(UroToday.com) The 2026 American Urological Association (AUA) Annual Meeting featured a poster presentation by Dr. Neal Shore evaluating real-world treatment patterns and outcomes among patients with metastatic hormone-sensitive prostate cancer (mHSPC) treated in U.S. community urology practices using the PRostatE Cancer dISease observatION (PRECISION) data platform.
The treatment landscape for mHSPC has evolved substantially over the past decade, with multiple randomized trials demonstrating improved survival with treatment intensification using androgen receptor pathway inhibitors (ARPIs) and, in selected patients, triplet therapy incorporating docetaxel. Because many patients with advanced prostate cancer in the United States initiate and continue treatment under the care of urologists, understanding real-world treatment patterns within community urology practices is of considerable clinical importance.
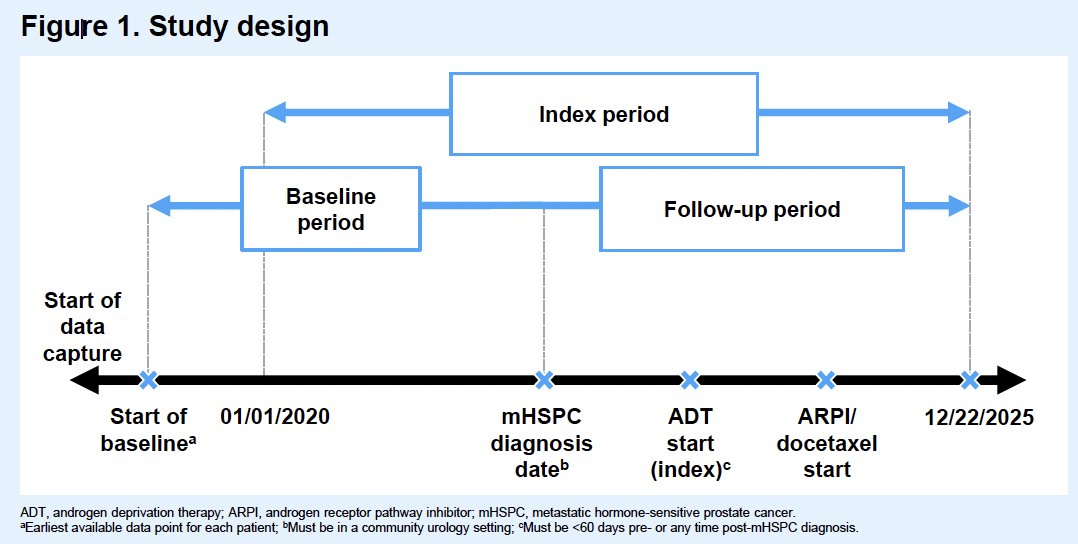
This retrospective study leveraged the PRECISION database, a large longitudinal prostate cancer dataset derived from multiple clinical settings across the United States. Eligible patients were adults diagnosed with mHSPC in community urology centers who initiated androgen deprivation therapy (ADT) within 60 days before or any time after the metastatic diagnosis date between January 1, 2020 and December 22, 2025. The ADT initiation date served as the index date. Patients were followed until development of metastatic castration-resistant prostate cancer (mCRPC), death, or last follow-up.
Treatment utilization was assessed across the entire mHSPC disease state and separately within the first four months after ADT initiation. Addition of an ARPI and/or docetaxel more than four months after index was defined as treatment intensification. Castration resistance-free survival (CRFS), defined as time to mCRPC or death, and overall survival (OS) were evaluated using Kaplan–Meier methods.
