(UroToday.com) The 2026 American Urologic Association (AUA) Annual Meeting was host to an advanced prostate cancer poster session. Dr. Alessandro Viti presented an analysis of the impact of PSMA-PET re-staging on disease classification and management for redefining EMBARK-like patients in the PSMA era.
EMBARK established the benefit of intermittent treatment intensification with enzalutamide, either with or without androgen deprivation therapy, in patients with high-risk, nonmetastatic BCR.1 However, EMBARK enrolled patients staged using conventional imaging with computed tomography and bone scans. In the contemporary era, PSMA-PET has markedly improved the detection of occult metastatic disease, raising an important question: how many “EMBARK-like” patients truly remain nonmetastatic when evaluated with molecular imaging?
To address this issue, the investigators analyzed two institutional cohorts of prostate cancer patients treated with radical prostatectomy who subsequently developed BCR. The first cohort consisted of 1,722 men staged with conventional imaging between 2010 and 2020. The second included 817 men restaged with PSMA-PET between 2016 and 2024. Patients were selected according to EMBARK criteria, defined as a PSA doubling time (PSADT) ≤9 months and a PSA level at BCR ≥1 ng/mL.
The study design leveraged the natural transition from conventional to molecular imaging to evaluate how improved staging alters both disease classification and downstream treatment recommendations.
In the conventional imaging cohort, 718 of 1,722 patients (42%) had a PSADT ≤9 months. Among these, 317 patients (18% of the entire cohort) had a PSA ≥1 ng/mL and therefore met EMBARK eligibility criteria. Median PSA in this subgroup was 2.50 ng/mL (IQR 1.36–6.50), and the median PSADT was 2.0 months (IQR 1.34–4.27). Conventional imaging identified metastatic disease in 194 of these 317 patients (61%), corresponding to 11.3% of the total conventionally staged population.
The impact of PSMA-PET was significant. In the PSMA-PET cohort, 245 of 817 patients (30%) had a pre-restaging PSA ≥1 ng/mL. Among these, only 26 patients (8%) had a PSADT ≤9 months and would therefore fulfill EMBARK criteria. These patients had a lower median PSA of 1.76 ng/mL (IQR 1.16–3.89) and a median PSADT of 2.63 months (IQR 1.56–4.63).
Of these 26 EMBARK-like patients, PSMA-PET detected positive lesions in 25 (96.2%). Importantly, only one patient (3.8%) remained truly miM0. The remaining 25 patients were upstaged to oligometastatic disease: 16 (64%) had miM1b disease, including 10 with a single bone lesion; 4 (16%) had miM1a nodal metastases; 2 (8%) had combined miM1c disease; and 3 (12%) had simultaneous miN1 and distant metastases.
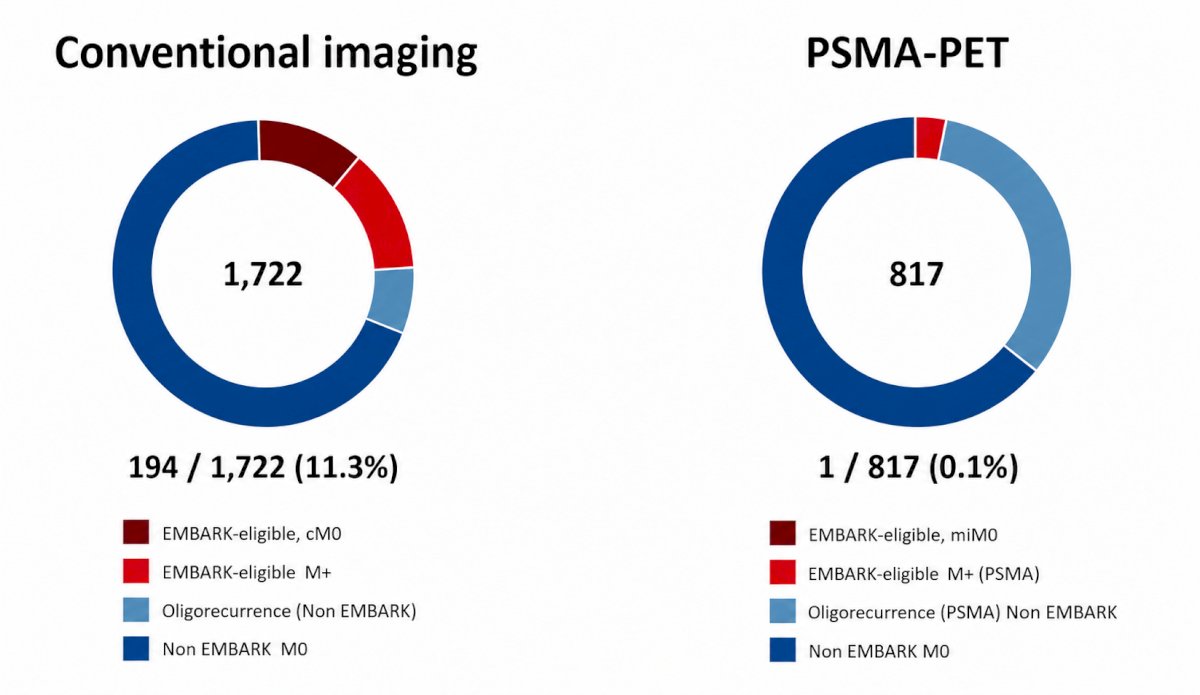
These findings are visually summarized in the central donut charts. Under conventional imaging, 194 of 1,722 patients (11.3%) would be classified as EMBARK-eligible. In contrast, when PSMA-PET was used, only 1 of 817 patients (0.1%) remained both EMBARK-eligible and molecularly nonmetastatic. Stated differently, the population of true “EMBARK-like” patients virtually disappeared in the PSMA era.
The investigators also evaluated patients who did not meet EMBARK criteria in the PSMA-PET cohort. Among 791 such patients, 268 (34%) nonetheless had oligorecurrence detected on PSMA-PET, including 46 (5.8%) with M1a nodal disease and 206 (26%) with M1b bone metastases. Of these, 186 (23%) had low-volume oligorecurrent disease, 63% received metastasis-directed therapy, and 6% received systemic treatment.
The authors concluded that in the PSMA era, EMBARK-like patients have virtually disappeared. Most men previously classified as having high-risk nonmetastatic BCR are now found to harbor metastatic disease detectable only by molecular imaging.
These findings have important clinical implications. They suggest that the traditional construct of “high-risk nonmetastatic BCR” requires fundamental reconsideration, and they support a transition toward PSMA-PET–guided management strategies that account for early oligometastatic disease rather than relying solely on conventional imaging definitions established in earlier clinical trials.
Presented by: Alessandro Viti, MD, Urology Resident, Università Vita-Salute San Raffaele, Milan, Italy
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference: