the proportion of patients achieving a PSA nadir <0.2 ng/mL, while post hoc analyses included PSA90 response rates, PSA nadir <0.02 ng/mL, and time to PSA progression.
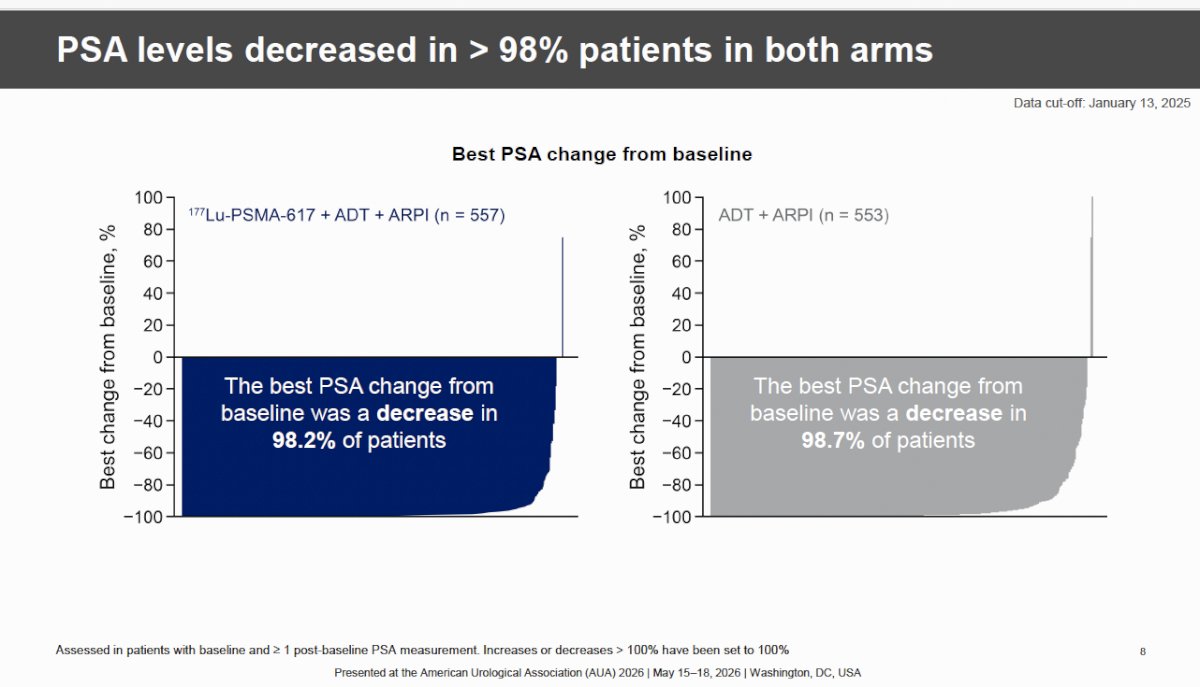
The waterfall plots below demonstrate that PSA levels declined from baseline in nearly all patients receiving either treatment strategy. Best PSA reduction from baseline was observed in 98.2% of patients treated with [177Lu]Lu-PSMA-617 plus ADT and ARPI and in 98.7% receiving ADT plus ARPI alone, highlighting the substantial activity of both regimens.
Despite similarly high rates of PSA decline, the addition of radioligand therapy resulted in deeper responses. The PSA90 response rate at any time during randomized treatment was 89.5% in the [177Lu]Lu-PSMA-617 arm compared with 85.6% in the control arm.
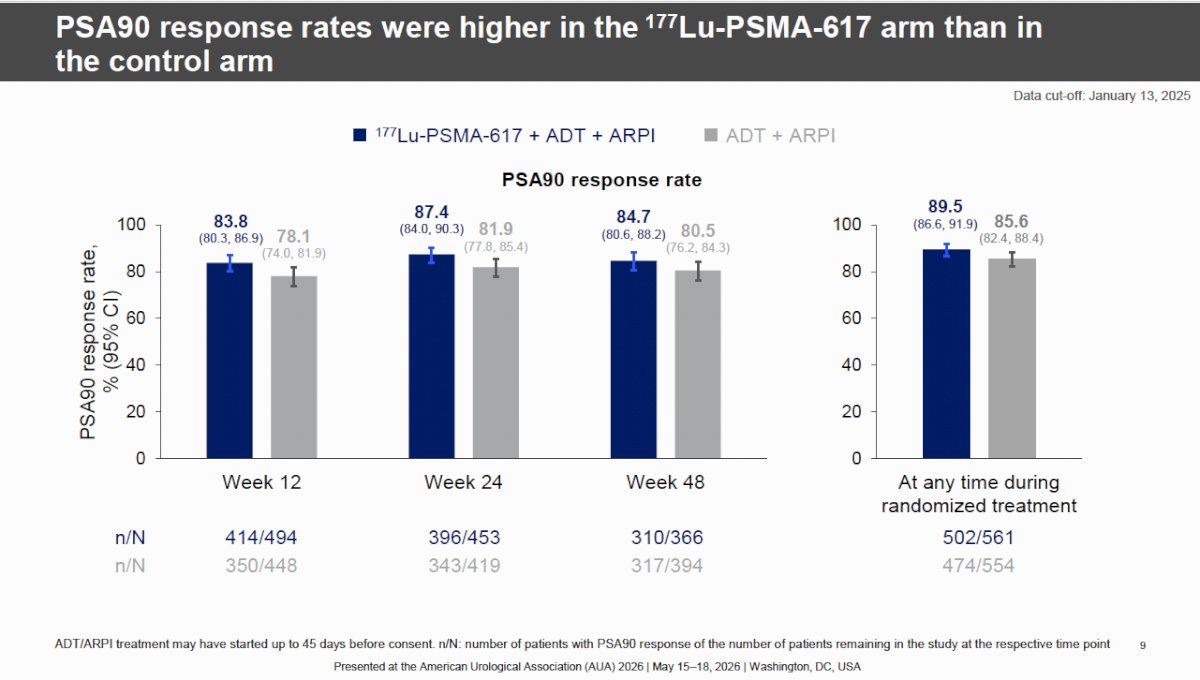
When examined longitudinally, PSA90 response rates consistently favored the radioligand arm:
- Week 12: 83.8% vs 78.1%
- Week 24: 87.4% vs 81.9%
- Week 48: 84.7% vs 80.5%
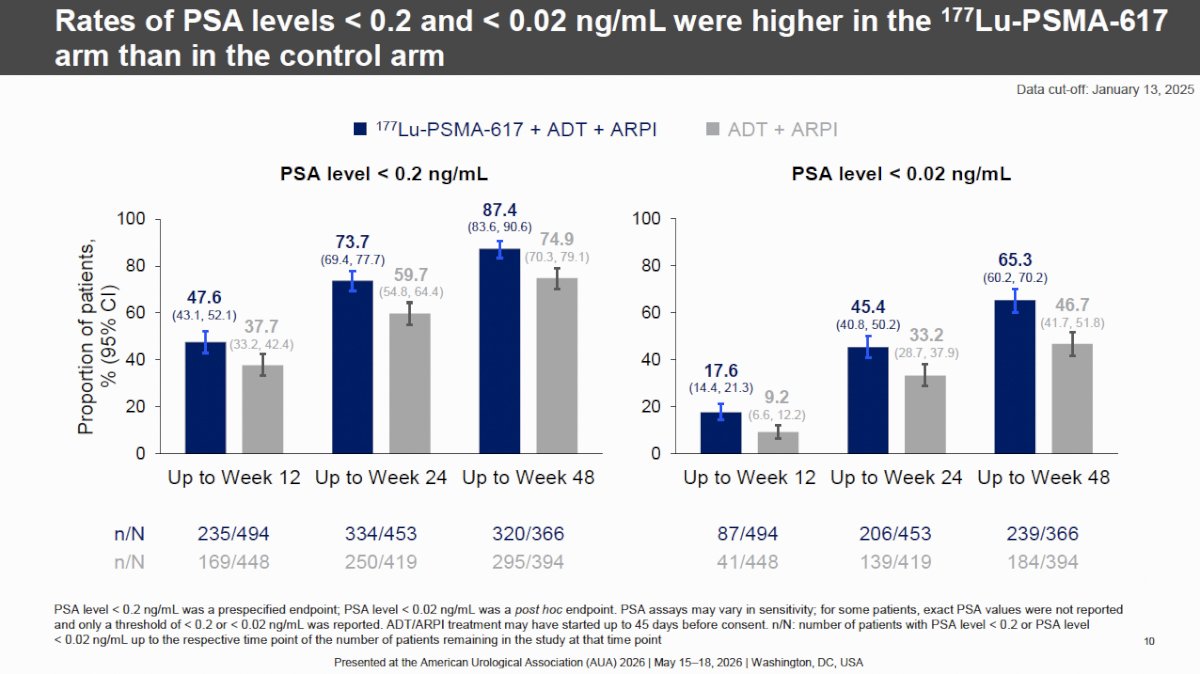
The bar graphs assessing PSA nadir thresholds showed a more pronounced advantage for the experimental arm. The proportion of patients achieving PSA <0.2 ng/mL was:
- By week 12: 47.6% vs 37.7%
- By week 24: 73.7% vs 59.7%
- By week 48: 87.4% vs 74.9%
Even more striking were rates of ultra-deep PSA suppression to <0.02 ng/mL:
- By week 12: 17.6% vs 9.2%
- By week 24: 45.4% vs 33.2%
- By week 48: 65.3% vs 46.7%
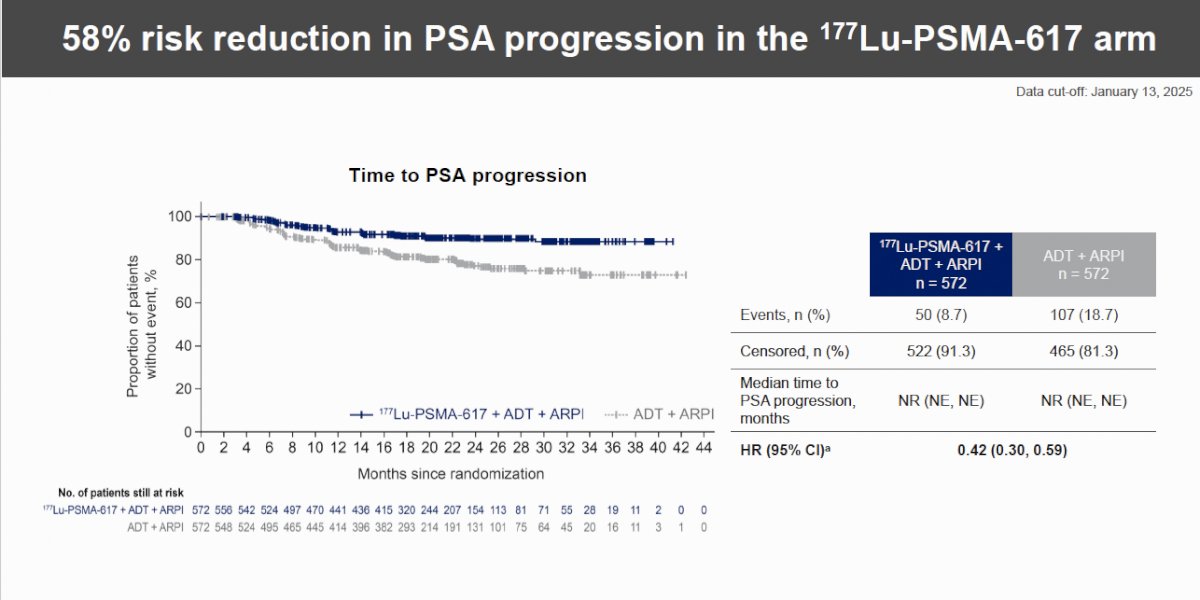
The Kaplan–Meier analysis for time to PSA progression demonstrated the most robust separation between treatment arms. Only 50 patients (8.7%) in the [177Lu]Lu-PSMA-617 group experienced PSA progression compared with 107 patients (18.7%) in the control group. Median time to PSA progression was not reached in either arm, but the addition of radioligand therapy reduced the risk of PSA progression by 58% (HR 0.42, 95% CI 0.30–0.59). The curves began to separate early and remained widely divergent throughout follow-up, with the blue treatment box beneath the graph highlighting the 36-week duration of radioligand administration.
Dr. Saad concluded as follows:
- PSA levels declined substantially in both treatment arms
- PSA levels decreased from baseline in > 98% of patients in both treatment arms
- PSA90 response rates were nominally higher in the 177Lu-PSMA-617 arm than in the control arm
- A greater proportion of patients had PSA levels < 0.2 ng/mL and < 0.02 ng/mL in the 177Lu-PSMA-617 arm than in the control arm
- The risk of PSA progression was reduced by 58% in the 177Lu-PSMA-617 arm versus the control arm
- Median time to PSA progression was not reached in either treatment arm
- Combining 177Lu-PSMA-617 with ADT + ARPI increased the frequency and depth of PSA responses, in addition to the rapid and substantial decline in PSA levels with ADT + ARPI alone
Presented by: Fred Saad, MD, FRCSC, Professor, University of Montreal Hospital Center, Montreal, Canada
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Sartor O, de Bono J, Chi KN, et al. Lutetium-177–PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021;385:1091-1103.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 Versus a Change of Androgen Receptor Pathway Inhibitor Therapy for Taxane-Naive Patients With Progressive Metastatic Castration-Resistant Prostate Cancer (PSMAfore): A Phase 3, Randomised, Controlled Trial. Lancet. 2024;403(10423):113-126.