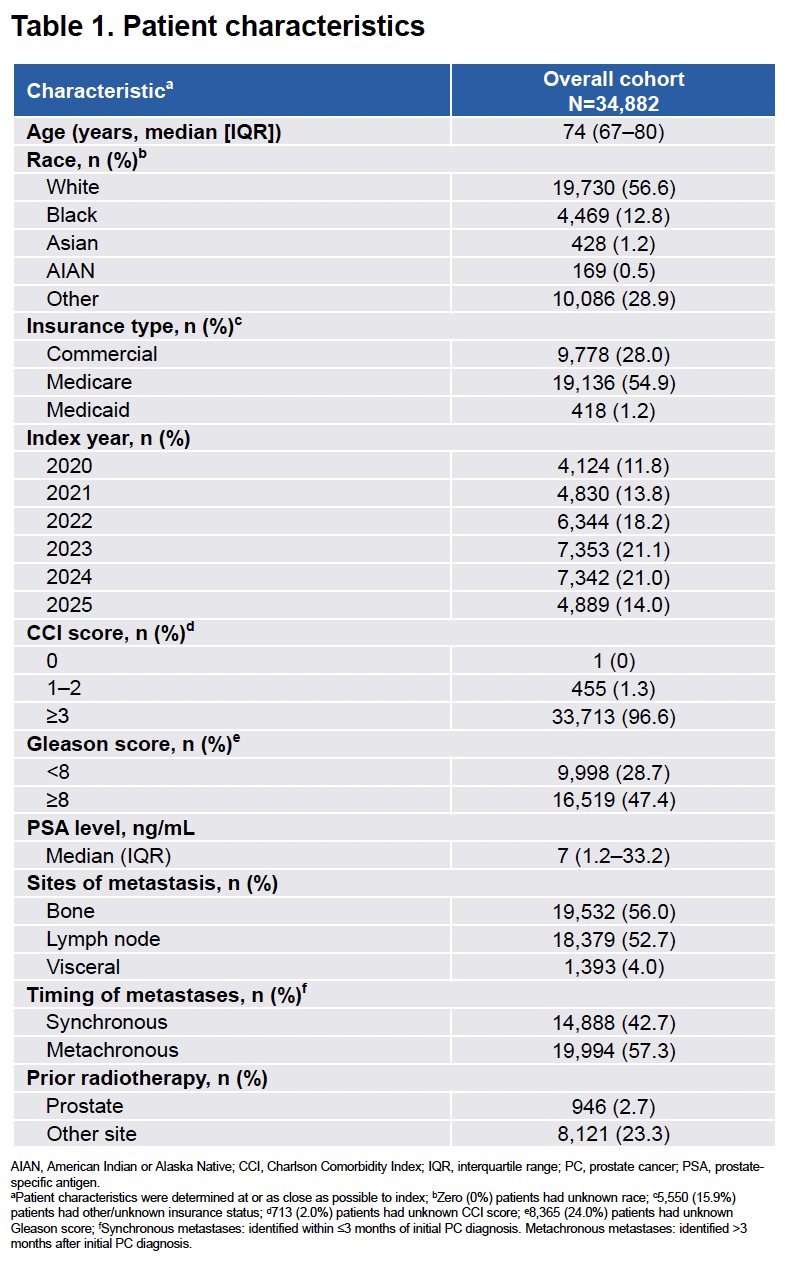
The study cohort included 34,882 patients, with a median age of 74 years (interquartile range [IQR] 67–80). Fifty-seven percent were White, 13% Black, and 55% were insured through Medicare. Nearly half of patients (47.4%) had Gleason score ≥8, and metastatic involvement most commonly included bone (56.0%) and lymph nodes (52.7%). Synchronous metastatic disease was present in 42.7%, while 57.3% developed metachronous metastases.
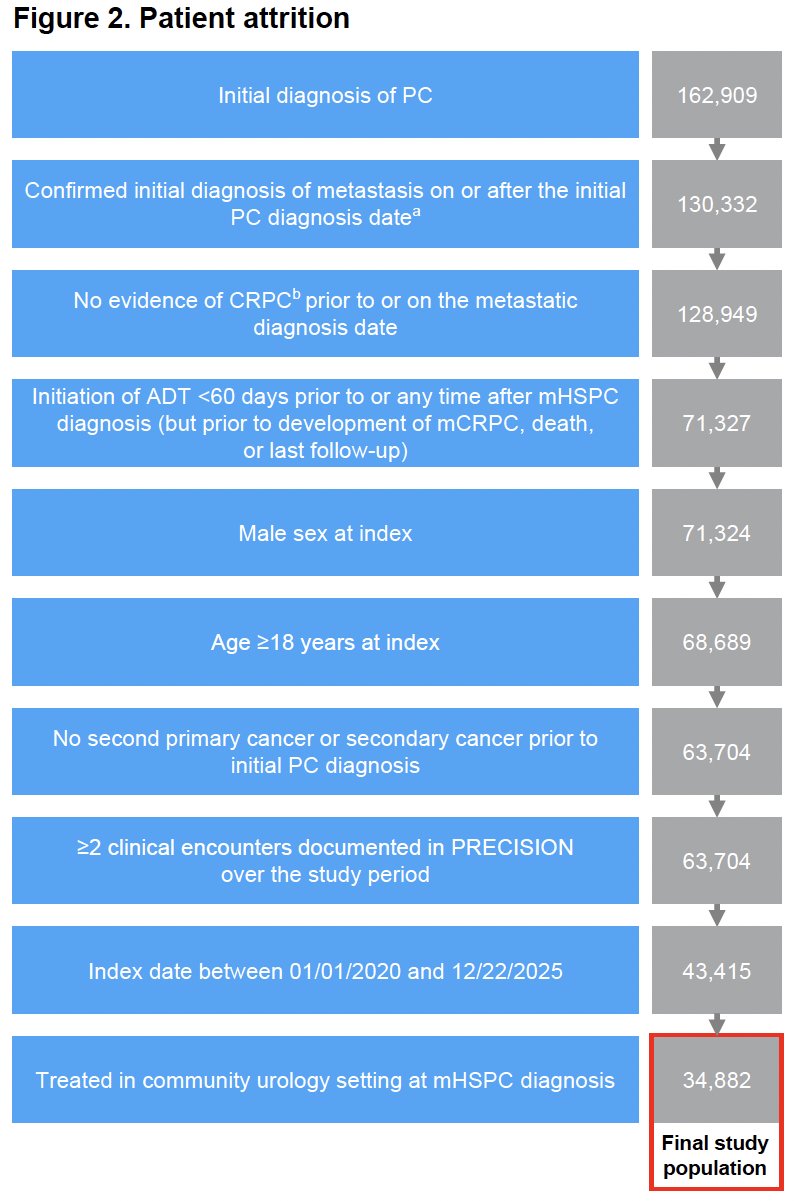
The patient attrition diagram demonstrated the scale of the PRECISION platform. Of more than 162,000 patients with an initial diagnosis of prostate cancer, sequential application of criteria including confirmed metastases, absence of prior CRPC, ADT initiation, treatment in a community urology setting, and adequate clinical encounters yielded the final analytic cohort of 34,882 patients.
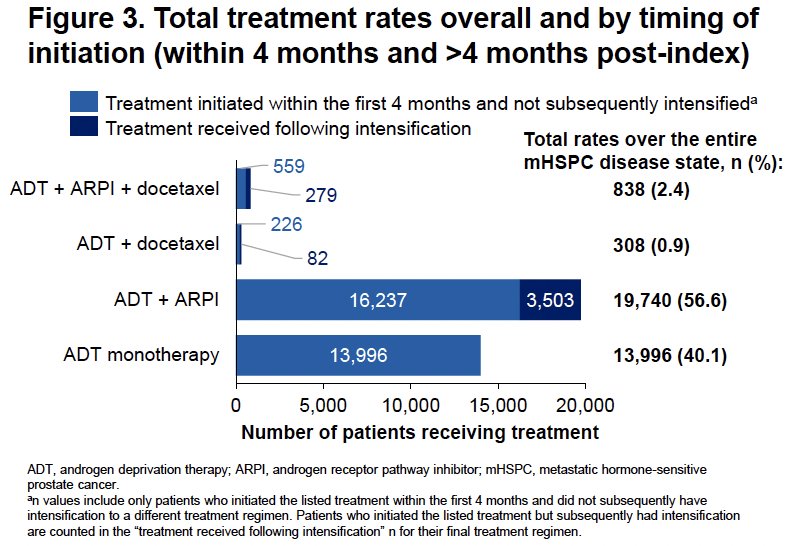
Treatment patterns revealed that ADT monotherapy remained the most common initial approach. During the first four months after index, 50.6% of patients received ADT alone, 47.8% received doublet therapy (46.9% ADT plus ARPI and 0.9% ADT plus docetaxel), and only 1.6% received triplet therapy with ADT, ARPI, and docetaxel. Among patients treated initially with ADT monotherapy, only 20.6% subsequently underwent treatment intensification, meaning that nearly 80% never received an ARPI and/or docetaxel during the mHSPC disease state.
When considering the entire mHSPC disease course, 40.1% of patients received ADT monotherapy, 57.5% received doublet therapy (56.6% ADT plus ARPI and 0.9% ADT plus docetaxel), and 2.4% ultimately received triplet therapy. The treatment utilization figure highlighted the limited adoption of triplet intensification despite contemporary evidence supporting this strategy in selected patients.
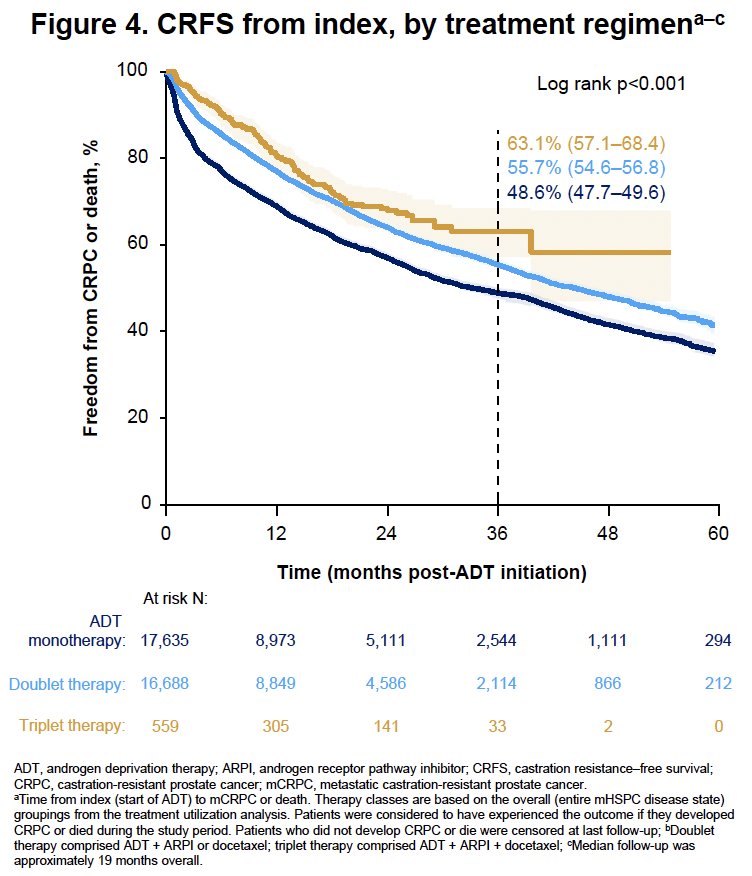
At a median follow-up of approximately 19 months, the overall median CRFS was 39.8 months (95% CI 38.6–41.1), with a 3-year CRFS rate of 52.2% (95% CI 51.4–52.9%). The Kaplan–Meier curves demonstrated significantly longer CRFS for patients receiving doublet and triplet therapy compared with ADT monotherapy (log-rank p<0.001). At three years, CRFS rates were 48.6% (95% CI 47.7–49.6%) with ADT monotherapy, 55.7% (95% CI 54.6–56.8%) with doublet therapy, and 63.1% (95% CI 57.1–68.4%) with triplet therapy.
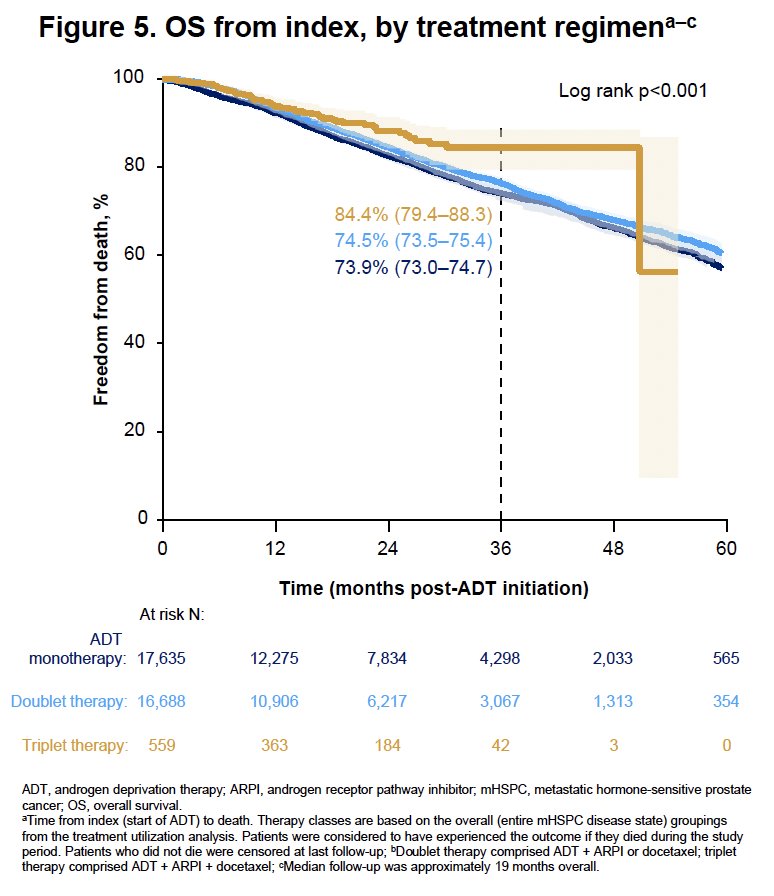
Median OS was not reached in any treatment group. The overall 3-year OS rate was 74.3% (95% CI 73.6–74.9%). The highest 3-year OS was observed among patients receiving triplet therapy at 84.4% (95% CI 79.4–88.3%), compared with 74.5% (95% CI 73.5–75.4%) for doublet therapy and 73.9% (95% CI 73.0–74.7%) for ADT monotherapy (log-rank p<0.001).
Dr. Shore concluded as follows:
- In this study focused on patients with mHSPC treated in community urology centers, ADT monotherapy was the most common initial treatment type observed
- Just over half of patients received ADT monotherapy for the first 4 months post-index, among whom 79% had no evidence of subsequent treatment intensification with ARPIs and/or docetaxel
- Both doublet and triplet regimens were associated with longer CRFS, while triplet therapy was also associated with a longer OS
- Longer follow-up is warranted to reach the median OS in all groups
- Improving the adoption of guideline-recommended combination therapies may improve outcomes among patients with mHSPC treated in community urology centers
Presented by: Neal Shore, MD, FACS, Urologist, Director, CPI, Carolina Urologic Research Center, Atlantic Urology Clinics, Myrtle Beach, SC
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.